
Abstract
The prevalence of HIV-positive pregnant women in relationships with HIV-negative men in the United States is unclear. The purpose of this study was to calculate the prevalence of HIV-positive pregnant women with a serodiscordant (HIV-negative) partner within a single clinic population, assess disclosure of their HIV status, and examine factors associated with disclosure. All HIV-positive pregnant women who received prenatal care at the Harris County Hospital District Women's Program at Northwest Health Center in Houston TX between 1/1/2006 and 4/1/2011 were identified. Data were obtained from electronic medical records. Prevalence of serodiscordance and disclosure was calculated, and predictors of disclosure were evaluated. We identified 212 HIV-positive pregnant women. About 40% had a serodiscordant partner, and 34% had a partner with an unknown HIV status. Disclosure occurred in over 90% of women with a serodiscordant partner and in 68% of women with partners whose HIV status was unknown. Among pregnant women who knew their HIV status prior to the current pregnancy and had a serodiscordant partner, 92% reported disclosing their status prior to conception. Our data indicated that serodiscordant relationships are common in our clinic population. Suboptimal disclosure rates were observed, especially among women who have a partner with an unknown HIV status. Further research is needed to evaluate the prevalence of serodiscordance and disclosure in other United States populations.
Introduction
Many women who are HIV-positive have partners whose HIV status is either negative or unknown. If one partner is HIV-positive and the other is HIV-negative, the couple is referred to as serodiscordant, (sometimes also described as magnetic, mixed, serodifferent, or serodivergent). 7 In a study by Heard conducted in France among a cohort of 555 women between the ages 18–44 years with known HIV for at least 6 months, 76% of HIV-positive women were in serodiscordant relationships and 15% had partners whose HIV status was unknown. 8 Little data are available on the number of HIV-positive pregnant women in serodiscordant relationships. Findings show that serodiscordant couples will risk HIV transmission in order to conceive a child. 9,10 Serodiscordant couples who engage in sexual activities without using safe sex practices run the risk of HIV transmission to the negative partner. Consistent use of condoms with each episode of intercourse decreases the risk of HIV transmission by >85%. 11 Additionally, condoms protect against other sexually transmitted infections (STIs), which have been shown to increase the risk of transmission and accelerate the progression of HIV illness. 12 However, condoms also prevent pregnancy.
There is solid evidence that the use of HAART successfully lowers transmission rates of HIV infection from mother to baby, but less information is available on how to protect an HIV-negative man during intercourse with an HIV-positive woman while attempting conception. In the United States, studies have shown that during unprotected heterosexual intercourse with an HIV-infected partner, women have a greater risk of becoming infected than uninfected men. 13 Strategies have evolved that allow serodiscordant couples to successfully and safely achieve pregnancy while decreasing the risk of HIV transmission to the uninfected partner. The safest method uses ovulation predictor kits to determine the timing of ovulation during the woman's menstrual cycle. Home insemination is then used to achieve conception while virtually eliminating the risk of HIV transmission from the HIV-positive woman to her negative partner. This technique, also known as the “turkey baster” method, is accomplished by collecting the man's ejaculate and transferring it into the woman's vagina via a syringe. 4,14 Serodiscordant couples can choose to use condoms with every episode of sexual intercourse, and still attempt pregnancy with home insemination. Not all couples favor the technical details of home insemination, however, and choose to use an ovulation predictor kit followed by having sex without using condoms during the time of optimal fertility. 5 Though there is some risk of HIV transmission during these episodes of unprotected sex, at all other times during the month the couple uses condoms to protect the HIV-negative partner from transmission. In this scenario, the HIV-positive woman follows a regimen of antiretroviral medication to reduce viral load prior to conception attempts, thus lowering the chance of transmission to the negative partner. An undetectable viral load makes transmission less likely, 15 though there is evidence that the viral load in the plasma may not correlate exactly with the viral load of the genital compartment. 16 The newest strategy is for the HIV-negative partner to take prophylactic antiretroviral medication before exposure or possible exposure to HIV. This regimen, known as pre-exposure prophylaxis (PrEP), has shown promising results from ongoing clinical trials. The iPrex study showed partial effectiveness in inhibiting HIV transmission in high-risk populations [men who have sex with men (MSM) and transgender women who have sex with men]; the risk of acquiring HIV infection was reduced by >43% in HIV-negative participants who took a daily oral dose of antiretroviral medication. 17,18 Recent studies evaluating the effectiveness of PrEP taken by HIV-negative men in sexual relationships with HIV-positive women reported that PrEP is associated with a 63–72% reduction in HIV transmission. 10,19,20 However, use of PrEP is only possible once HIV status is disclosed.
