
Abstract
The CDC recommends discontinuing opportunistic infections (OIs) prophylaxis in HIV-infected patients who have CD4+ cell count >200 cells/mm3 after receiving combination antiretroviral therapy (cART). A prospective randomized controlled trial was conducted at Chiang Mai University Hospital from June 1, 2009 to January 31, 2012 in 74 adult HIV-infected patients who had received cART and had CD4+ cell count <200 cells/mm3 but plasma HIV-1 RNA<50 copies/ml. Forty-three patients (58.1%) were male and the mean age was 41.8±8.1 years; 68 (91.9%) and 59 (79.7%) patients were receiving co-trimoxazole and antifungal prophylaxis, respectively. The median CD4+ cell counts at enrollment were 142 (IQR 108, 161) and 158 (IQR 141, 176) cells/mm3 among patients who discontinued and continued OIs prophylaxis, respectively (p value=0.041). One of 37 patients (2.7%) in the discontinuation group developed Pneumocystis jiroveci pneumonia, giving the incidence rate of 1.57/1000 person-months. None of the 37 patients in the continuation group developed OIs. The difference in the prevention rates of OIs between groups was −2.7% (95% CI −7.9, 2.5). In conclusion, in the setting where plasma HIV-RNA measurement is available, e.g., Asia-Pacific region, discontinuation of prophylaxis is considerably safe in HIV-infected patients receiving cART with undetectable plasma HIV-RNA but incomplete immune recovery.
Introduction
Materials and Methods
Study design and participants
A prospective randomized controlled trial was conducted among HIV-infected patients attending the outpatient HIV Clinic, Chiang Mai University Hospital, a 1500-bed, tertiary-care Hospital in Northern Thailand, between June 1, 2009 and January 31, 2012. All patients who had documented HIV infection and met the following criteria were included: (1) age ≥18 years old, (2) receiving cART, (3) CD4+ cell count <200 cells/mm3, (4) plasma HIV-1 RNA <50 copies/mL for at least 6 months, (5) receiving primary or secondary prophylaxis for OIs caused by Pneumocystis jiroveci, Cryptococcus neoformans, Penicillium marneffei, Histoplasma capsulatum, Toxoplasma gondii, or Mycobacterium avium complex (MAC), and 6) able to give a written informed consent. The patients were excluded if they were pregnant.
Randomization and masking
JP prepared a list for randomization to either discontinue or continue primary or secondary prophylaxis in a 1:1 ratio with a block size of 6. Randomization was not stratified by any characteristics. Participants, investigators, and statistician were not masked to treatment allocation.
Procedures
Eligible and consenting patients were enrolled and randomized to either discontinue or continue primary or secondary prophylaxis. Patients were followed up at least every 6 months and were censored when they met one of the following criteria: (1) died, (2) developed any of the following OIs: PCP, cerebral toxoplasmosis, disseminated MAC, disseminated penicilliosis marneffei, disseminated histoplasmosis, and cryptococcal meningitis, (3) discontinued primary OI prophylaxis when their CD4+ cell counts were ≥200 cells/mm3 for ≥3 months or discontinued secondary OI prophylaxis when their CD4+ cell counts were ≥100–200 cells/mm3 for ≥3–6 months, or (4) when the last enrolled patient reached 1 year of follow-up.
Primary endpoint was incidence of patients who died or developed any of the following OIs: PCP, cerebral toxoplasmosis, disseminated MAC infection, disseminated penicilliosis marneffei, disseminated histoplasmosis, and cryptococcal meningitis.
Data collection included baseline characteristics (age, gender, mode of HIV transmission), clinical data (OIs prior to cART initiation, date of primary or secondary OIs prophylaxis, OIs prophylaxis medication, date of cART initiation, cART regimen, CD4+ cell count before initiating cART and every 6 months thereafter, and plasma HIV-1 RNA at 6 months after cART and every 6–12 months thereafter), and outcomes (death, date of death, occurrence of OIs after randomization, date of OIs occurrence after randomization).
cART was defined as a combination of a non-nucleoside reverse transcriptase inhibitor (NNRTI) or a protease inhibitor (PI) plus two nucleoside reverse transcriptase inhibitors (NRTI).
