
Abstract
Promoting HIV medication adherence is basic to HIV/AIDS clinical care and reducing transmission risk and requires sound assessment of adherence and risk behaviors such as substance use that may interfere with adherence. The present study evaluated the utility of a telephone-based Interactive Voice Response self-monitoring (IVR SM) system to assess prospectively daily HIV medication adherence and its correlates among rural substance users living with HIV/AIDS. Community-dwelling patients (27 men, 17 women) recruited from a non-profit HIV medical clinic in rural Alabama reported daily medication adherence, substance use, and sexual practices for up to 10 weeks. Daily IVR reports of adherence were compared with short-term IVR-based recall reports over 4- and 7-day intervals. Daily IVR reports were positively correlated with both recall measures over matched intervals. However, 7-day recall yielded higher adherence claims compared to the more contemporaneous daily IVR and 4-day recall measures suggestive of a social desirability bias over the longer reporting period. Nearly one-third of participants (32%) reported adherence rates below the optimal rate of 95% (range=0–100%). Higher IVR-reported daily medication adherence was associated with lower baseline substance use, shorter duration of HIV/AIDS medical care, and higher IVR utilization. IVR SM appears to be a useful telehealth tool for monitoring medication adherence and identifying patients with suboptimal adherence between clinic visits and can help address geographic barriers to care among disadvantaged, rural adults living with HIV/AIDS.
Introduction
A variety of techniques have been used to monitor adherence, including pill counts, medication records, laboratory markers, medication event monitoring systems, and verbal report measures. 3,4 No single reporting system is universally agreed upon as best, and all have strengths and weaknesses. Nevertheless, verbal report measures correlate well with laboratory markers of adherence and are less time- and resource-intensive than many other data collection methods. 4,5 Debate continues, however, about necessary time frames for obtaining accurate adherence reports that can provide clinically meaningful data, (e.g., retrospective assessment over short intervals of 3–4 days appears to be accurate), 5,6 but longer intervals that provide more data points may have greater utility for monitoring and promoting adherence. Despite the need for extended adherence monitoring in HIV care, lengthy retrospective reports that require patients to summarize behavior over many days, weeks, or months risk inaccuracies due to normal forgetting or recall biases (e.g., over-/under-reporting due to the social desirability/undesirability of reported behaviors). Daily prospective assessment over lengthy intervals resolves these concerns, but raises other questions about convenience and utilization by patients with chronic conditions like HIV/AIDS.
Another limitation of available research is that most HIV adherence studies have been conducted in coastal urban centers, and few have taken place in the rural Deep South where the HIV epidemic is now disproportionately concentrated. 7,8 The rural South has been particularly hard hit and is home to two-thirds of the nation's non-metropolitan cases of HIV/AIDS. 9 The region is culturally distinct from much of the United States, including its political conservatism, history of racial inequality, and heightened stigma surrounding HIV disease. 10 Rural Southerners living with HIV/AIDS face barriers to receipt and optimal utilization of HIV care related to geographic distance from care, inadequate access to health infrastructure and insurance, and a shortage of health care personnel and services. 8,11 –13
Therefore, innovative measurement approaches are needed to reach and assess these geographically isolated, resource-poor populations. Telephone-based Interactive Voice Response (IVR) systems offer an under-utilized technology for monitoring HIV-related behaviors, including medication adherence. IVR systems can support efficient patient monitoring over long intervals and distances, assisting stepped care when indicated, and allowing event-level examination of temporal sequences of HIV risk and protective behaviors. 14 Although not universally appealing, IVR users tend to find IVR applications acceptable and easy to use and often provide more complete IVR reports of sensitive behaviors compared to face-to-face interviews. 15,16
Potential limitations of IVR applications include system start-up and maintenance costs (e.g., financial resources required for implementation, computer infrastructure, programming), data confidentiality protections, and the additional burden IVR reporting may place on patients engaged in complex medication regimens like antiretroviral pharmacotherapy (ARV). 19,29 But such patients are precisely the target population who will benefit from ongoing ambulatory monitoring. Furthermore, once operational, IVR systems tend to recoup initial investment costs; this will continue to be the case as the medical profession moves forward with Electronic Medical Records (EMR) systems and the infrastructure necessary to power them. If IVR protocols are properly written with clear, simple response options and branch and skip patterns depending on patient responses, the added burden on patients is minimized, and daily assessment can be brief (2–5 min or less).
