
Abstract
Some people living with HIV (PLHIV) refuse to initiate antiretroviral therapy (ART) despite availability. Between March 2010 and September 2011, using a social ecological framework, we investigated barriers to ART initiation in Lusaka, Zambia. In-depth interviews were conducted with PLHIV who were offered treatment but declined (n=37), ART staff (n=5), faith healers (n=5), herbal medicine providers (n=5), and home-based care providers (n=5). One focus group discussion with lay HIV counselors and observations in the community and at an ART clinic were conducted. Interviews were audio-recorded, transcribed, and translated, coded using Atlas ti, and analyzed using latent content analysis. Lack of self-efficacy, negative perceptions of medication, desire for normalcy, and fear of treatment-induced physical body changes, all modulated by feeling healthy, undermined treatment initiation. Social relationships generated and perpetuated these health and treatment beliefs. Long waiting times at ART clinics, concerns about long-term availability of treatment, and taking strong medication amidst livelihood insecurity also dissuaded PLHIV from initiating treatment. PLHIV opted for herbal remedies and faith healing as alternatives to ART, with the former being regarded as effective as ART, while the latter contributed to restoring normalcy through the promise of being healed. Barriers to treatment initiation were not mutually exclusive. Some coalesced to undermine treatment initiation. Ensuring patients initiate ART requires interventions at different levels, addressing, in particular, people's health and treatment beliefs, changing perceptions about effectiveness of herbal remedies and faith healing, improving ART delivery to attenuate social and economic costs and allaying concerns about future non-availability of treatment.
Introduction
With HIV prevalence estimated at 14.3% in the Zambian population aged 15–49 years 13 and an estimated HIV incidence of 1.6%, 14 Zambia is one of the countries in SSA worst hit by the pandemic. Since 2005, free ART services have been progressively rolled-out in public sector clinics, resulting in a steady increase in the number of people on ART. However, not everyone eligible for treatment is receiving it. At the end of 2010, out of an estimated 503,284 adults and children in need of ART, only 68.4% were receiving it. 15
While many studies have been conducted on barriers to patient initiation of ART, most of these studies have been conducted outside sub-Saharan Africa (SSA), the sub-continent worst hit by the HIV pandemic. In Zambia, these studies have comprised: a quantitative study; 16 a sub-study of a clinic-based HIV prevention programme; 17 and a qualitative study conducted during the early years of ART roll-out. 18 The reported barriers to patient-initiation of ART have included financial and logistical costs, 16,18 negative perceptions of medication, 16,17 fear of stigma, 17,19 and fear of involuntary disclosure and straining marital relationships. 17 In view of the steady roll-out of free life-saving antiretroviral medication in many countries and the drive towards universal access, more studies on non-uptake of treatment have become more critical to inform successful delivery of ART services. To corroborate previous evidence and to add to the body of evidence, we used the social-ecological framework 20 –22 to investigate the different-level factors hindering HIV-patient initiation of HIV treatment.
Analytical framework: Social ecological framework
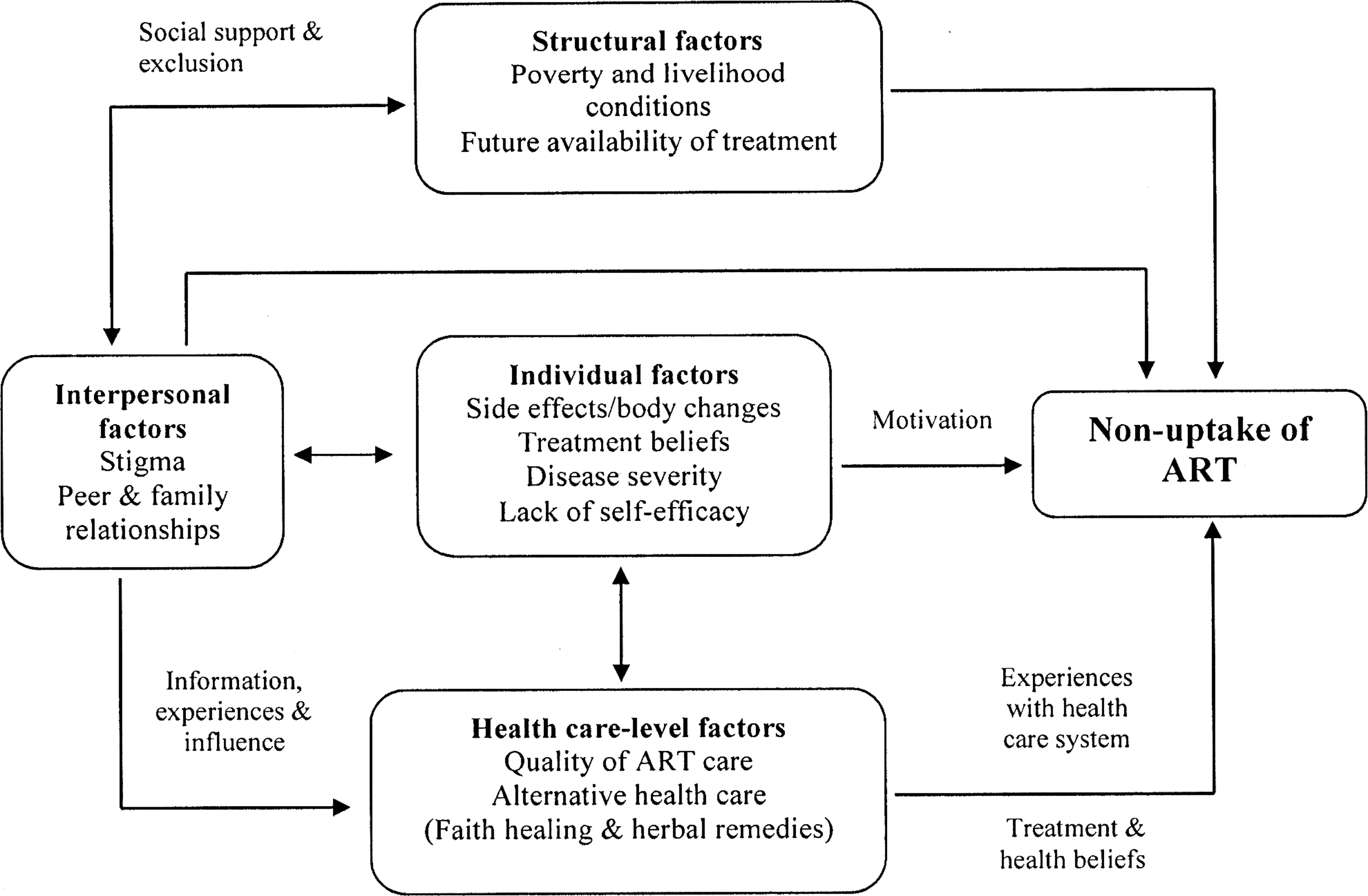
The social ecological framework provides a comprehensive approach for exploring and encapsulating the wide ranging individual and non-individual level factors that dissuade individuals from initiating treatment, including how they are linked. The social ecological framework positions health-seeking behavior in a ‘social ecology’ 20 in which treatment-seeking behavior is influenced not only by personal factors but also by interpersonal, health-system and structural-level factors, all embedded in this ‘social ecology’ (Fig. 1). The framework bridges the divide between “individualist” and “structuralist” models of health-seeking behavior by treating both paradigms as complementary and lying on the same continuum. 20 Human behavior is therefore construed not as something that exclusively resides in the individual but also a reflection of wider interactive dynamic processes in the social environment. 20 –22