The study was approved by the Faculty of Medicine, Chiang Mai University Ethical Committee. This trial was registered with ClinicalTrials.gov number, NCT01392430.
Statistical analysis
The analysis was performed on an intention-to-treat basis. The comparisons of baseline characteristics between groups were performed using Chi-square or Fisher's exact test for categorical data and Student's t-test or Mann-Whitney U test for continuous data. The incidence rate was calculated by the number of events over total person-months of follow-up.
Time to the occurrence of OIs was analyzed using Kaplan-Meier estimates and log rank tests. Cox proportional hazard models were used for estimation of hazard ratios (HRs) and confidence intervals (CIs).
All statistical analyses were performed using Stata statistical software version 10.0 (Stata Statistical Software: Release 10.0, Stata Corporation, College Station, TX, 2007). All p values were two-sided. A level of significance of 0.05 was used to guide interpretation of relationships throughout the analysis.
Based on the previous studies, 8,9,12,17 –23 we estimated that after 1 year of follow-up the cumulative incidence of OIs would be 10% among patients who continued OIs prophylaxis giving the assumption of 90% prevention rate of OIs in this control group. The study was designed to demonstrate that the prevention rate of OIs in the discontinuation group was non-inferior to that in the continuation group with a margin of ten percent. A sample of 45 patients was required in each group, to demonstrate the non-inferiority at the power of 80% and the significance level of 5%.
Results
From June 1, 2009 to January 31, 2011, 74 HIV-infected patients attending the outpatient HIV Clinic at Chiang Mai University Hospital who fulfilled the inclusion criteria were enrolled to the study (Fig. 1). The enrollment rate was slowing down through the end of study period due to the increase in number of HIV-infected individuals who accessed to cART at higher CD4+ cell counts in the region. After the enrollment of the 74th participant on January 13, 2011, no participant was enrolled during the 12-month period until