
Abstract
This study sought to determine the synergistic effects of age and HIV infection on medical co-morbidity burden, along with its clinical correlates and impact on health-related quality of life (HRQoL) across the lifespan in HIV. Participants included 262 individuals across four groups stratified by age (≤40 and ≥50 years) and HIV serostatus. Medical co-morbidity burden was assessed using a modified version of the Charlson Co-morbidity Index (CCI). Multiple regression accounting for potentially confounding demographic, psychiatric, and medical factors revealed an interaction between age and HIV infection on the CCI, with the highest medical co-morbidity burden in the older HIV+cohort. Nearly half of the older HIV+group had at least one major medical co-morbidity, with the most prevalent being diabetes (17.8%), syndromic neurocognitive impairment (15.4%), and malignancy (12.2%). Affective distress and detectable plasma viral load were significantly associated with the CCI in the younger and older HIV-infected groups, respectively. Greater co-morbidity burden was uniquely associated with lower physical HRQoL across the lifespan. These findings highlight the prevalence and clinical impact of co-morbidities in older HIV-infected adults and underscore the importance of early detection and treatment efforts that might enhance HIV disease outcomes.
Introduction
In that regard, there has been increasing attention to the possible role of medical co-morbidity burden in the poorer health outcomes observed in older PLWH. In fact, the new conceptual model of aging with HIV infection proposed by the HIV and Aging Working Group of the NIH Office of AIDS Research posits that medical co-morbidities are seen earlier and more frequently in older PLWH, which leads to frailty, neurocognitive and functional impairment, organ system failure, and increased hospitalization. 11 Across the lifespan, HIV is associated with increased rates of co-morbidities such as hepatitis C co-infection 12 and metabolic syndrome 13 that heighten risks of adverse cognitive 13,14 and health-related outcomes (e.g., chronic liver disease progression 12 ). As PLWH grow older, they also become more susceptible to developing the physical and mental diseases associated with so-called “normal” aging. For example, older PLWH have higher prevalence of multimorbidity, 15 including cardiovascular complications such coronary artery disease, hypertension, hypercholesterolemia, and diabetes, 16,17,18 as well as cancer and diseases of liver, kidney, bone (e.g., ostopenia), and nervous system. 19 Older PLWH may also acquire these co-morbidities earlier in life relative to their seronegative counterparts: Guaraldi et al. 20 reported that the prevalence of multimorbidity (which indicates ≥2 noninfectious co-morbidities) among 41- to 50-year-old PLWH was comparable to that of seronegatives who were a decade older (i.e., 51–60 years of age). Similarly, Oursler et al. 21 reported that amongst HIV-infected and uninfected patients with pulmonary disease, PLWH experienced poorer functioning relative to seronegative individuals; In fact, a 50-year-old PLWH was functionally equivalent to a 68-year-old seronegative individual, 21 which further supports the role of HIV in possibly accelerating both the prevalence and onset of co-morbid conditions.
Nevertheless, there have been very few studies that have directly evaluated the synergistic effects of age and HIV on co-morbidity burden using appropriate comparison groups, thereby leaving questions about the unique and combined effects of these two increasingly intersecting risk factors. In one of the first such studies, Goulet et al. 22 reported interactions between HIV and older age for diabetes, vascular disease, liver disease, and substance use disorders in the Veterans Aging Cohort Study (VACS), with the highest rates in older PLWH. Guaraldi and colleagues 20 reported significantly elevated rates of multimorbidity, including cardiovascular disease, renal failure, bone fractures, and diabetes, in older PLWH as compared to demographically comparable seronegatives in Italy. In terms of the clinical correlates of co-morbidity burden in older PLWH, a handful of studies have identified associations with lower CD4 cell counts, 20,22 –24 higher HIV RNA levels in plasma, 22 –24 cART interruption, 25 and injection drug use. 24 The everyday impact of higher co-morbidity burden among older PLWH is also not well understood, though a few studies have suggested that such burden might increase the risk of clinician-rated disability and unemployment. 10,21
Thus, the existing literature suggests that older PLWH experience greater risk of multimorbidity and co-morbidity burden, which may be associated with poorer immunnovirologic functioning and injection drug use. The present study seeks to extend this literature by: (1) using a factorial design to determine the synergistic effects of older age and HIV infection on co-morbidity burden in a well-characterized cohort matched on demographics (e.g., education, premorbid IQ) and substance use histories who underwent comprehensive sociodemographic, psychiatric, cognitive, and medical research evaluations; (2) determining the clinical correlates of co-morbidity burden in both younger and older PLWH; (3) measuring co-morbidity burden with a standardized, weighted, and widely validated summary index (i.e., Charlson Co-morbidity Index); and (4) characterizing the association between co-morbidity burden and health-related quality of life in both younger and older PLWH.
Methods
The study protocol was approved by the University of California, San Diego (UCSD) human research protections program. Each participant provided written, informed consent, and was administered a comprehensive medical, psychiatric, and neuropsychological medical evaluation.