Self-monitoring (SM) using an IVR platform has been employed successfully to measure health-related behaviors, including substance use and sexual risk behaviors 17,18 and to promote adherence to medication regimens for chronic health concerns such as obesity, diabetes, and depression. 19 However, the few studies that have used IVR systems to assess or promote medication adherence employed international samples that limit generalization to IVR applications in the rural South. 20,21 Other studies have piloted cell phone-based interventions to measure and increase ARV medication adherence. Text-message reminders were found superior to beeper reminders, 22 and unannounced biweekly pill counts with counseling via cell phone increased adherence more so than unannounced biweekly pill counts alone. 23 Both studies were conducted in urban areas, and neither engaged participants in IVR SM.
Given the measurement advantages of IVR SM to obtain real-time reports of HIV-related behaviors, the present study used an IVR system to obtain daily verbal reports of HIV medication adherence, substance use, and other HIV risk behaviors in Deep South rural patients living with HIV/AIDS. Participants were taking medication for HIV disease, were sexually active, and reported recent substance use, which has been associated with medication nonadherence and other HIV-related risk-taking. 24,25 They received IVR access for daily reporting of medication adherence, alcohol and drug use, and sexual activity for up to 70 days.
The present data analyses had two main goals: (1) Concordance between daily IVR, 4-day, and 7-day recall reports of medication adherence was evaluated to determine whether daily IVR reports differed from better studied short-term recall measures. 5,6 Daily IVR assessment of socially undesirable risk behaviors typically yields higher reports than recall measures and is presumably more accurate. 15,16 The opposite result may be found for desirable protective behaviors such as medication adherence. Thus, higher participant reports of adherence were predicted for the recall measures compared to daily IVR reports, particularly the longer 7-day recall that is subject to greater risk of reporting inaccuracies. (2) Predictors of medication nonadherence (e.g., substance use) were examined using prospective IVR reports to determine if predictive relationships established using retrospective measures were replicated using near real-time daily reports.
Methods
Sample characteristics
The study received Institutional Review Board approval and a federal Certificate of Confidentiality. HIV medical care patients were recruited from a nonprofit HIV clinic in rural northeastern Alabama. Eligibility criteria included: (1) age ≥19 years, the age of majority in Alabama; (2) any partner sexual activity and alcohol or illicit drug use within the past 3 months, in order to obtain sexually active substance users living with HIV/AIDS, the high risk target population for HIV risk reduction programs; (3) no health problems precluding participation (e.g., dementia); and (4) daily phone access. The behavioral risk eligibility criteria were deliberately inclusive based on any reported recent sexual activity or substance use because the reports were obtained at screening before rapport was established with participants, which might contribute to under-reporting, and because any episode of unsafe sex entails HIV transmission risk and any substance use may promote unsafe sex.
Of 109 screened respondents, 59 met all eligibility criteria, and 50 were ineligible due to not reporting recent HIV risk behaviors (15 no sex, 18 no drug use, 17 no sex or drug use). Of those eligible, 91.5% (54/59) were enrolled either in an initial pilot study to finalize procedures that involved up to 28 days of IVR reporting (n=8), or in the main study that involved up to 70 days of IVR reporting (n=46); 8.5% (5/59) declined to participate. 18 Of the 54 eligible patients who were consented and enrolled, 44 provided some IVR data and were included in the present analyses. Callers and noncallers did not differ significantly on demographic characteristics, baseline substance use, and sexual practices, although callers did have a longer duration of HIV medical care. 18 As presented in Table 1, the sample of callers was 61% male, 43% African-American, and disadvantaged socio-economically. Sample demographics were similar to statewide statistics, although percentages of males and African-Americans living with HIV/AIDS in Alabama are somewhat higher (71.6% and 65.2%, respectively). 26 Most participants were unemployed, unmarried, and heterosexual, although a minority was variously lesbian, gay, bisexual, or questioning. ARV medication regimens during the data collection interval (2/9/2007 to 6/30/2008) consisted primarily of tenofovir + emtricitabine (Truvada), supplemented with efavirenz or atazanavir.