Social ecological framework of non-uptake of HIV treatment.
Based on previous studies on non-uptake of treatment, 4 –7,10,12,16,17,20,23,26 –28 we developed a schema of the social-ecological framework that depicts the different level factors that undermine patient uptake of treatment (Fig. 1). At individual level, personal characteristics such as perceived disease severity, illness, and wellness interpretations and treatment beliefs inhibit uptake of treatment. 21 The social ecological framework also shows that treatment-seeking behavior is generated and perpetuated through socially structured interactions, 22 which are sometimes deeply engendered. 23 These social relationships serve as a source of information, influence, experience, 21 and social and economic support, 20,24,25 which in turn impacts on treatment-seeking behavior.
Treatment-seeking behavior is also influenced by the way health services are provided. 21 Even when individuals are motivated to seek treatment, studies have shown that health system constraints such as long waiting times, 20,21 costs of accessing treatment due to distance to the treatment centers, 10,20 and poor patient–provider interactions 21,26 dissuade individuals from seeking treatment. At the wider society level, structural-level factors—barriers that lie outside the direct control and influence of the individual 20,21 —also undermine uptake of treatment. These include health policies such as charging user fees 18 and poverty and livelihood circumstances. 16,27 As a result, based on their health and treatment beliefs as well as social influences, some individuals opt for herbal medication and faith healing. 28
The data collection and analysis was therefore guided by these different multi-level categorizations that underpin the social-ecological framework in order to gain in-depth insights into the different factors that undermine patient uptake of antiretroviral treatment.
Methods
Study setting
The study was conducted in a low-income, high-density residential area of Lusaka, Zambia. The majority of the residents are poor, eking out a living in the informal sector, mainly selling fruits, vegetables, meat products, charcoal, and second-hand clothes in the city center markets or in the open-air local markets. Small makeshift shops, locally called ‘tuntemba’, are ubiquitous—scattered along the dusty roads, in the local markets, or next to homes. A few residents are in formal employment in the public and private sectors of the economy. Some youth earn their income by doing daily piece-works as construction workers in the neighbouring communities. Others work as taxi, bus, and truck drivers. Most days, many of these informal sector workers set off for livelihood activities early morning and return home late in the evening. Unemployment is endemic, not only amongst youth but also amongst the old, many of whom lost their jobs during the economic reforms of the 1990s. Some of the unemployed, more especially the youth, have had little formal education and spend time patronizing the bars and drinking places. These places provide opportunities for girls and young women to engage in transactional sexual relationships.
Christianity is the predominant religion. The United Church of Zambia (UCZ), Roman Catholic Church, New Apostolic Church, and the Seventh-Day Adventist Church (SDA) are the mainstream churches. Since the official declaration of Zambia as a Christian in the 1990s, there has been an exponential increase in the number of Pentecostal churches in Zambia, some of which profess faith healing for health problems, including HIV.