Participants
Participants included 262 individuals enrolled in an NIMH-sponsored study on the effects of aging and HIV on memory functioning, which was housed at the UCSD HIV Neurobehavioral Research Program (HNRP). Participants were recruited from local HIV clinics and from the general community. HIV serostatus was confirmed using enzyme-linked immunosorbent assays, along with a Western blot test. Consistent with prior research in HIV, 27 age group classifications were defined as: younger (i.e., age ≤40 years old) and older (i.e., age ≥50 years old). This approach yielded four study groups, including younger HIV- (n=56), older HIV-(n=65), younger HIV+(n=50), and older HIV+(n=91).
Participants were excluded if they had histories of severe psychiatric (e.g., schizophrenia) or neurological conditions (e.g., seizure disorders, closed head injuries with a loss of consciousness greater than 15 min, central nervous system neoplasms, or opportunistic infections) or if they met Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV 28 ) criteria for current (i.e., within the past 30 days) substance use disorders (i.e., abuse or dependence) as determined by the Composite International Diagnostic Interview (CIDI, Version 2.1). 29 The CIDI is a semi-structured computer-assisted interview for the assessment of psychiatric and substance use disorders using DSM-IV criteria that was administered by certified research associates and has been widely used in HIV research. 27 To confirm recent abstinence from alcohol and drugs, a urine toxicology test for illicit drugs (except marijuana) and Breathalyzer were used for screening on the day of evaluation. Due to the aims of the parent study, which were focused on the neurocognitive impact of aging with HIV infection, participants with a verbal IQ estimate <70 based on Wechsler Test of Adult Reading 30 were also excluded. Demographic characteristics of the participants are displayed in Table 1. The study groups were comparable for most demographics (e.g., education, sex, estimated premorbid IQ; p>0.10). However, the two younger groups had higher proportions of ethnic minorities relative to the two older samples (p<0.05; See Table 1 for more detail regarding proportions of ethnic minorities within the study groups). Self-reported sexual orientation was gathered via structured interview and is also reported in Table 1.
Data represent means (SD) unless otherwise noted.
p Value reflects omnibus group difference.
Median (interquartile range).
AIDS, acquired immune deficiency syndrome; ARVs, antiretrovirals; CD4, cluster of differentiation 4; CSF, cerebrospinal fluid; HDS, HIV Dementia Scale; MDD, major depressive disorder; POMS Total, Profile of Mood States, total mood disturbance score; SF-36 Total, RAND 36-Item Short Form Health Survey, general summary score; VIQ, verbal IQ (based on the Wechsler Test of Adult Reading); VL, viral load.
Measurement of medical co-morbidity burden
Medical co-morbidity burden was quantified using the Charlson Co-morbidity Index (CCI), which was selected because it: (1) was compatible with the available study data; (2) has strong construct validity, reliability and feasibility; 31 and (3) has been used in previous studies examining PLWH. 32 –34 The CCI accounts for 19 co-morbidities, each assigned a weight based on the adjusted 1-year mortality risk as determined by Charlson et al. 35 We excluded AIDS as a co-morbidity due to the inherent bias that would result as a function of our study group definitions (i.e., HIV+ versus HIV-), and its arguably outdated co-morbidity burden (CMB) weight in the era of cART. 36 A CCI was generated for each individual participant, blinded to HIV and age status by matching the ICD-9-CM codes derived from the standardized neuromedical and neuropsychological research examinations (detailed below) with each co-morbidity as reported by Deyo et al. 37 For this study, CCI coding of “dementia” was adjusted to account for the recent decrease in the prevalence rates of HIV-associated dementia (HAD) 38 and increase in the rates of milder forms of cognitive impairment in HIV infection. 39 Specifically, participants were given a weight of “1” if they were classified as having both neurocognitive impairment (NPI) and related functional declines, which is a classification that corresponds roughly to a diagnosis of mild neurocognitive disorder (MND) in HIV infection. 40
Medical evaluation
Each participant had a standardized medical history interview, structured neurological and medical examination, as well as collection of blood, cerebrospinal fluid, and urine samples consistent with previous studies that have been conducted through the UCSD HIV Neurobehavioral Research Program (HNRP; e.g., Heaton et al. 39 ). All medical history interviews were conducted by trained research staff and the examinations performed by clinicians (RN, NP, or MD). Medical history questionnaires completed by the participants were used as a guide during the medical interview process to complete case report forms evaluating past medical history, HIV disease stage, antiretroviral use history, current medications, and pertinent review of systems. While the majority of medical history data was collected via self-report, additional data and/or clarifications were collected utilizing medical records as available. For data on current medications, participants were asked to bring all prescribed medications or a medication list to their study visits. All antiretroviral (ARV) and concomitant medications were recorded at each visit (name, daily dose, dose units, frequency and start date). These medications were divided into ARV and non-ARV medications. Number of ARV medications includes each antiretroviral component regardless of formulation (e.g., the combination medication Truvada is counted as two ARVs: emtricitabine and tenofovir). Number of non-ARV medications includes all concomitant medications except those taken on an as needed basis. Current blood CD4 cell counts were measured by flow cytometry and HIV RNA concentrations in both plasma and cerebrospinal fluid (CSF) were assayed by ultrasensitive (lower limit of detection, 50 copies/mL) reverse transcriptase-polymerase chain reaction (Amplicor®, Roche Diagnostic Systems, Indianapolis, IN). Co-morbid medical diagnoses, current medications, antiretroviral history, and HIV disease characteristics (except for current CD4 and HIV RNA) were self-reported. Current blood CD4 cell counts were measured by flow cytometry, and HIV RNA concentrations in both plasma and CSF were assayed by ultrasensitive (lower limit of detection, 50 copies/mL) reverse transcriptase-polymerase chain reaction (Amplicor®).