Past studies have looked at HIV serodiscordance and disclosure in other countries and the United States, but serodiscordance and disclosure among HIV-positive pregnant women in the United States has not been well studied. Siriwasin 21 reported on 342 pregnant women in Thailand; 90% had disclosed their status to their partners and 26% had HIV-negative partners. Two South African studies reported 59% disclosure by pregnant women; being married, higher level of partner's education, and less history of violence was positively associated with disclosure; qualitative analysis revealed that women went through a process of considering the risks of being abandoned and discriminated against versus their desire to protect partners and seek support. 22,23 A 2008 study in Nigeria found an 80% serodiscordance rate in an antenatal clinic; 88% of the 166 women had disclosed to their partners; nulliparity and being unmarried were variables associated with nondisclosure. 24 Fear of others learning of their HIV status and loss of partner relationship were reasons given for not disclosing.
Whether a woman discloses may depend on the nature of the relationship, length of time with a partner, and whether a partner has been tested for HIV, according to a study in Kenya; the authors reported a 50% disclosure rate in the first year after diagnosis, with the majority disclosing within 3 days of a positive test. 25 In the U.S., Serovich et al. followed women over a 15-year time interval and found that 58% of women had disclosed to their partners within one year after diagnosis; 86% of women had disclosed at the conclusion of the study. 26 A recent study from South Africa found that disclosure is not necessarily a single event; in some cases a woman may disclose and later deny she disclosed. 27
There is a paucity of studies examining serodiscordance and disclosure among HIV-positive pregnant women in the United States. Using data obtained from electronic medical records, a retrospective cohort study was conducted to establish the prevalence of serodiscordance and disclosure as well as patient factors associated with disclosure among all HIV-positive pregnant women who received prenatal care from the Harris County Hospital District Women's Program at Northwest Clinic between 2006 and 2011.
Methods
Study population
All HIV-positive pregnant women who received prenatal care at the Harris County Hospital District (HCHD) Women's Program at Northwest Health Center in Houston, Texas between January 1, 2006 and April 1, 2011 were identified. Northwest Health Center (NHC), affiliated with Baylor College of Medicine (BCM), is one of 14 outpatient clinics administered by the HCHD that provides primary care services to adults and children in the Houston/Harris County area. NHC manages approximately 48,000 patient visits per year, with specialty services including obstetrics and gynecology as well as HIV/AIDS care.
Study data
All data were obtained from electronic medical records (EMR). For women with more than one pregnancy in 2006–2011, only the first pregnancy following their HIV diagnosis was considered. Demographic characteristics including age at conception, ethnicity, preferred language, country of birth, and marriage status were recorded. Variables related to pregnancy history included gravidity, parity, and estimated gestational age at first prenatal care visit. HIV-related information included date of HIV diagnosis, prior HIV care, CD4 count, viral load, prior use of antiretroviral medication, and HAART use in the current pregnancy. The partner's HIV status as well as disclosure status was also recorded. Discordant status was determined based on patient report of the HIV status (positive, negative, unknown) of the partner. If disclosure had occurred, the time of disclosure was recorded.
Statistical analysis
The prevalence of serodiscordance and disclosure was calculated among all HIV-positive pregnant women identified for this study. Among women in a serodiscordant relationship with known HIV prior to pregnancy, demographic and clinical characteristics were compared between women who disclosed their HIV status and those who did not. A similar analysis was conducted among women having a partner with unknown HIV status. Continuously measured variables were compared using an independent, two-sample t-test assuming equal variances. Categorical variances were compared using Fisher's exact test. Statistical significance was evaluated assuming a 0.05 Type 1 error rate.
This study was approved by the Institutional Review Board at the Baylor College of Medicine and the Harris County Hospital District Office of Research.
Results
A total of 308 electronic medical records were reviewed; 63 women did not satisfy the inclusion criteria. Inclusion criteria for this study were (1) ages 18 and older; (2) confirmed pregnancy; (3) confirmed HIV-positive status; and (4) seen by a provider at the obstetrics and gynecology clinic at the NHC. An additional 33 pregnancies were excluded because they were repeated observations (more than one pregnancy) by the same women.
The final study cohort consisted of 212 unique, pregnant women diagnosed with HIV either prior to pregnancy or at the time of initiating prenatal care (Fig. 1). Approximately 57% of these women were black, 26% were Hispanic, 6% were white, and 11% were unknown race. About 58% were born in the United States, and 60% were single. Among the entire sample of HIV-positive pregnant women, 40% reported disclosing their HIV status to their partner prior to pregnancy.