Since 2006, a public sector clinic based in the study area has been providing free ART services. The clinic services a catchment population of over 150,000 people. By mid-2010, the clinic had more than 5000 people on ART and more than 5000 on pre-ART. The ART clinic attends to more than 100 patients (old and new) per day. Other HIV-related services in the area such as HIV testing, male circumcision, and reproductive health services are complemented by local and international non-governmental organizations. In parallel with the formal health system, traditional healers and herbalists abound, some claiming to provide herbal remedies that ‘boost’ the immune system of PLHIV. Home-based care providers either affiliated with local non-governmental organizations or churches provide psychosocial, treatment, and spiritual support to PLHIV and their families.
Study procedures
This was an exploratory, community-based qualitative study. This study design was suitable for identifying and eliciting in-depth insights into factors hindering uptake of treatment. Due to the difficulties of identifying PLHIV eligible for but not on ART, a three-pronged purposive sampling strategy was employed. Some PLHIV who had been initiated on but opted not to start ART were identified, contacted, and recruited through ART staff of a public-sector clinic located in the study area. Others were contacted and recruited through their lay home-based care providers. Also, because some of the PLHIV had formed social networks, using snowball sampling, each PLHIV interviewed was asked to nominate and contact on behalf of the researchers individuals they knew were eligible for ART but had opted not to start treatment. In all instances, only PLHIV that agreed to be interviewed were later contacted and appointments made for interviews. Living in the study area for an extended period of time (18 months) helped the researcher (first author) to win the trust and confidence of these PLHIV, thereby enabling them to open up and share their perspectives for not starting treatment.
Data collection and analysis
Data was collected between March 2010 and September 2011. Three data collection methods were employed. In-depth, audio-recorded, open-ended interviews were held with PLHIV (n=37), ART staff (n=5), religious leaders (n=5), home-based caregivers (n=5), and herbal medicine providers (n=5). Some PLHIV were contacted again and re-interviewed during the study period. The main initial question asked to PLHIV was: ‘would you explain why you decided not to start treatment?’ Data on the demographic characteristics and livelihood conditions of the PLHIV was also collected. Key informants were asked: ‘why do PLHIV eligible for treatment opt not to start medication?’ Interviews with clinic staff and religious leaders were conducted in English, while interviews with PLHIV, herbal medicine providers, and home-based caregivers were mostly conducted in the local language, Nyanja. One focus group discussion was conducted with voluntary counseling and testing (VCT) staff (n=10) of the local public sector clinic to elicit their perspectives on PLHIV reluctance to initiate treatment.
Structured observations were conducted at the local ART clinic and in the community. Sit-in observations at the ART clinic aimed at gaining insights into inter alia, patient–provider relationships, waiting times, and patient beliefs about and experiences of being on treatment. Observations in the community included conducting transect walks, attending social events, and religious/church meetings. They were aimed at understanding social relationships and ties, lifestyle activities, livelihood activities of the people, identifying health care providers located in the community, and gaining insights into ‘lay talks' about HIV treatment and informal health care services.
The use of different data collection methods helped gather in-depth data as well as validate the data collected. Data collection and preliminary data analysis were cyclical: preliminary data analysis informed ensuing interviews and data collection was ended when no new insight emerged from the interviews.
The interviews conducted in the local language (Nyanja) were translated, and all interviews were transcribed verbatim. Latent content analysis 29 was used to analyze and interpret the data. All interview and focus group discussion transcripts and observational field notes constituted our unit of analysis. Unit of analysis refers to all words and phrases of the interview transcripts and written field notes. 29 These were read several times to create a sense of the whole data. 29,30 Atlas ti version 6 was used to organize, manage, and code the data. The interview transcripts and field notes were coded, and the codes compared for similarities and differences, and then grouped into categories on a manifest level. Themes were then generated by interpreting the categories for their underlying meaning. In line with the analytical framework, the themes for non-uptake of treatment are presented as individual-level, interpersonal, health-system, and structural-level factors. For instance, codes such as feeling healthy, lack of self-efficacy, fear of treatment-induced body changes, and perceptions of HIV medication as poisonous and harmful were categorized as individual-level factors. Collectively, these were thematically interpreted as perceptions and experiences of health and treatment.
Protection of research participants
Ethical approval was granted by the ethics committee in Basel (Ethik-Kommission beider Basel) and the University of Zambia Humanities and Social Sciences Research Ethics Committee as part of the research study ‘Improving equity of access to HIV care and treatment in Zambia.’ Administrative clearance was also obtained from the Ministry of Health at national and district levels. Written informed consent was obtained from all research participants. To ensure confidentiality and avoid involuntary disclosure of their HIV status, most of the PLHIV were interviewed at neutral locations such as at the local health facility, homes of respondents' friends and at respondents' local churches. Some PLHIV preferred to be interviewed at home. To protect the identity of respondents, all identifying information was excluded from the interview transcripts.
Results
Characteristics of PLHIV not on ART
The majority of the respondents (n=24) were women, almost half (n=18) were aged between 25–34 years old, and the oldest was a married woman aged 51 years old. More than two-thirds (n=27) made a living in the informal sector. Almost two-thirds (n=21) had known their HIV status for at least 2 years and more than two-thirds (n=27) had not been on ART for between 6 months and 2 years (Table 1).