January 2012. The study team considered that it was unlikely to enroll additional 16 participants to meet the enrollment target; therefore, the study team decided to end the study on January 31, 2012 due to the futility reason. No patient died during the total follow-up of 1210.5 person-months and median duration of 16.6 months. Twenty-eight patients discontinued primary OI prophylaxis when their CD4+ cell counts were ≥200 cells/mm3 for ≥3 months, and 29 discontinued secondary OI prophylaxis when their CD4+ cell counts were ≥100–200 cells/mm3 for ≥3–6 months. Sixteen patients (7 in the discontinuation group and 9 in the continuation group) were followed up until the end of study period.
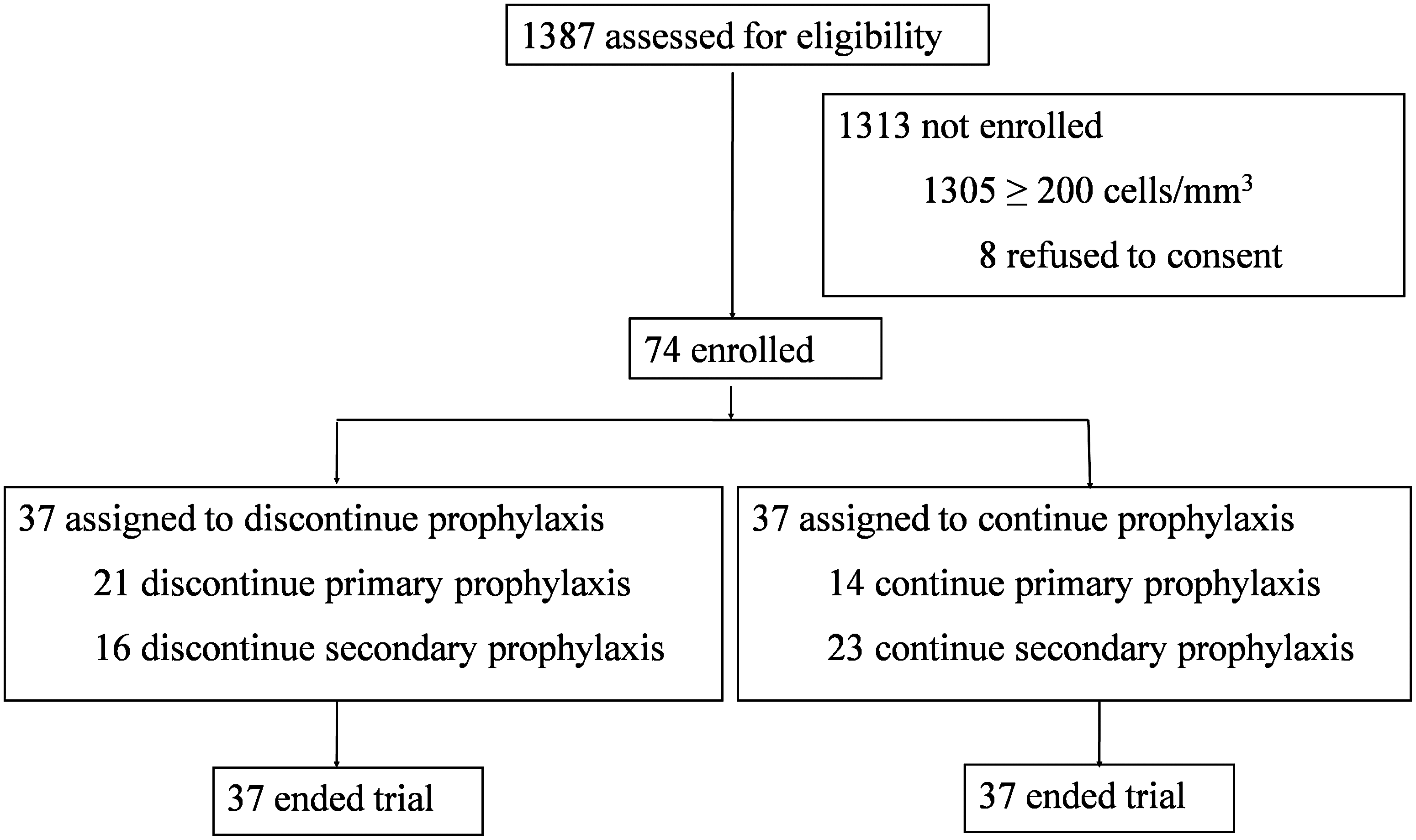
Flow chart of the study participants.
Baseline characteristics
Among the 74 patients enrolled to the study, 37 patients each were randomly assigned to the discontinuation and continuation groups. Forty-three patients (58.1%) were male and the mean age was 41.8±8.1years. Thirty-five patients (47.3%) received primary prophylaxis. Thirty-nine patients (52.7%) received secondary prophylaxis: 20 patients for PCP, 5 for penicilliosis marneffei, 5 for cryptococcal meningitis, 4 for PCP and cryptococcal meningitis, 2 for histoplasmosis, 1 for cerebral toxoplasmosis, 1 for PCP and penicilliosis marneffei, and 1 for PCP, cryptoccocal meningitis, and cerebral toxoplasmosis. Sixty-eight patients (91.8%) received co-trimoxazole, 49 patients (66.2%) received fluconazole, 11 patients (14.9%) received azithromycin, 10 patients (13.5%) received itraconazole, and 9 patients (12.2%) received dapsone. The median CD4+ cell counts at enrollment were 158 (IQR 141, 176) and 142 (IQR 108, 161) cells/mm3 among discontinuation and continuation groups, respectively. The comparisons of baseline characteristics between groups are shown in Table 1. Overall, the baseline characteristics were similar between groups, except the discontinuation group had slightly but significantly lower CD4+ cell counts and shorter duration on cART at baseline.
cART, combination antiretroviral therapy, NRTI, non-nucleoside reverse transcriptase inhibitor.