Medical and HIV-disease related characteristics are presented in Table 1. The older HIV+group had a greater proportion of individuals infected with HCV relative to their older HIV- counterparts, and both older groups had larger proportions relative to the younger groups (p<0.05). With regard to HIV-disease characteristics, the older HIV+group had a longer duration of infection, lower nadir CD4 counts, a greater proportion of individuals diagnosed with AIDS (p<0.05), and a slightly lower proportion of individuals with detectable plasma HIV viral load (p=0.075) relative to the younger HIV+ group. The two HIV+groups were comparable for current CD4 count, as well as proportions of individuals on antiretroviral (ARV) therapy or with detectable CSF HIV viral load (p>0.10). Each HIV-infected participant was also administered the ACTG Adherence to Anti-HIV Medications questionnaire, a self-report measure designed to assess cART adherence (e.g., how many pills missed and why) over the 4 days prior to their assessment. Participants were classified as “poor adherers” if they missed one or more doses in the past 4 days. The older and younger HIV+groups did not differ in regards to ARV adherence (p>0.10; see Table 1).
Neuropsychological evaluation
Participants were administered the reading subtest of the Weschler Test of Adult Reading 30 as an index of pre-morbid cognitive functioning, and the HIV Dementia Scale (HDS) alongside a comprehensive neuropsychological test battery designed to assess cognitive domains most commonly affected in HIV-associated neurocognitive disorders (HAND) 40 including executive functions, attention/working memory, episodic learning and memory, verbal fluency, information processing speed, and motor skills (see Woods et al. 42 for details). Clinical ratings ranging from 1 (above average) to 9 (severely impaired) were assigned to each individual cognitive domain by a neuropsychologist (SPW) using published, standardized, and well-validated procedures 42 and used to determine the presence or absence of global neuropsychological impairment (NPI). A cut-point of 5 or greater was used as an indicator of global NPI.
To determine whether the observed NPI was “syndromic”, participants also completed a modified form of the Lawton and Brody 43 Activities of Daily Living (ADL) Scale, which has been used previously in the HIV literature as an index of daily functioning abilities. 44,45 This self-report measure requires the participant to rate his/her current and best ability to independently perform various basic (e.g., dressing) and instrumental (i.e., medication and financial management, housekeeping, grocery shopping, cooking, transportation, shopping, laundry, telephone use, and home repairs) activities of daily living (BADLs and IADLs, respectively). As this study was primarily concerned with the ability to carry out higher-order everyday activities, only IADL items were used for classification purposes and analyses 45 . Individuals were classified as IADL dependent if they reported a decline from their best level of functioning in their ability to carry out two or more functional tasks. 44,45 As noted above, this IADL variable was used to derive a weighted “syndromic NPI” variable for inclusion into the CCI, whereby individuals received a weight of “1” if they were classified as having both global NPI and IADL dependence.
Psychiatric evaluation
The current mood (i.e., covering the past week) of each participant was assessed using the Profile of Mood States (POMS), 46 which is a 65-item, self-report measure of current affective distress. Current (within the last 30 days) and lifetime (LT) major depressive disorder (MDD) and lifetime substance use disorders were assessed using the Composite International Diagnostic Interview. 29 Psychiatric and substance use diagnoses for the study groups are presented in Table 1. The older HIV+group reported greater current affective distress on the POMS (i.e., Total Mood Disturbance) relative to the two HIV- study groups (p<0.05), but did not differ from their younger HIV+counterparts (p=0.279). Current rates of MDD amongst the older HIV+group were significantly higher than the older HIV- group (p=0.007) and slightly higher than that of the younger HIV- group (p=0.061), though were comparable to that of the younger HIV+group (p>0.10). Lifetime rates of MDD within the older HIV+group were significantly greater relative to the younger HIV- group (p=0.002), though they did not differ relative to the older HIV- or younger HIV+groups (p>0.10). The study groups had similar rates of lifetime substance dependence disorders (p=0.720).