Reasons for declining ART
Using the social ecological conceptualization, factors inhibiting patient uptake of HIV treatment are subsumed as individual, interpersonal, health system, and structural factors.
Individual-level factors: Perceptions and experiences of health and treatment
Feeling healthy
Individual experience of health was found to heavily influence uptake of treatment. Despite acknowledging being infected, some PLHIV nonetheless assessed their eligibility for treatment not in terms of their immune system as clinically defined through CD4 cell count and viral load but in terms of their subjective experiences of their corporeal health. The absence of severe physical symptoms and the lack of negative impact of HIV infection on their productive and social lives dissuaded them from starting treatment. Normalcy was maintained as long as possible, as one PLHIV explained:
For me, I am living a normal life; I am not experiencing any problems. My life is just normal, not until it hits in, you know what I mean, not until it really becomes worse. So, I do not think the medicine will make any difference right now. (23-year-old man)
Feeling healthy also made a few PHIV express doubt about their HIV status. For a few women, lack of symptoms and giving birth to an HIV-negative child without taking medication for prevention of mother-to-child transmission of HIV (PMTCT) fed into doubts about the validity of the HIV test results.
Lack of self-efficacy
Perceived inability to be on life-long treatment discouraged some PLHIV from starting medication. They felt that they would not manage to adhere to life-long treatment. Others expressed reluctance to adjust their social lifestyles particularly stopping alcohol consumption as advised by treatment counselors. As one lay ART support worker explained:
Some, it is because of beer, especially men, what I have seen is that it is common. You find that when they are told that you cannot mix beer and medication, they really find it hard because they think they cannot do away with beer. So they do not want to start medication. (37-year-old ART adherence counselor)
Fear of treatment-induced body changes
While some PLHIV acknowledged the value of treatment, side effects including treatment-induced body changes inhibited its uptake. Most PLHIV, especially women, gave accounts of how ART had irreversibly made the body shapes of their spouses, friends, and relatives “structure-less” or “deformed,” and these experiences dissuaded them from initiating treatment. Some were fearful that this could ignite stigma, alter their social relationships, or reducing their chances of finding marital partners. The commonly mentioned bodily changes were breast enlargement, abdominal fat accumulation, skin pigmentation, and muscle wasting in the face, arms, and legs. As one PLHIV illustrated:
Like my husband when he started, he was taking Triomune 30. He was slimming and slimming, and even this time when you look at him, his legs are very thin, not the way he was at first. Even my sister-in- law, she had a very nice body but when she just started treatment, her breast grew big, her stomach bulged.…It changes the structure of the body, you become structure-less. (32-year-old woman)
Perception of HIV medication as poisonous and harmful
Related to concerns about side effects and treatment-induced body changes, some PLHIV perceived ART as poisonous and harmful. While they acknowledged witnessing a trajectory of improved health in other PLHIV after starting treatment, they also viewed HIV medication as harmful and insidiously inflicting bodily harm, sometimes leading to death in unexplained circumstances. While some PLHIV may have died on account of starting treatment late, some PLHIV attributed their death to the treatment itself. Two excerpts below illustrate these concerns:
The ARVs kill very slowly. Your body looks healthy, but inside, the ARVs are eating, eating up your body. Then next, you just develop small sickness and then die. Can't you say it is the ARVs that have killed that person? The problem is that with ARVs, you look very healthy, but you do not know what the ARVs are doing in your body. (30-year-old man)
You know what happened is that I had my late sister, second born in our family. Up to now, I still believe that it is the ARVs that killed her because before she started treatment, yes she used to complain about her health here and there, but when she just started treatment, a week never elapsed and she died, only after 3 or 4 days of starting treatment. (27-year-old man)
Interpersonal-level factors: Social exclusion and social network influence and experience
Treatment-induced stigma
At social relational level, fear of stigma either within the family or at community level dominated the thoughts of some PLHIV. They feared that being seen at the ART clinic or experiencing treatment-induced body changes would creating visibility of their HIV status and consequently attract stigma:
Like me, my relatives do not know that I am HIV positive. My fear is that if I start treatment, they will know. You know even in the families, not everyone has knowledge about HIV and treatment. Stigma is there in the homes. (39-year-old married woman)
For a kind of body like mine, if you gain weight, people would start suspecting. So to avoid people talking, to avoid people discriminating against you, I think it is better to live without the medicine. (24-year-old man)
Family influence
Non-uptake of treatment was further modulated by family influence. Family members and friends not only served as sources of information about ART but also imposed their health beliefs and wielded influence, and sometimes power, on treatment-seeking behavior. Many of our research participants gave accounts of how friends and family members had encouraged them to take herbal remedies or go for faith healing instead of ART. One young woman explained her experience:
My mother told me that I should just be going to church for prayers. So that is how I started going for prayers.…So, when I was prayed for, I went to the clinic to re-test to find out if truly I had been healed. So when I was tested, I was told that I was still HIV positive. I never believed this and my mother was very cross with me. She accused me of lacking faith and explained that, that was also the reason why I was not getting healed. (24-year-old woman)
The family influence could also be directed from the children to the parents. An elderly PLHIV died on account of having declined to start treatment following the wish of his children. A lay home-based care provider narrated the experience of his deceased client:
There is one man in the area, one of my clients. We approached him and counseled him and he was ready to start treatment. When he told his children about it, the children followed us up and told us to keep away. They said that they go for prayers and there is no need for their father to go to the clinic and start medication. So that is how we gave up and a few months later, we just heard that the man had passed away.…If the man had started treatment, he could have been alive up to this day.