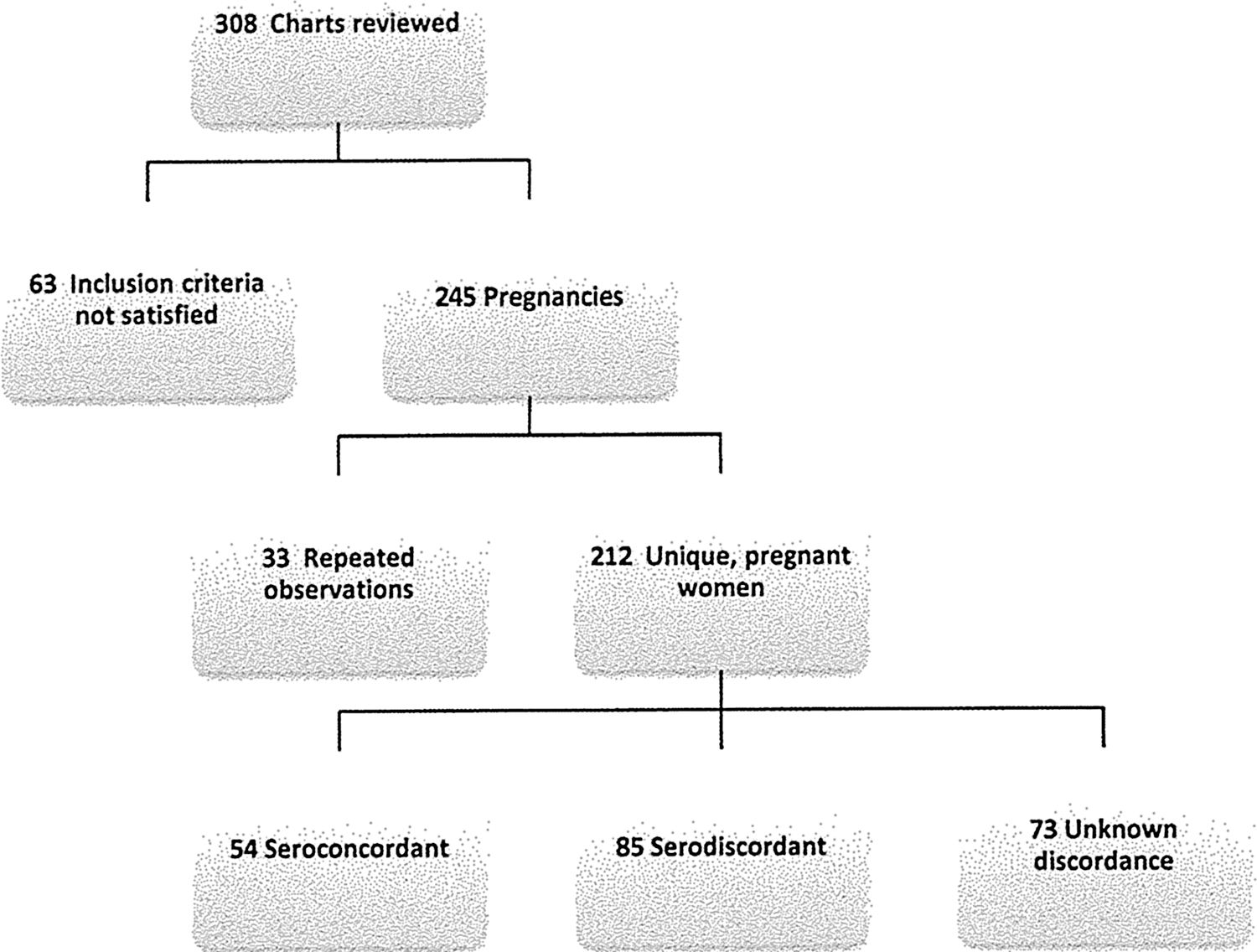
Study population flowchart.
Approximately 40% (n=85) of HIV-positive pregnant women in this clinic population of 212 HIV-positive pregnant women were in a serodiscordant relationship. Most of these women were black (69%) and were born in the United States (71%). Over 36% had CD4 counts <500 cells/μL at the time of their first prenatal visit, and 25% had detectable viral loads of >400 copies/mL.