Assessment of Health-Related Quality of Life
Each participant also completed the RAND 36-item Short Form Health Survey (SF-36), which is a disease nonspecific 36-item self-report questionnaire designed to assess aspects of physical and mental health well-being, and has been validated in HIV as an index of health-related quality of life (HRQoL). 47,48 The overall SF-36 score (General Summary Score) is composed of two main summary scores (the Physical and Mental Health-Related Quality of Life subscales), which in turn are comprised of 4 subscales each, and range from 0 to 100 where higher scores indicate better HRQoL. The Physical Functioning (PF), Role-Physical (RP; i.e., role limitations due to physical problems), Bodily Pain (BP), and General Health (GH) subscales comprise the Physical Health summary measure, and the Vitality (VT), Social Functioning (SF), Role-Emotional (RE; i.e., role limitations due to emotional problems), and Mental Health (MH) subscales comprise the Mental Health summary score. Continuous Physical and Mental HRQoL summary scores were used for analyses.
Results
Shapiro-Wilk W-test showed that CCI was not normally distributed (p<0.001), so nonparametric statistics (e.g., Spearman's rho) were used whenever possible. In the multivariable models for which alternate nonparametric approaches were not readily available or easily interpretable, a review of the residuals revealed no major departures from normality. All statistical analyses were performed using JMP 9.0.2 software (SAS Institute, Carey). Hedges' g was used for effect size estimates and a critical alpha level of 0.05 was used for all analyses.
Age and HIV effects on the CCI
A multiple linear regression was used to explore the main and interactive effects of age and HIV infection on the CCI (Table 2), while accounting for potentially confounding variables that differed between the four study groups (i.e., ethnicity, HCV, POMS Total Mood Disturbance, and sexual orientation). The overall regression model predicting the CCI was significant [F(7,248)=8.82, Adjusted R2=0.18, p<0.001]. Analysis revealed a significant interaction between age and HIV (Estimate=0.46, p=0.005). Specifically, a significantly higher CCI was observed in the older HIV+ group relative to each of the remaining study groups (ps<0.001; Fig. 1), even when accounting for the aforementioned potentially confounding variables. The proportions of individual CCI conditions across the study groups in order of frequency in older HIV+ group are displayed in Table 3.
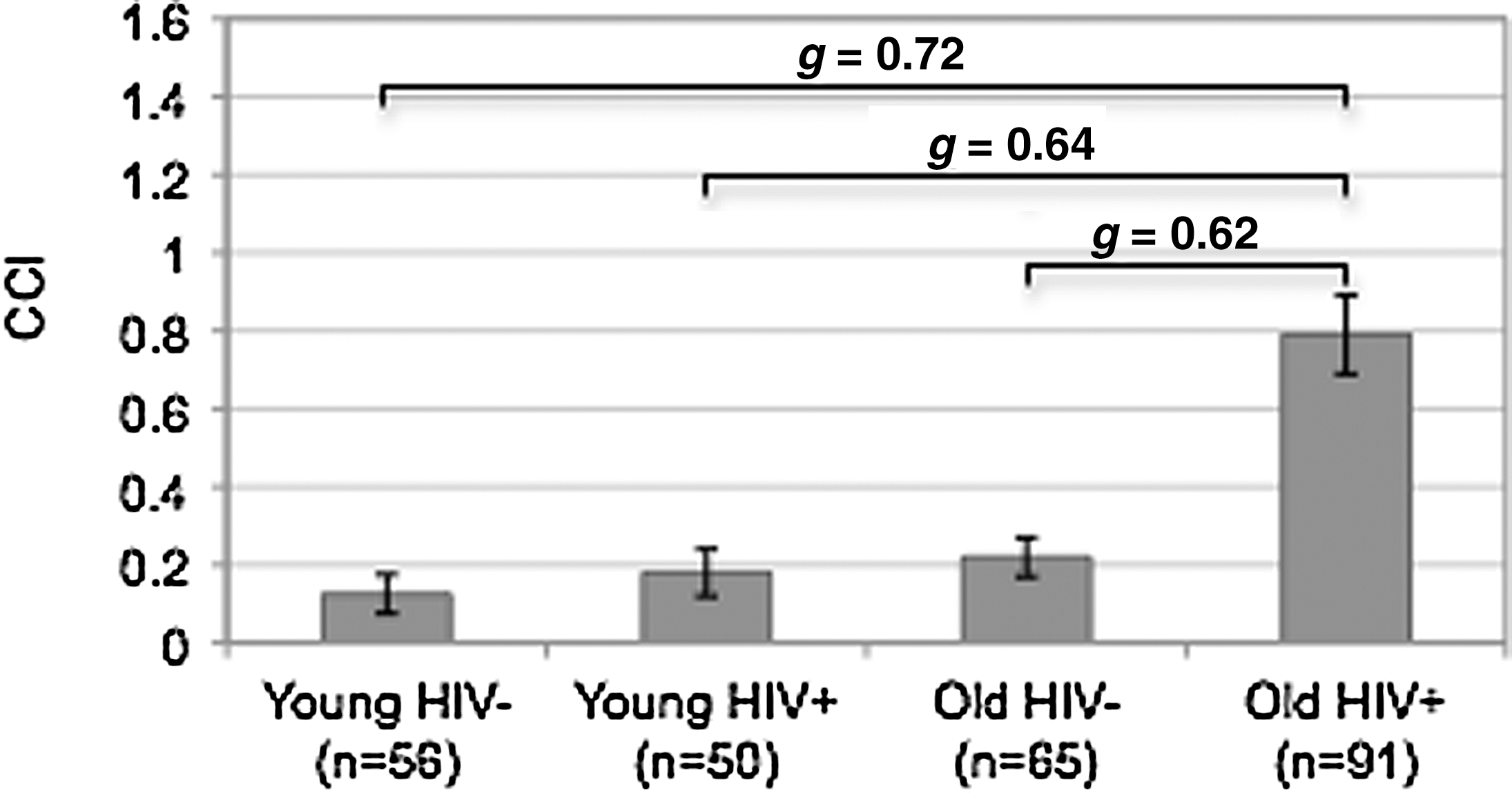
Bar chart displaying the interaction of HIV and age on the Charlson Co-morbidity Index (CCI). All p values<0.001.