Peer influence
Similarly, for some PLHIV, observing friends continue living ‘healthy’ and ‘normal’ lives without recourse to treatment further convinced them not to start treatment. Within friendship circles, PLHIV reportedly discussed ART and these discussions often centered on the negative effects of treatment, including being a drug ‘addict’. As one man succinctly put it:
You find that sometimes in social gatherings, you talk about some of these things. Others would say the drugs are not good for your health, others would say once you start treatment, you become like an addict; you cannot stop the medication, and if you do, you die. Some people would say the drugs have very, very bad side effects; very difficult to deal with. That you see a person becoming fat, not that normal way of gaining weight. (27-year-old man)
Structural-level Factors: Livelihood constraints and sustainability of HIV treatment
Food insecurity— “… the drugs will just kill me”
Most of the PLHIV interviewed reported lacking an adequate and steady income and came from food insecure households. This dissuaded them from starting treatment. Some respondents reported more than one household member and sometimes multiple generations of family members on treatment or diagnosed with HIV. Given the food and nutritional demands associated with being on antiretroviral treatment, some PLHIV suspended initiating treatment until their livelihood conditions had improved. Two respondents who suspended starting treatment narrated their exasperating situation:
I was wondering how I was going to manage to take the medication; I do not have a good job and steady income; I do not have a good diet; so how am I going to manage those drugs? My husband is on treatment and he is not working; the little money that we make have to be spent on him to improve his nutritional status. So, I said I will not start now. (51-year-old married woman)
The other problem is that once you start treatment, you need to have good nutritional foods to accompany the medication and for the medication to work well in the body. But for us, we do not have good jobs, and sometimes the whole day goes without selling anything [earning an income] and that creates problems in terms of having enough food to eat. (30-year-old man)
Future availability of treatment
A few PLHIV expressed doubts about long-term availability of treatment. These fears were reinforced by reported intermittent shortages and rationing of drugs in public sector clinics and reported pronouncements by Zambian government officials about challenges of keeping people on long-term treatment. Aware that HIV drug supplies were heavily funded by external support and harboring doubts about government's ability to fund treatment with local resources, some PLHIV opted not to take the risk of starting treatment. One PLHIV illuminated this concern:
Even these days when you are listening to the news, the Minister of Health was saying that the way HIV is going, in future, the government might even fail to provide these ARVs.…These drugs, we are told that if you stop for some time, it is a problem. Imagine the government just tells us that there is a shortage of ARVs, then what happens? (42-year-old woman)
Programme-level factors: Health system constraints and availability of alternative therapy
Quality of ART care
Even for those eager to start ART, the way treatment services were being delivered dissuaded PLHIV from initiating treatment. Health facilities had to cope with an enormous number of patients and lacked the resources and time to adequately attend to patients. For PLHIV not on ART, congestion and long waiting times at ART clinics were seen as imposing inordinate social and opportunity costs. The social costs included involuntary disclosure of HIV status while seeking care meant suspending livelihood activities. Therefore, the incentive to start treatment especially when PLHIV still felt ‘healthy’ diminished:
Truly speaking, it is not because of ignorance; it is not that we do not know the good things that the ARVs can do to us. The problem is because of the services.…The process is so long. (27-year-old man)
The thing they are also complaining about is that they come here at 05 hours but leave at 16 hours. That day when they are coming to get their ARVs, their day's programmes are all shattered. Right now, if you have to look at the defaulter rate, it is also growing. There are people who even say that ‘if I had money, I would go and look for alternative treatment instead of spending time at the clinic.’(ART support worker)
In view of the perceived disadvantages of initiating treatment, there are also alternatives to ART that may seem more attractive. These serve as pull-factors from seeking ART care:
Herbal treatment
In the quest to maintain their health in the absence of ART, all the PLHIV interviewed reported using herbal remedies, sometimes at great financial cost. The most commonly used herbal remedies were moringa, aloe vera gel (also locally available in plant form called tembusha), ginger, garlic, and Chinese herbal remedies. While some of the herbs were bought from the drug stores and mobile herbal medicine traders, some PLHIV reported locally growing some of these herbs (particularly tembusha), thus ensuring easy and unfettered access to ‘treatment’. A local herbal medicine provider sold aloe vera gel for ZMK150 (US $30) for a one-liter container. Some PLHIV reported being financially supported by other family members to purchase these herbal remedies. Ironically, some ART staff with HIV also reported opting for herbal remedies instead of ART:
When they told me that my CD4 count was low, I just started using herbs like moringa, mojic and after that, my CD4 count improved a bit up to 460 something. (32-year-old woman—PMTCT support worker, not on ART)
Faith healing
Some PLHIV also opted for faith healing. Some church Pastors either from within or outside the study area conducted healing sessions. One local church held healing sessions every Wednesday and Thursday afternoon, while another church conducted healing sessions every Saturday. Sometimes open-air inter-denominational prayer sessions for ‘healing and deliverance’ were conducted and people moved across Christian denominations for healing. Observations in selected churches revealed some Pastors openly preaching about God's power to cure any disease, including AIDS, and some PLHIV gave testimonies of how God had ‘cured’ them of HIV. One old woman challenged her fellow church members to always look up to God for help. In our ensuing interview, she explained:
God heals, if you just have faith in Him.…It is by faith; God can do anything, the miracles are there, so it is up to you as an individual. (50-year-old woman)