Viral load is an index of HIV nucleic acid used to monitor HIV disease and guide treatment; values <40 copies/mL are considered “undetectable.” CD4 is a measure of immune system function; CDC categorizes values <200 as AIDS. bBaseline Timeline Followback Interview. cDays with participant reports of sexual activity with multiple or anonymous partners, substance use before or during sex, unprotected sex, or exchange of money or goods for sex.
Procedures
Procedures summarized here are detailed in earlier publications, 15,18 including measure characteristics, reliability, and validity. Baseline interviews (1.5–2.0 h) assessed risk behaviors during the past 3 months and verified eligibility. Eligible participants were enrolled in either an initial pilot study that offered 28 days of IVR SM (n=8) or in the main study that offered 70 days of IVR SM (n=46); 6/8 pilot and 38/46 main study participants accessed the IVR and provided some IVR data. Methods in the pilot and main studies were very similar except for the length of the IVR interval, and data were therefore combined for analysis. An expanded Timeline Followback (TLFB) interview assessed alcohol and drug use, 27 sexual behaviors, 26 and predictors of risk behaviors (e.g., time perspective, HIV-related self-efficacy expectations) using established questionnaires. 28,29 Participants received IVR training, and then had IVR access for 4 or 10 weeks. They received $35 university-issued Visa™ gift cards for baseline interviews and training.
IVR self-monitoring
Participants were assigned a personal identification number to access the toll-free IVR system. The system was programmed using commercial software (SmartQ Version 5(5.0.141), Telesage, Chapel Hill, NC). The daily IVR survey assessed whether participants took all prescribed HIV medications the preceding day (defined as the 24-h period midnight-to-midnight yesterday). The daily IVR survey also asked whether participants drank alcohol or used drugs to get high on the preceding day and whether they had sexual activity that day. If sex was reported, additional questions asked about the type of activity (anal, oral, or vaginal sex queried separately), type of partner for each sex act (main, non-main, anonymous), other sexual risk behaviors (sexual exchange for money/goods; drug/alcohol use before or during sex), and protective behaviors (barrier protection use).
The weekly survey asked about weekly income and noncash assets received and medical care obtained. It also included recall checks on daily reports of medication adherence during the past week. Participants were asked how many days during the week they missed taking any of their HIV medications (0–7 days), which corresponded with the daily IVR adherence assessment. An additional IVR-administered short-term recall adherence scale 6 asked participants to recall how many days during the past 4 days they missed or took only part of a dose.
Daily and weekly IVR surveys averaged <5 min each. To promote IVR utilization, participants accrued modestly reimbursed points for call completion using an “electronic bank”. 31 They received $0.50 for each daily call and $1.00 after seven consecutive calls; bonus payments stopped when a call was missed, were reinstated after another seven consecutive calls, and so forth. Among those who called the IVR at least once, pilot and main study participant earnings averaged $20 (range=$3–43) and $41 (range=$3–103.50), respectively.
Data analysis
Daily and weekly IVR reports of medication adherence were matched in time for each participant. Because the numbers of matched data points varied across participants, analyses were based on the percentage of matched observation days for each measure that involved full adherence. For the daily and weekly time-matched reports, data points were averaged across reports for each participant for the IVR daily, 7-day recall, and 4-day recall of days involving full HIV medication adherence. Reliability analyses included only participants who had ≥10 daily IVR reporting days and ≥2 weeks of weekly reports; these cutpoints were chosen in order have sufficient observation pairs for each measure to evaluate statistically the concordance of daily and weekly reports. Pearson product-moment correlations were computed across participants using the aggregated, 4- and 7-day recall reports in order to evaluate the reliability of the adherence reports. Dependent samples t-tests evaluated whether the measures yielded significantly different adherence estimates based on matched observation intervals. Pearson correlations between the IVR-reported percentages of daily medication adherence (0–100%) and baseline demographic and substance use variables evaluated associations with overall adherence.