Denotes significance at p<0.05.
CCI, Charlson Co-morbidity Index; HCV, Hepatitis C virus; HIV, human immunodeficiency virus; POMS, Profiles of Mood States.
p Value reflects omnibus group difference. HIV, human immunodeficiency virus; NPI, neuropsychological impairment.
Clinical correlates of the CCI in younger and older HIV-infected individuals
Next, exploratory correlational and regression analyses were conducted within the younger (n=50) and older (n=91) HIV+samples separately in order to identify any of the demographic (e.g., age, education, ethnicity, sexual orientation), psychiatric (e.g., lifetime MDD), medical (e.g., HCV, total number of medications) or HIV-disease (e.g., AIDS status) variables listed in Table 1 that may be associated with the CCI. The CCI was examined as a dichotomous variable in the younger HIV+group due to the severely restricted range of CCI values (i.e., values consisted of only 0 or 1, with 0 indicating no co-morbidities as indexed by the CCI), and as a continuous variable for analyses within the older HIV+ group (range=0, 4). Within the younger HIV+group, only greater current affective distress (i.e., higher POMS Total Mood Disturbance score) was a significantly associated with the CCI (p=0.014). Further examination into the individual POMS subscales revealed significant associations between the CCI and the vigor/activation (p=0.012) and depression/dejection (p=0.045) subscales only. Within the older HIV+group, only detectable HIV RNA plasma viral load emerged as a significant correlate of the CCI (p=0.037), a finding that persisted even when examined alongside ARV use (p=0.030).
Polypharmacy
The total number of non-ARV medications was also evaluated as a possible correlate of the CCI in the younger and older HIV+ groups. No significant relationship was found in the younger HIV+ group (p>0.10), though there was a significant, moderate correlation between total number of non-ARV and the CCI in the older HIV+ group (r=0.24; p=0.02).
Effects of age and the CCI on health-related quality of life in HIV infection
Lastly, correlational and multiple linear regression analyses were conducted within the entire HIV+sample (i.e., younger and older HIV+ groups combined; n=141) in order to explore the main and interactive effects of age and the CCI on aspects of physical and mental HRQoL in HIV (i.e., Physical and Mental HRQoL subscale summary scores), alongside factors that differed between the younger and older HIV+samples (i.e., ethnicity, HCV infection, AIDS status, duration of HIV infection, and sexual orientation; Table 4). Lifetime MDD was also included in the model due to its consistent association with adverse functional outcomes in the HIV literature. 44 While the younger and older HIV+ groups also differed on other HIV disease variables (e.g., nadir CD4 count), only AIDS status and duration of HIV infection were included in the models in order to maintain a statistically appropriate number of predictors given our sample size, and to avoid issues of multicolinearity. While related, AIDS status and duration of infection were less strongly associated relative to other pairings of HIV-disease characteristics (e.g., AIDS status and nadir CD4 count). Of note, however, the main findings from our analyses did not change regardless of which HIV-disease variables were included in the models. Significant regression models were observed for both the Physical [F(9,126)=7.36; adjusted R2=0.30; p<0.001] and Mental [F(9,125)=4.65; adjusted R2=0.20; p<0.001] HRQoL subscales. A trend-level age by CCI interaction was observed for the Physical HRQoL subscale (Estimate=6.38, p=0.089), though no significant interaction was observed for the Mental HRQoL subscale (p>0.10). A significant main effect of the CCI was observed for the Physical HRQoL summary score (Estimate=−9.23, p=0.011), though not for the Mental HRQoL summary score (p>0.10), nor were there main effects of age group for either measure (p>0.10). Lifetime MDD was the only other variable that emerged as a significant correlate of the HRQoL measures, and was significantly associated with both the Physical (Estimate=−8.01), and Mental HRQoL summary scores (Estimate=−8.74, ps<0.001). AIDS status was associated with Physical HRQoL though only at trend level (Estimate=−3.15, p=0.072).