Some PLHIV with financial means reported travelling outside Zambia, to South Africa or Nigeria, at great financial cost for healing sessions, while others bought ‘anointing water’ (spiritual water purported to have healing properties) from their respective churches. One respondent who had travelled to Nigeria for prayers bought a 100 mL bottle of ‘anointing water’ for US $100. Droplets of this anointing water were either added to drinking water, sprinkled on food or swallowed in the mouth. Ironically, even some ART support workers with HIV opted for faith healing instead of initiating ART. One PLHIV explained:
They told me to start treatment but then I was about to go to South Africa for prayers with my husband.…There, we were taught how to receive healing. We were learning about how to have faith, and how to receive healing.…When I came back, I went to the clinic to check my CD4 cell count and it had been boosted; from 165 to 365. So that is it. (37-year-old female ART support worker)
While some PLHIV who went for faith healing never re-tested to confirm their ‘new’ status, a few did. However, re-testing and still being found HIV positive did not lead to uptake of treatment:
There is this woman also who after testing HIV positive, she decided to go and consult a Pastor. The Pastor took her into the mountains for some days for prayers and fasting for healing. After that, the woman came back here and said she had tested positive but had gone for prayers.…We re-tested her and even told her how to read the results. The results still came out positive. She left without saying a word. (FGD, VCT lay counselors)
Although patient-reported benefits of ART appeared to contradict their reasons for not initiating treatment, these conflicting viewpoints intersected. For instance, while reluctance to start treatment was due to fear of side effects and perceived deleterious effects and concerns about future availability of treatment, PLHIV still reported willingness to start treatment if their health deteriorated. However, the use of herbal remedies and conventional non-HIV medication to mitigate HIV-related symptoms reduced the motivation to initiate treatment. One PLHIV explained:
“Yes, I have seen that some people that were very sick are now doing fine but those drugs, ARVs, are also bad for the body. That is why at the clinic, people do laboratory tests to find out how the drugs are destroying their bodies, like the liver. Me, I will only start when I feel that the sickness is more problematic now. For now, I just take herbs.” (29-year-old man)
Discussion
In our study of reasons for non-uptake of ART in an urban area of Lusaka, Zambia, several factors that undermined PLHIV uptake of ART were identified: subjective perceptions and experiences of health and treatment; stigma, peer and family influence, and experience; livelihood constraints and concerns about future availability of treatment; and ART delivery constraints and availability of alternative care. While the majority of the respondents were women, our findings suggest that the barriers to patient uptake of treatment were similar across men and women. From these findings, the following insights can be deciphered:
PLHIV measure their health in terms of functional ability and not clinical condition
Our study found that lay experience of health and treatment negatively affect treatment-seeking behavior. Individuals assess and perceive their health not only in terms of their clinical health condition as reported by their health care providers; rather, in terms of their corporeal health and functional ability 31 —being able to live ‘normal’ and ‘healthy’ lives and engage in productive activities and social lifestyles without recourse to treatment. The findings are consistent with other studies which showed that individuals understood illness in terms of feeling sick and therefore never sought treatment when asymptomatic. 5,32 These findings suggest that PLHIV are not passive recipients of ART care. They act as ‘naïve scientists' 33 and use ‘lay logic and reasoning’ 34 as a basis of deciding whether to initiate treatment. These lay assessments lead to delays to initiate ART and undermine recent HIV treatment policy changes which stipulate treatment initiation at higher CD4 cell count (from <200 to ≤350 cells/mm3) to reduce AIDS-related mortality and morbidity. 14,35 They also cast doubt about the viability of universal testing and immediate treatment as a way of reducing HIV incidence. 36
Quest to protect normalcy and social identity undermine uptake of treatment
While ART is crucial for long-term survival and its efficacy is indisputable, the assumption that individuals would prioritize treatment because of the associated biomedical benefits is not always the case. This is because, as our findings show, taking medication is a ‘meaning-filled subjective expression’ 37 and individuals conduct ‘cost-benefit analyses' 38 of medicine-taking, and treatment can be shunned if perceived to have negative impact on social image, social relationships, and social aspirations. Therefore, PLHIV avoid actions that would expose them as having HIV, especially if uptake of treatment threatens their social and economic networks or alters their lifestyles and aspirations. This explains why despite treatment being available, some PLHIV opted not to take it. Our findings mirror previous studies that have reported that some PLHIV did not initiate treatment because they did not want to be identified as having HIV. 39,40
Perceived long-term negative effects of treatment inhibits its uptake
The findings also suggest that uptake of treatment is undermined by perceived impact of medication on physical and physiological wellbeing. In our study, PLHIV did not want to start treatment because of the perceived toxicity of treatment. Interestingly, some PLHIV were concerned about the effects of treatment on their body shape. They were fearful of their bodies being ‘structure-less', ‘deformed,’ or ‘disfigured’ due to ART. For some PLHIV, physical changes to their bodies could limit their chances of finding marital partners. Also, there was a strong perception that despite improving corporeal health, the medication did more harm to the body in the long term. Previous studies have also found that PLHIV opted not to start treatment because side effects and drug toxicity were perceived as a threat to their physical and psychological wellbeing. 4,6,7 In our study, PLHIV drew on the negative experiences of close family members or friends and their death or declining health led them to conclude that treatment had deleterious effects and was insidiously harmful.