Results
IVR utilization
As reported in prior publications, 17,18 10 of 54 participants (2 pilot, 8 main study participants) did not start the IVR task (“noncallers”). Of the 44 participants who provided some IVR reports (“callers”), the mean percentage of IVR call days was 61.6% (SD=33.7), and the median was 65.7% (Fig. 1). The mean percentage of scheduled IVR weekly recall reports was 50.5% (SD=31.3, median=50.0). Callers had received HIV-related medical care for more years (M=7.30, SD=5.15) than noncallers (M=3.30, SD=3.65; p=0.025). 18
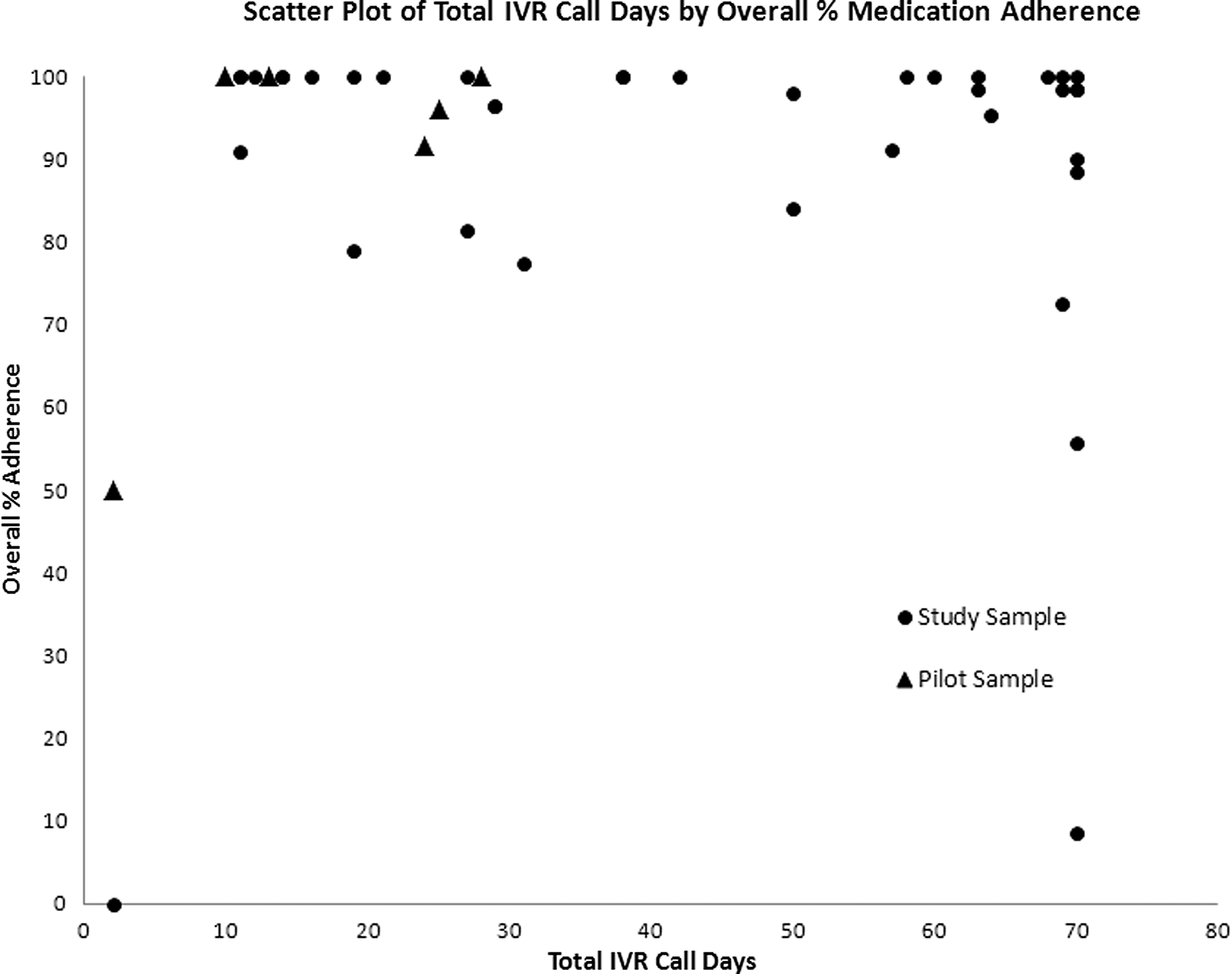
Scatter plot of total IVR call days as a function of the percentage of call days with reports of full adherence with prescribed antiretroviral medications the preceding day over the 28- to 70-day self-monitoring intervals. The x-axis shows call days for each of the 6 pilot and 38 main study IVR callers, and the y-axis is the percentage of reporting days involving full adherence (0–100% of calls).