Denotes significance at p<0.05.
AIDS, acquired immune deficiency syndrome; CCI, Charlson Co-morbidity Index; HCV, Hepatitis C virus; HIV, human immunodeficiency virus; HRQoL, health-related quality of life; MDD, major depressive disorder.
Discussion
As the prevalence of older PLWH has increased, there has been growing concern regarding medical co-morbidity burden in this population characterized by high rates of general and age-related chronic medical conditions and treatments. 20,23 Thus, identifying the nature and extent of medical co-morbidity burden in older PLWH, including its clinical and quality of life correlates, is imperative as these factors may have significant functional and public health implications. 11 Results of this study extend the prior literature on this topic by demonstrating synergistic effects of older age and HIV on an overall medical co-morbidity burden, which persisted even when accounting for potentially confounding variables that differed amongst the study groups (e.g., ethnicity, current affective distress, and HCV infection). Specifically, the older HIV+group had a significantly higher co-morbidity index with medium effect sizes relative to older HIV- (g=0.62), younger HIV+(g=0.64), and younger HIV- (g=0.72) cohorts. Results are consistent with and extend the aforementioned studies showing that older PLWH are at increased risk for various medical co-morbidities, including vascular disease, diabetes, and liver disease. 22 In fact, approximately 50% of our older HIV+group had at least one co-morbid medical condition that was considered for inclusion in the CCI (Fig. 2), which was notably higher than the rates observed in our older HIV-, younger HIV-, and younger HIV-groups (approximately 22%, 18%, and 13%, respectively). Moreover, when the CCI is expanded to include other current co-morbid conditions that are highly prevalent in both HIV and aging populations (i.e., hepatitis C virus and current MDD) and associated with poor health-related outcomes, 12,49 rates of at least one co-morbid condition in the older HIV+group increase to approximately 67% (n=61) of the sample, which was again considerably higher than the rates observed in the remainder of the groups (i.e., range 17–32%).

Proportions of study participants with unweighted CCI conditions across HIV serostatus and age group.
The most prevalent CCI conditions observed in our older PLWH were diabetes (18%), syndromic neurocognitive impairment (15%), and malignancy (9%). Chronic pulmonary disease was also prevalent in the older HIV+sample, (i.e., approximately 12%), but occurred at a rate that was comparable to the other study groups. Elevated prevalence rates in older PLWH have been previously observed for diabetes/metabolic syndrome, 15 –17,50 which have often been associated with ARV use. In fact, ARV use has been linked to a wide variety of metabolic complications (e.g., diabetes, hypertension 51 ) that can lead to further complications (e.g., metabolic syndrome, cardiovascular disease) and may increase non-HIV-related morbidity and mortality. 52,53 Non-HIV-related cancers are also common in older HIV-infected adults, 15,54 and may be associated with immunodeficiency. 55 The elevated prevalence rates of these conditions is alarming given recent increases in the rates of non-AIDS related deaths among older PLWH, which has been closely linked to cardiovascular and pulmonary disease as well as non-AIDS related malignancies. 56
Of particular interest is the relatively high prevalence of syndromic NPI among the various co-morbidities in the older PLWH. In this study, we operationalized syndromic NPI as having at least mild global neurocognitive deficits that interfered with daily functioning ability (i.e., akin to a diagnosis of HIV-associated mild neurocognitive disorder). In fact, the older HIV+individuals were over four times more likely to be classified as syndromic relative to their younger counterparts. The proportion of individuals with syndromic NPI in our older HIV+sample (15%) is consistent with the results of a recent large-scale multisite neuroepidemiologic CHARTER study 38 that reported a 14% prevalence rate. Of note, global NPI (impairment irrespective of functional impact) was evident in 39% of the older HIV+ group, which is also broadly commensurate with current prevalence estimates. 38 This is consistent with recent evidence suggesting that older HIV+ individuals may be particularly vulnerable to cognitive and functional decline. 5,10,27,57 Myriad adverse functional consequences have been linked to HIV-associated neurocognitive deficits specifically in older HIV+adults, including poor medication management, 58,59 financial difficulties, 59 and declines in activities of daily living. 10,57 Moreover, older HIV+ adults have high prevalence rates of co-existing conditions (e.g., substance use disorders, mood disorders) that have been established as independent risk factors for neurocognitive impairment (for a review, see Schuster and Gonzalez 60 ) and could further complicate functional outcomes. Collectively, the high proportion of syndromic NPI in older HIV+adults and the strong link between neurocognitive impairment and adverse functional outcomes highlights the importance of early detection and remediation of cognitive impairment in order to improve aspects of everyday living and/or to prevent further disability.