PLHIV regard food security as prerequisite for treatment uptake
Even when individuals are willing to start treatment, the findings suggest that its uptake requires navigating and overcoming broader structural-level factors. Structural factors are those non-individual-based circumstances present in the environment that influence health-seeking behavior but over which the individual has no direct control. 41,42 These comprise the economic, social, policy, organizational, or other aspects of the environment. 43 Although health system-level factors may be subsumed under structural-level factors, we have separated wider-level structural factors from health system-level factors in order to facilitate analysis and identify interventions that could specifically be aimed at addressing health system-level constraints. 41
Previous studies have implicated economic-related barriers as influencing patient uptake of treatment. 10,16,20,26,44 –46 In our study, it was neither the transport costs of accessing treatment nor the cost of medication that inhibited uptake of treatment because ART services were free and the health facility was conveniently located within the study area. Instead, inadequate income and household food insecurity dissuaded PLHIV from starting treatment due to the nutritional demands of being on treatment. Consistent with the findings of Unge and colleagues, 27 due to livelihood constraints, some PLHIV were often scared of taking strong HIV medication on an empty stomach as this was viewed as inimical to the effectiveness of treatment and their long-term health. They opted to postpone starting treatment until their livelihood conditions had improved.
Lack of trust in government and health system also undermine access to treatment
Structural conditions also entail national health policies related to funding and delivery of ART care. While ART has become widely available in many resource-limited settings like Zambia, our study found that the downside was the lack of trust in government's ability to sustain provision of treatment in the long-term in the absence of external support. Interestingly, for some of our research participants, the heavy reliance on donor support created anxiety about future availability of treatment.
These concerns need to be contextualized. Zambia is heavily reliant on external funding for HIV services. 15,47 HIV interventions are heavily funded by external support agencies with the Presidential Emergency Plan for AIDS Relief (PEPFAR) of the United States of America being the major contributor. 47 Therefore, any disruptions in the funding and supply of medication undermines people's confidence in government's ability to provide HIV treatment and care. For instance, the alleged embezzlement of donor funds at the Zambian Ministry of Health and the subsequent freezing of donor support by Global Fund to fight AIDS, Tuberculosis and Malaria (GAFTM) and other bilateral donors in 2010, which in turn led to periodic stock-outs and rationing of drugs 48 exposed the fragility of the HIV treatment program in Zambia. As UNAIDS Executive Director Michel Sidibe recently warned, the heavy reliance on external funding by countries heavily affected by HIV was “a source of great risk and potential instability. The status quo cannot be sustained.” 49 For some PLHIV, this unpredictability and fragility of treatment supply casts serious aspersions about future availability of treatment. Therefore, not starting treatment was construed as a rational individual strategy to avoid future negative health outcomes associated with discontinuation of treatment on account of its possible non-availability.
Faith healing and herbal remedies also reflect dissatisfaction with formal health care
Various studies have described the impact of faith healing 50 –53 and herbal remedies 28,54,55 on uptake of ART. Consistent with these findings, and unlike previous studies conducted in Zambia, 16 –18 the use of faith healing and herbal remedies were found to be prevalent in our study. Our findings suggest that opting for faith healing and herbal remedies was not based on ignorance of the benefits of antiretroviral treatment. Neither was it solely a reflection of individual health beliefs. Rather, it was also a response to dissatisfaction with the formal health care and perceived shortcomings of ART. Concerns about treatment side effects and toxicity, worries about sustainability of treatment, in addition to perceived low self-efficacy to be on life-long treatment resulted in individuals opting for herbal remedies and faith healing.
Interestingly and unlike previous studies, our findings suggest that factors undermining uptake of HIV treatment are inextricably linked and sometimes coalesce to affect treatment-seeking behavior (Fig. 2). For instance, while livelihood constraints such as food insecurity (structural factor) dissuades individuals from starting treatment, long waiting times at ART clinics (health system factor) also create opportunity costs, which exacerbate already fragile livelihood conditions, thus reducing the motivation to initiate treatment. Similarly, opting for alternative care (herbal remedies and faith healing) is as much a result of concerns about future availability of treatment (structural factor) as much as it is about fear of side effects and lack of self-efficacy (individual-level factors). We may also subsume the plethora of alternative treatments in view of a weak health system, but its use is shaped by individual treatment beliefs, which are perpetuated in social relationships with peers, family members, faith healers, and traditional medicine providers who not only exert influence but also provide information and share experiences (Fig. 2).
Nested relationships of factors influencing non-uptake of treatment.