Callers also had higher self-efficacy for negotiating safer sex as assessed by the Semple et al. scale 28 (M=3.52, SD=0.70) than noncallers (M=2.86, SD=0.86; p=0.032). Based on the daily IVR data, the percentages of callers who reported any drinking, drug use, or risky sex were 58.3%, 69.4%, and 69.4%, respectively.
Daily medication adherence
For each of the 44 IVR participants, Fig. 1 presents a scatter plot of total IVR call days as a function of the percentage of call days with reports of full adherence with prescribed ARV medications the preceding day over the 28- to 70-day IVR SM intervals. Participants' reports of perfect adherence ranged from 0% to 100% of days in the study period. Overall, 30 of the 44 participants (68%) reported perfect adherence on >95% of study days. The mean percentage of days with IVR reports of perfect adherence was 89.7 (SD=22.0); the median was 100%.
Concordance between adherence measures
Daily and weekly adherence measures were compared for the 28 main study participants with sufficient IVR reports to support comparisons. Table 2 presents the mean percentage adherence for each measure, correlations among measures, and t-test comparisons. Daily and weekly IVR reports of days involving full adherence were highly correlated. There was a near significant tendency for daily IVR adherence reports to be lower than the 7-day weekly recall. The 4-day weekly recall did not differ from either of the other two measures. Based on these analyses using the subset of participants with sufficient reporting days to be included, the percentage of IVR call days for which full adherence to HIV medications was reported (Fig. 1) was considered to be a reliable and valid measure.
Analyses were based on 28 participants with ≥10 daily observation days and ≥2 weeks of weekly reports over matched IVR intervals (see text). * p<0.0001.
Correlates of medication adherence
For the sample of callers as a whole, the percentage of IVR call days that included perfect adherence reports was significantly and negatively correlated with the percentage of baseline days involving any alcohol or drug use (r=−0.32, p=0.035), drug use only (r=−0.41, p=−0.0058), and duration of HIV/AIDS medical care (r=−0.30, p=0.049). Adherence was positively correlated with the percentage of participants' scheduled IVR calls completed during the daily SM interval (r=0.89, p<0.0001). This positive association was observed for pilot (r=0.65, p<0.16) and main study (r=0.79, p<0.0001) participants, notwithstanding the different IVR assessment intervals. Other baseline variables, including demographic characteristics and sexual practices, had no significant association with adherence.
Discussion
Medication adherence was variable over the IVR assessment interval for the sample as a whole. Although about two-thirds of participants reported adherence >95%, the common clinical target for optimal therapeutic benefits and transmission risk reduction, close to one-third reported adherence rates below this threshold. Given the positive correlation observed between IVR utilization and medication adherence, missed call days likely involved additional nonadherence days. The observed and apparent extent of nonadherence in this sample is of considerable clinical concern and underscores the importance of reliable, ongoing assessment of medication adherence.
