
Abstract

Dear Editor,
Out of 81 eligible cases; 32 entered care ≤1998 and 49 afterwards. There were no differences between the groups in age, gender, transmission category, baseline CD4 count, baseline plasma viral load, length of time followed, or CXCR4 tropism. There was a statistically significant association between the period of diagnosis and time to T CD4+ cells decline to ≤350 cells/mm3 (log rank p<0.001). Before 1998, the mean time to a CD4 count of 350 cells/μL was 2.43 (95% CI 1.70–3.15) years and from 1998 and later 7.03 (95% CI 5.63–8.42) years (Fig. 1). This adjusted hazard ratio was 0.17 (95% CI 0.08–0.32), corresponding to a decline of 56.68 cells/μL/year before 1998 and 49.74 cells/μL/year in 1998 and later. Having CXCR4 tropic HIV (HR, 3.1, 95% CI, 1.2–7.8) was statistically associated with progression to CD4 count ≤350 cells/μL. Despite the clinical impression that treatment-naïve patients are progressing more rapidly in the ART era, we found that CD4 cell counts were, in fact, declining less rapidly in 1998 and later than before 1998. We also found that CXCR4 tropic viruses were associated with faster progression disease, as have other authors, 1,4 but the differential presence of CXCR4 tropic viruses did not explain the changes we observed. Our study was limited by its small sample and irregularly sampled CD4 cell measurements, especially before 1998. Larger and more regularly sampled cohorts may have different results. Nonetheless, our findings are compelling and suggest slower CD4 cell declines in treatment-naïve patients in the era of effective ART. The mechanism for this is not clear. Additional studies will facilitate the identification of factors that may underlie this trend.
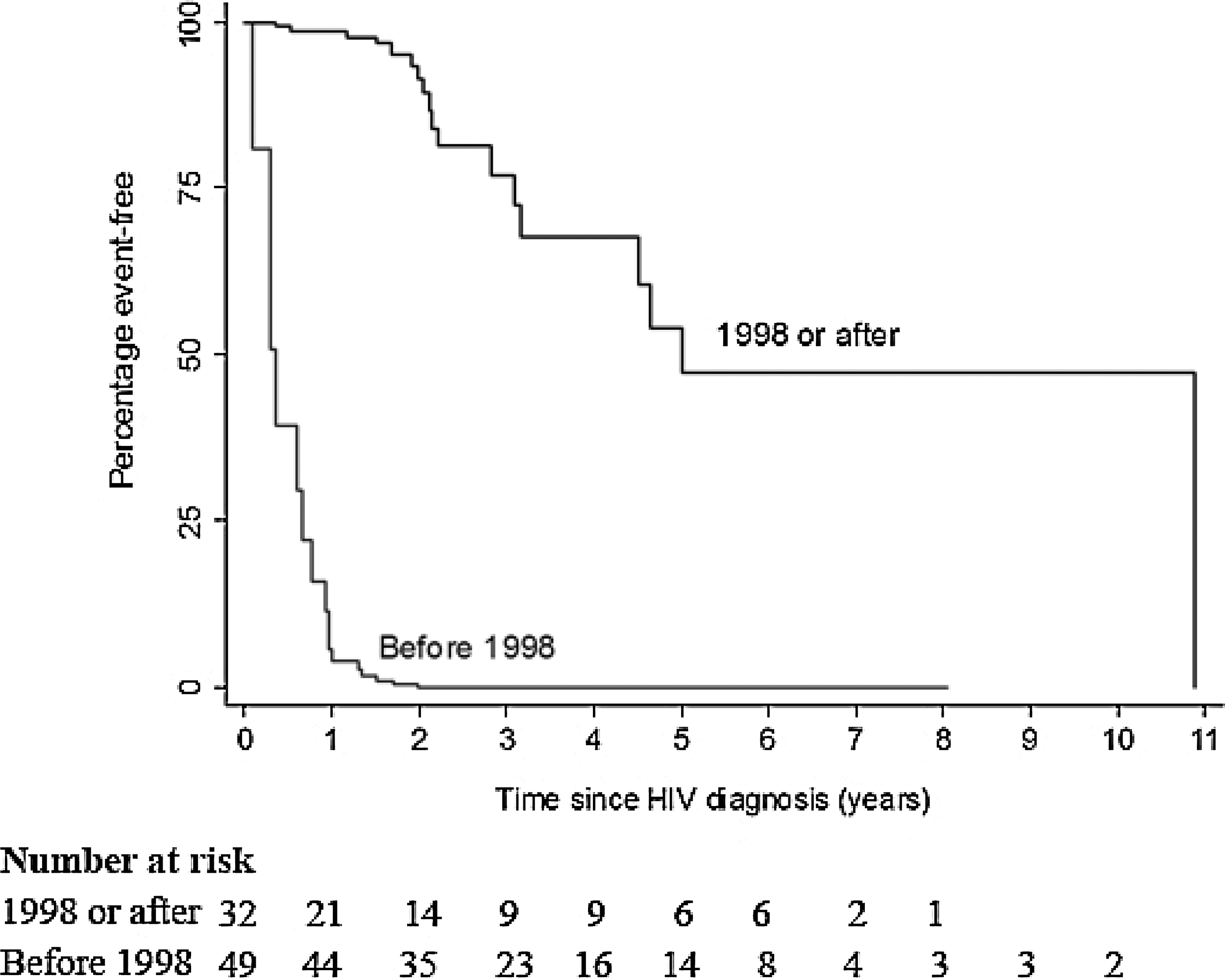
Survival curves to CD4 less than 350 by ART era (before and after 1998) adjusted for covariates (age, gender, HIV follow-up time, and CD4 at baseline).
Footnotes
Acknowledgments
The first author (DC) received support through the University of California San Francisco from U.S. National Institutes of Health (NIH) Fogarty International Center (FIC), D43TW005799 and National Institute of Mental Health (NIMH) International Traineeships in AIDS Prevention Studies (ITAPS), R25MH064712, and HIV Research Trust Scholarship (HIVRT), HIVRT11-074. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, NIMH, FIC, or HIVRT. We all thank the patients who participated in this study. We also thank Claudio Gonsalez, Marcelo Mendonça, Eduardo Lago Negro, and Lucas Medeiros for clinical assistance.
Author Disclosure Statement
No competing financial interests exist.