Findings of this study also suggest that there may be differential clinical correlates of medical co-morbidity burden (i.e., CCI) within older and younger PLWH that will be important to consider in the development of preventative and/or treatment measures. In our older HIV+sample, only detectable HIV RNA plasma viral load was significantly associated with the CCI, a finding which persisted even when accounting for ARV use. This is consistent with previous research suggesting an association between medical co-morbidities and viremia. 22 –24,53 For example, Monroe et al. 53 found a significant correlation between viremia and poor control of diabetes and hypertension in HIV-infected individuals. One interpretation of their findings was that poor virologic control leads to chronic inflammation, which is an established cardiovascular risk factor 61 and has been associated with poorer immune functioning. Another explanation for their findings, as well as the results of this study, is that the association between detectable viral load and medical co-morbidities in older HIV+adults may be related to poor medication adherence. This is of particular concern in light of the high proportion of NPI in our older HIV+sample, as older adults with HIV with cognitive impairment may be at increased risk for poor medication adherence. 59 Collectively, this highlights the importance of effective HIV disease management, particularly in older HIV+individuals, who may be especially susceptible to these co-morbid medical conditions that may further exacerbate HIV disease.
In the younger HIV+group, current neuropsychiatric distress (i.e., POMS Total Mood Disturbance) was the only significant correlate of medical co-morbidity burden, which was primarily driven by the depression/dejection and vigor/activation subscales. Although these data are observational and correlational, it is possible that there is a bidirectional relationship between these affective symptoms and medical co-morbidity burden. Specifically, greater medical co-morbidity burden may lead to more negative affective symptoms (e.g., depression, lethargy), or vice versa (e.g., leading a sedentary lifestyle may cause the development of medical co-morbidities). Interestingly, despite similar levels of self-reported affective distress and proportions of MDD, this association was not observed in the older HIV+cohort. One explanation is that the etiology of mood symptoms may differ for younger and older HIV+ groups, and that medical co-morbidity burden is not a major cause of depression in older HIV+ adults when other potential causes are considered (e.g., loss of a partner, reduced independence). Nonetheless, it is important to highlight the role of affective distress in medical co-morbidity burden as mood symptoms (e.g., depression, apathy) have been associated with adverse functional outcomes in HIV, including medication nonadherence, 58 difficulties with everyday activities, 62 and poorer HRQoL, 63 and are amenable to detection and intervention. 64 Thus, effective screening and treatment of mood symptoms, as well as encouraging healthy behaviors that have been utilized in treatment (e.g., exercise 65 ), may help to prevent the development of medical conditions that may result as a consequence of mood related issues and improve the medical health of younger HIV+individuals.
The clinical relevance of this study is highlighted by the independent association between medical co-morbidity burden and physical HRQoL across the lifespan. Specifically, a greater medical co-morbidity burden as measured by the CCI was associated with poorer physical HRQoL in HIV-infected individuals, even while accounting for variables that differed between the groups (e.g., ethnicity, sexual orientation) and other factors known to be predictive of HRQoL (e.g., lifetime MDD 10,66 ). Moreover, a trend-level interaction between age and co-morbidity was observed for physical HRQoL, whereby older (but not younger) PLWH with greater medical co-morbidity burden reported poorer physical HRQoL. In contrast, greater medical co-morbidity burden was not associated with poorer mental HRQoL across the lifespan. As noted above, diabetes, syndromic NPI, chronic pulmonary disease, and malignancy were the most prevalent in the HIV-infected group, which suggests that these conditions may play a unique role in physical HRQoL outcomes in HIV. This is consistent with previous research demonstrating associations between poorer HRQoL and neurocognitive impairment (e.g., prospective memory 66 ). Relatedly, diabetes and chronic lung disease have been associated with clinician-rated functional outcomes 10 and reduced ability to carry out physical day-to-day activities (e.g., eating, walking, running 26 ), respectively. Collectively, these results suggest that adverse functional and health-related outcomes may be associated with co-morbid medical conditions that are highly prevalent in HIV infection, particularly in older adults.
The current study has a few limitations that are worth consideration. First, the cross-sectional nature of our study does not allow for conclusions regarding causality; for example, we are unable to determine whether the increased rates of age-related medical co-morbidities is a cause of accelerated aging due to HIV. We also made a few modifications to the comprehensive medical co-morbidity index that limits comparison of our results with other studies. As mentioned above, CCI coding of “dementia” was adjusted to a classification that corresponds roughly to a diagnosis of mild neurocognitive disorder (MND) in HIV infection 40 to account for the recent decrease in the prevalence rates of HIV-associated dementia (HAD) 38 and increase in the rates of milder forms of cognitive impairment in HIV infection, 39 as well as the demonstrated impact of neurocognitive impairment on mortality in HIV. 67,68 Moreover, we excluded AIDS diagnoses from the CCI given the nature of our clinical samples (i.e., HIV-infected versus HIV-seronegative individuals), and due to the arguably outdated index score for the AIDS diagnosis. 36 However, future research using a CCI including AIDS with an updated index score may provide additional useful information with regard to the influence of disease progression on medical co-morbidity burden in both younger and older HIV-infected adults.