Implications for policy and practice
At policy level, there is need for increased funding for HIV treatment from local resources rather than heavy reliance on external support. This would help build confidence in local capacity to deliver HIV treatment and assuage fears about future non-availability of treatment. Pronouncements by Zambian government officials to establish a national health fund to help hedge against unpredictable external financial support particularly for HIV treatment are a step in the right direction. Additionally, at global and national levels, efforts should be made to assess the therapeutic benefits of herbal medication, and authorize and regulate those found to have therapeutic value without undermining access to and effectiveness of ART. As the World Health Organisation (WHO) noted more than two decades ago, there is need “… to evaluate those elements of traditional medicine, particularly medicinal plants and other natural products, that might yield effective and affordable therapeutic agents.” 56 Such efforts to identify and promote certain herbal remedies should be counterbalanced by strong regulatory measures to avert proliferation of fake herbal medication.
The fragile food security situation of some PLHIV clearly demonstrates the impact of poverty on access to health care. As previously noted elsewhere, 16 while provision of food aid to vulnerable PLHIV may enable them initiate treatment, this could be difficult to sustain in the long-term due to the costs of providing such support in a poverty-endemic setting where access to formal social welfare programmes is very limited. Instead, funding for HIV should also prioritize livelihood empowerment programs for economically disadvantaged people living with HIV.
At service delivery level, efforts to improve uptake of ART should comprise close, open rapport between HIV testing/ART service providers and service users, and general sensitization campaigns, to ensure that (potential) HIV service users' negative health and treatment beliefs are identified, understood, and addressed. This also entails treating (potential) service users not merely as passive recipients of HIV information and services; rather as active agents and co-producers of good health outcomes. Attention should also focus on building confidence, self-esteem, and positive body image of PLHIV in the face of treatment-related side effects. Equally, focus should be placed on sensitization campaigns on the benefits of early initiation of treatment and dispel beliefs about perceived effectiveness of herbal remedies in the absence of scientific proof. Individuals that have sought faith healing should be encouraged to re-test for HIV. Additionally, sensitization campaigns should also target faith healers and herbalists about the benefits of ART and the dangers of unproven healing practices. As many people get onto treatment, there is also need for increased manpower in the ART clinics and adoption of longer, flexible clinic hours to avoid congestions and long waiting hours to help attenuate possible opportunity costs associated with seeking ART care. This has policy implications as it requires increased funding for additional health workers.
Possible limitations of the study
Some PLHIV were recruited in the community through their caregivers or snowball sampling, and their eligibility for the study was based on self-reports of being eligible for treatment. Consequently, this recruitment strategy could have led to some clustering of shared ideas and views. However, more than three-quarters of our study participants were identified, contacted, and recruited through the ART clinic. The clinic staff were aware of which individuals had declined ART, despite it being recommended to them, suggesting that our sample largely comprised treatment-eligible PLHIV who were independent from each other. Also, more women than men were recruited due to the difficulties of recruiting men for the study. The reasons included: some men refused to be interviewed; many were mobile due to their livelihood activities; and others were no longer in contact with the health system in the area and not attached to home-based care providers. However, as the findings suggest, the reasons for non-uptake of treatment were similar between men and women. Future studies should aim to explore this further.
A more general limitation concerns the generalizability of the findings. This study was conducted in a low-income setting with a small sample of respondents and aimed at identifying a wide range of themes rather than getting a representative sample. Similar studies are therefore needed in other settings, especially targeting people in higher socio-economic strata. Despite these possible limitations, our study is probably generalizable to similar settings in urban areas in the country and provides useful insight that can inform policy and practice to improve ART uptake.
In conclusion, using the social ecological framework, our findings suggest that patient non-uptake of treatment is complex and dynamic, and is influenced by interplay of individual-level and contextual factors outside the direct control of the individual. Individual health and treatment beliefs undermine treatment initiation and these are generated and perpetuated through close social network influence and experiences. Even for those willing to start treatment, the necessity and utility of treatment is counteredbalanced by concerns about future supply of treatment, perceived opportunity costs of seeking treatment, and by attempts to preserve physical, mental, and social wellbeing. This balancing act is mediated by the state of corporeal health, faith healing, and availability of herbal remedies which are perceived as effective as ART but with perceived less side effects and less arduous treatment requirements. Thus, ensuring that PLHIV initiate treatment requires addressing individual health and treatment beliefs through close patient–provider rapport and sensitization campaigns targeting faith healers, herbalists, and wider community members. Efforts should also be made to assess the therapeutic value of herbal remedies and enforce pharmaceutical measures to regulate their supply and use. There is also need for improved resource allocation for HIV treatment to ensure sustainability of care and for efficient delivery of ART services. Strong inter-sectoral collaboration is also needed to support economically vulnerable individuals who cannot access treatment due to income/food insecurity concerns.
Footnotes
Acknowledgments
The study was funded by the Swiss National Science Foundation (SNSF) through the project ‘Improving equity of access to HIV care and treatment in Zambia.’ The authors are grateful to the home-based care providers and ART staff of a local public health centre that helped identify and recruit research participants; and the research participants for agreeing to share their time and experiences.
The views expressed in this article are those of the authors and do not necessarily represent the views of the funding agency. The funding agency played no role in the design and conduct of the study; the interpretation of the data; and the write up of this article.
Author Disclosure Statement
No competing financial interests exist.