Incidence of opportunistic infections
The median follow-up duration after randomization was 67 weeks (IQR 28, 98) among patients who discontinued OIs prophylaxis and 80 weeks (IQR 35, 112) among those who continued OIs prophylaxis (p=0.446). The total follow-up duration in the discontinuation group was 636 person-months; 1 patient (2.7%) developed PCP 163 days after randomization at a CD4+ cell count of 158 cells/mm3, giving the incidence rate of 1.57/1000 person-months (95% CI 0.22, 11.16/1000 person-months). The total follow-up duration in the continuation group was 574 person-months; no patients developed opportunistic infections. The probability for development of opportunistic infections did not differ between groups as shown in Fig. 2 (log-rank test, p=0.355).
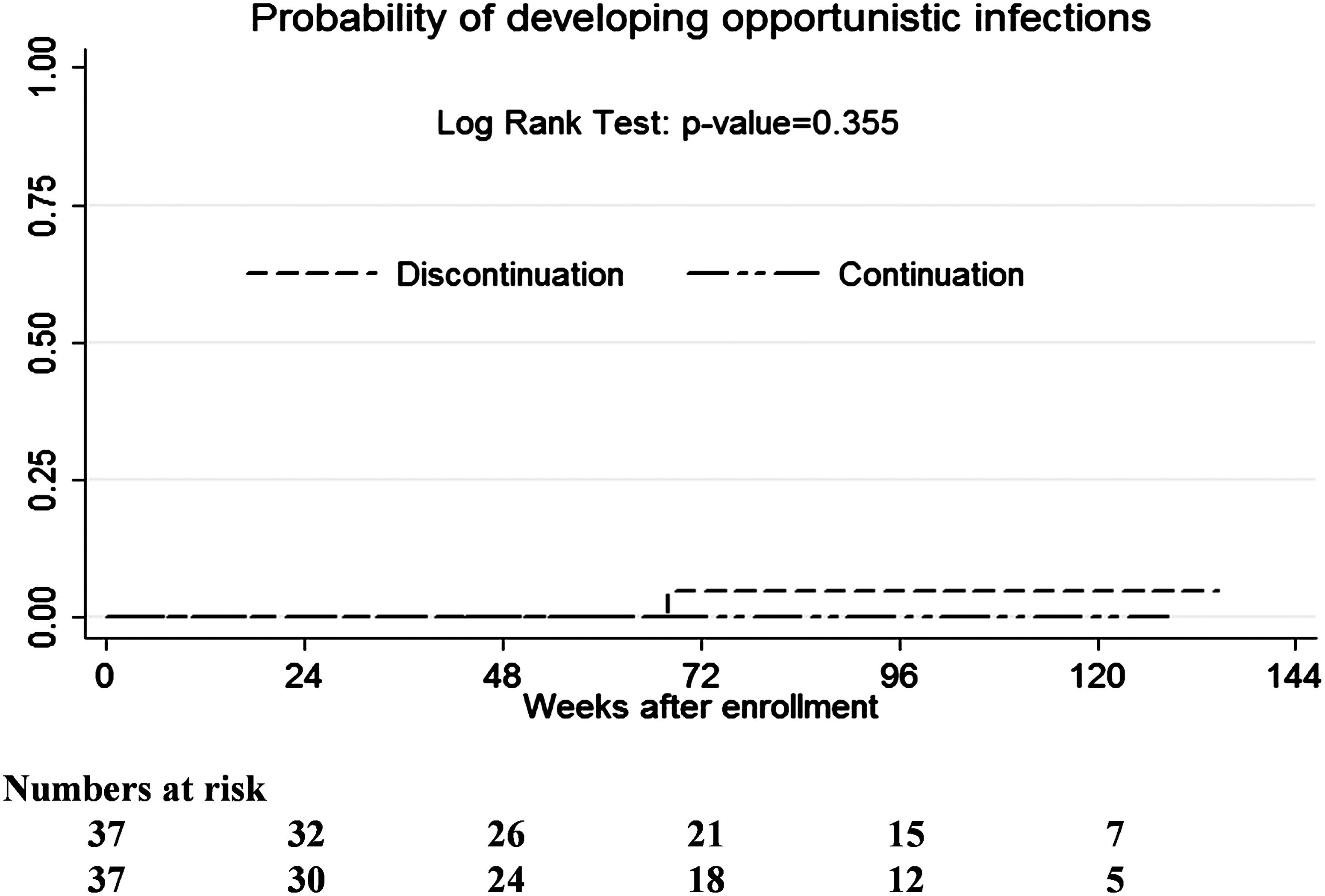
Probability of developing opportunistic infections among patients who discontinued and continued primary or secondary prophylaxis.