Based on participants with sufficient observations for the reliability analyses, daily IVR adherence reports were significantly correlated with both the 7- and 4-day weekly recall measures, supporting the reliability of reporting across measures, including on the 4-day time frame widely used by the Adult AIDS Clinical Trial Group 6 and others. However, higher adherence was reported on both weekly reports compared to the daily measure, with a trend toward significantly higher reporting on the 7-day recall measure. Because reporting high adherence may be seen as a positive health behavior among patients in HIV treatment, social desirability concerns may have promoted over-reporting when participants were asked to summarize their behavior over a week. This contrasts with earlier analyses with this sample that found higher daily IVR reports of drug use and risky sex for which incentives exist for under-reporting. 15 Thus, the lower adherence reports found for prospective daily IVR SM compared to weekly recall measures may reflect slightly greater sensitivity and a more accurate picture of participants' day-to-day adherence behavior.
IVR-reported medication nonadherence was associated with higher baseline substance use and longer time in HIV medical care. The negative relationship between substance use and medication adherence is consistent with prior research, 7 but the relationship between adherence and tenure in medical care was unexpected. One possibility is that adherence drifted over time as a consequence of “treatment fatigue.” 32 In contrast, medication adherence was positively correlated with IVR utilization, and IVR use may have had a therapeutic benefit in promoting adherence. Such “reactive” effects of SM have been found for many behaviors. 19 Alternatively, the compliance observed across these behaviors may reflect a stable patient characteristic, such that participants more likely to adhere to their medication regimen also were more likely to adhere to the IVR call schedule. Future studies that manipulate IVR access as an independent variable will help disentangle causal relationships between IVR SM, a form of self-care, and adherence with life-saving medications for HIV/AIDS.
In clinical applications, IVR systems can be used to track medication adherence and risk behavior sequences and contexts, and support rapid detection of emerging risk factors for nonadherence (e.g., escalating substance use, worsening depressive symptoms). In this study, exploratory longitudinal analyses (not reported) of day-to-day sequences of substance use and medication nonadherence showed strong negative associations for four of six participants with sufficient data for analysis, such that a daily report of substance use was associated with a report of nonadherence. The near-real-time IVR information can be reviewed regularly (e.g., by a nurse or behavioral health professional) and help guide clinical decision-making by physically distant health care providers. Other potential IVR applications in HIV care include aiding new patients in navigating complex medication regimens; assisting those who have experienced disruption in their care routine due to acute medical complications; and closely monitoring and supporting other adherence requirements of patients challenged by distance and access to a medical clinic.
Potential limitations of IVR applications include start-up costs, data confidentiality protections, and the fact that IVR systems are not universally appealing. 19,31 However, as health care providers in the United States implement federally required EMR systems, the time is ripe also to implement IVR platforms as an add-on to new electronic information architecture, thereby reducing overall IVR start-up and maintenance costs.
Study limitations should be considered. First, the adherence measures appeared reliable based on the internal daily/weekly reliability checks for the subset of participants with sufficient IVR reports for analysis. Second, we did not have the opportunity to compare verbal reports with medical markers of adherence, such as lab-verified viral load or CD4 counts. Third, the results were obtained with a modest sample size in a single, rural Southern clinic. Findings should be generalized with caution to other rural settings and populations living with HIV/AIDS. Fourth, like many other extended IVR SM studies, 17,31,33 an electronic bank modestly reimbursed participants for making scheduled IVR calls. Whether similar results would be obtained without payment needs investigation, but alternatives to monetary payments such as vouchers and lotteries have been shown to effectively incentivize behavior change to promote health. 34
With these qualifications, the present study demonstrated the utility of IVR SM to assess medication adherence in rural persons living with HIV/AIDS. IVR systems can reach rural, disadvantaged, and other hidden populations living with chronic illness over long periods of time. Even in poor communities, phone access is near universal and is an affordable tool for extending the reach of care. Such telehealth applications deserve wider implementation and evaluation to help monitor and support adherence and other positive health behaviors in under-served risk groups.
Footnotes
Acknowledgment
This research was supported in part by NIH/NIDA grant no. 1 R21 DA021524 to Jalie A. Tucker.
Author Disclosure Statement
No competing financial interests exist.