With regard to the demographic characteristics of the study samples, our HIV+group were predominantly male, which limits the generalizability of our findings, given evidence to suggest lower HRQoL in women with HIV. 69 –71 Our “older” samples were also relatively young relative to the mean age in traditional aging literature, and the prevalence and clinical correlates of medical co-morbidity and HRQoL may differ as these older HIV infected individuals reach later decades (e.g., 70s and 80s). Moreover, our older HIV+cohorts were mostly Caucasian, which is likely reflective of larger cohort effects evident in the San Diego County HIV epidemic. 72 While we did not find an association between ethnicity and either physical or mental HRQoL in the current analyses, future research should continue to consider ethnicity as a potential contributing factor, given prior evidence of poorer self-reported HRQoL in ethnic minorities (e.g., Hispanic individuals) with HIV infection 73 and the importance of HRQoL in HIV-related health outcomes and treatment. Lastly, due to the cognitive focus of parent study from which these data were drawn, we excluded individuals with very low reading abilities (i.e., estimated premorbid verbal intelligence less than 70), which inherently limits the generalizability of our findings, particularly given the potential role of health literacy in co-morbidity burden and its impact on HRQoL. 74
Also of note is that the vast majority of our sample was on antiretroviral medications, some of which have been associated with higher risk for cardiovascular and metabolic complications. 75 Relatedly, we did not thoroughly examine the effects of specific non-HIV medications in older HIV-infected adults. While there was an association between total number of non-HIV medications and medical co-morbidity burden, we were unable to determine whether specific medications were driving these effects. Further research is needed to identify specific HIV and non-HIV related medications that may be associated with greater medical co-morbidity burden so that medication regimens may be appropriately and individually adjusted based on the risk of various medical conditions.
Despite these limitations, these findings are of significant clinical and public health interest. Advances in treatment have led to significant decreases in AIDS-related events, though non-AIDS related conditions (e.g., cardiovascular complications, malignancies) have increased, 56,76 particularly in older HIV-infected individuals. Co-morbid medical conditions can result from a myriad of factors including HIV-disease and age-associated factors, as well as HIV treatment characteristics (e.g., antiretroviral therapy), which should be taken into consideration when reviewing treatment options and developing appropriate medication regimens. Moreover, many of these conditions are amenable to treatment to some degree, thus it is critical that HIV-infected individuals, particularly those who are older, receive comprehensive medical evaluations to ensure early detection and remediation of conditions or symptoms in order to reduce co-morbid medical burden and improve overall health-related quality of life.
Footnotes
Acknowledgments
The San Diego HIV Neurobehavioral Research Program (HNRP) group is affiliated with the University of California, San Diego, the Naval Hospital, San Diego, and the Veterans Affairs San Diego Healthcare System, and includes: Director: Igor Grant, MD; Co-Directors: J. Hampton Atkinson, MD, Ronald J. Ellis, MD, PhD, and J. Allen McCutchan, MD; Center Manager: Thomas D. Marcotte, PhD; Jennifer Marquie-Beck, MPH; Melanie Sherman; Neuromedical Component: Ronald J. Ellis, MD, PhD (P.I.), J. Allen McCutchan, MD, Scott Letendre, MD, Edmund Capparelli, PharmD, Rachel Schrier, PhD, Terry Alexander, RN, Debra Rosario, MPH, Shannon LeBlanc; Neurobehavioral Component: Robert K. Heaton, PhD (P.I.), Steven Paul Woods, PsyD, MarianaCherner, PhD, David J. Moore, PhD, Matthew Dawson; Neuroimaging Component: Terry Jernigan, PhD (P.I.), Christine Fennema-Notestine, PhD, Sarah L. Archibald, MA, John Hesselink, MD, Jacopo Annese, PhD, Michael J. Taylor, PhD; Neurobiology Component: Eliezer Masliah, MD (P.I.), Cristian Achim, MD, PhD, Ian Everall, FRCPsych, FRCPath, PhD (Consultant); Neurovirology Component: Douglas Richman, MD, (P.I.), David M. Smith, MD; International Component: J. Allen McCutchan, MD, (P.I.); Developmental Component: Cristian Achim, MD, PhD; (P.I.), Stuart Lipton, MD, PhD; Participant Accrual and Retention Unit: J. Hampton Atkinson, MD (P.I.); Data Management Unit: Anthony C. Gamst, PhD (P.I.), Clint Cushman (Data Systems Manager); Statistics Unit: Ian Abramson, PhD (P.I.), Florin Vaida, PhD, Reena Deutsch, PhD, Anya Umlauf, MS. The authors thank Marizela Cameron, Erica Weber, and Nichole Duarte for their assistance with study management. This research was supported by National Institutes of Health grants R01-MH73419 and T32-DA31098 to Dr. Woods, P30-MH62512 to Dr. Grant, T35-AG026757 to Dr. Dilip Jeste, and L30-DA034362 to Dr. Iudicello.
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, nor the United States Government.
Author Disclosure Statement
The authors report no conflicts of interest.