The cumulative incidence of opportunistic infections among patients who discontinued OI prophylaxis was 2.7% giving the prevention rate of 97.3% whereas that of the continuation group was 100%. The difference in the prevention rates of OIs between groups was −2.7% (95% CI −7.9, 2.5).
Discussion
Antiretroviral therapy restores immune function primarily by an increment of CD4+ cell count. Observational and randomized controlled trials have demonstrated that discontinuation of prophylaxis for several OIs was safe in patients who received cART and achieved undetectable plasma HIV-1 RNA with sustained increase of CD4+ cell count above certain levels; for example, ≥200 cells/mm3 for PCP, and ≥100 cells/mm3 for penicilliosis marneffei and cryptococcal meningitis. 7 –9,13,14,24 –26 Question is raised whether the prophylaxis of OIs can be discontinued if the patients had suppressible HIV-1 RNA but failed to achieve adequate immune recovery. Several studies reported the association between a lower plasma HIV-1 RNA and a decreased risk of developing OIs regardless of CD4+ cell count. 27 –29 Two observational studies showed that the risk of developing OIs decreases when plasma HIV-1 RNA was fully suppressed even with incomplete CD4+ cell recovery. 16,30 Our study, although with a small number of sample size, is the first prospective randomized controlled study to determine the safety of discontinuation of OIs prophylaxis in patients who had CD4+ cell count <200 cells/mm3 but undetectable plasma HIV-1 RNA; all patients received PCP prophylaxis and almost 80% received antifungal prophylaxis. We found that the incidence rate of PCP in the discontinuation group was 1.57/1000 person-months. The protection rates of OIs in the discontinuation and continuation groups were 97.3% and 100%, respectively, giving the difference in protection rate of −2.7% (95% CI −7.9, 2.5). The −7.9% lower bound of 95% CI met the pre-defined criteria for non-inferiority between discontinuation and continuation groups. However, based on the small sample size, we estimated the power of 70% to determine the statistical significance.
Our study has strength over previous studies in that it aimed at multiple OIs at the same time while others addressed only one specific OI. In our study, more than half of the participants received secondary prophylaxis. The common OIs in our population included PCP, penicilliosis marneffei, cryptococcal meningitis, histoplasmosis, and cerebral toxoplasmosis; many participants had multiple episodes of OIs. The results of this study may have clinical implication in the resource limited setting where the occurrence of multiple OIs is more common than in the developed countries. However, our study does have several limitations. First, the study was at a single site and the number of sample size was smaller than what was planned. A multi-center study may be needed to ensure an adequate sample size for the non-inferiority trial. Second, there were slight but significant imbalances between groups in our study. Patients who discontinued prophylaxis had lower CD4+ cell count (p=0.04) and shorter duration on cART before randomization (p=0.025) than those who continued prophylaxis. This is most likely by chance particularly with a small sample size. However, these imbalances favor the control group thus having no effect on the final interpretation. Again, a multi-center study may be necessary to adequately address a statistical power and significance as well as a strong evidence to confidently change the practice guidelines.
In conclusion, our study, in addition to the previous observational studies, supports that in the setting where plasma HIV-RNA measurement is available (e.g., Asia-Pacific region), discontinuation of OI prophylaxis is considerably safe in HIV-infected patients receiving cART with undetectable plasma HIV-RNA but incomplete immune recovery. However, the power to detect the statistical difference might be low due to the small sample size and small number of events.
Footnotes
Acknowledgments
We wish to thank the National Research University Project under Thailand's Office of the Higher Education Commission for financial support. The sponsor did not have a role in study design, data analysis, data interpretation, or drafting the article.
The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. RC participated in trial design, data analysis, data interpretation, and drafted the article. JP participated in patient randomization and data collection. NN and WK participated in patient recruitment. KS participated in trial design, data interpretation, and revised article critically for important intellectual content. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.