Serodiscordance and disclosure
Among the 85 women with a serodiscordant partner, 75% (n=64) knew that they were HIV-positive prior to the current pregnancy. Almost 70% of these women were black, 73% were born in the United States, and 61% were single. About 48% had CD4 counts <500 cells/μL at their first prenatal appointment and 32% had a detectable viral loads of >400 copies/mL at the initial prenatal visit. Sixty percent of these women had received HIV care at least once in the 6 months prior to this pregnancy, and 61% had been on HAART within the 12 months prior to the current pregnancy. Among women who were known to be HIV-positive prior to pregnancy, 92% disclosed their HIV status to their partner prior to the pregnancy. No differences in disclosure were observed by demographic or clinical characteristics (Table 1).
Women in relationships with partners with unknown HIV status
About 34% (n=73) of the 212 HIV-positive pregnant women identified for this study had a partner with an unknown HIV status. Two-thirds of these women were black, 60% were born in the United States, and 70% were single. Among the 29 women who were known to be HIV-positive prior to pregnancy but had a partner of unknown HIV-status, 67% received HIV care within 6 months of conceiving and 62% were on HAART within 12 months of the current pregnancy. Only 68% of women who were known to be HIV-positive disclosed their HIV status to their partner prior to the pregnancy.
Discussion
The purpose of this study was to examine serodiscordance in pregnant HIV-positive women. We found that 40% of HIV-positive women were in serodiscordant relationships, and 34% had a partner of unknown HIV status. Over 90% of women in serodiscordant couples disclosed their HIV status compared to only 68% of women having partners of unknown status. However, it is important to note that in relationships where disclosure has not occurred and the woman reports that her partner has an unknown HIV status, unknown HIV status could be reported because the partner had not been tested for HIV or the couple had not discussed their HIV status prior to pregnancy.
A significant number of women are having children with serodiscordant partners. Questions asked of HIV-positive pregnant women during pregnancy planning as well as during prenatal visits are critical. Whether protective measures are put into place to ensure that the uninfected partner is aware of the woman's status and whether he is knowledgeable about how to remain safe during conception attempts are important for providers to know when developing counseling techniques for these couples. As progress is made in the development of PrEP for heterosexual individuals and as HAART therapy continues to allow suppression of viral replication, providers can educate patients about risks associated with HIV transmission during conception attempts and how to minimize transmission to the uninfected partner.
An incidental discovery in this study revealed that a large percentage of men (34%) in this cohort have an unknown HIV status. This information could significantly impact the serodiscordant rate in this study; had the 34% of these men been tested for HIV and found to be negative, the range of serodiscordance increases from 40% to 74%. A challenge for healthcare providers exists in targeting the population of men who have not been tested for HIV yet engage in sexual intercourse with HIV-positive women. This is a subgroup with needs for counseling and services that differ substantially from the cohort of those individuals already infected. An opportunity exists in pregnancy planning with HIV-positive women to link their partners to care by encouraging HIV testing as well as providing ways to protect the man from HIV transmission.
Several previous studies have examined serodiscordance and disclosure; however, studies examining these issues in pregnant women have mostly been done outside of the United States. Siriwasin reported a surprisingly high rate of disclosure (90%) and low rate of serodiscordance (26%) in Thailand during the 1990s, 21 when one would expect stigma to have been greater (prior to access to antiretroviral therapy) than now. Disclosure among HIV-positive pregnant women has been assessed in South Africa, 22,23,27 Nigeria, 24 and Kenya 25 —all nations where stigma has tended to be greater than in the United States, possibly because antiretrovirals have been available longer in the United States, people are living longer, and discrimination against people living with HIV has diminished. Serovich and colleagues also investigated HIV disclosure over time among women in the midwestern United States; however, they did not focus on pregnant women. 26
Ours is one of few studies that have examined serodiscordance and disclosure in HIV-positive pregnant women. However, the limitations of this study must be acknowledged. This study relied on information obtained from the medical record, including self-reported information provided by the HIV-positive pregnant woman to the healthcare provider. As with all self-reported information, the potential exists for inaccurate testimonials because of the sensitive nature of the topic. Limited information was also available about the use of HIV transmission prevention measures while trying to conceive. Also, African women and African-American women were categorized together as “black,” which may have masked cultural differences. Lastly, although we observed a high rate of serodiscordance in our clinic population, these findings may not be generalizable to other study populations.
Gaps exist in our current model of HIV prevention, as rates of serodiscordance and disclosure from an HIV-positive pregnant woman to her discordant partner have previously not been well quantified. Efforts to provide acceptable options for these couples who wish to get pregnant safely have been limited, in part because the level of need has been unclear. Clinical implications for healthcare providers are numerous. Practitioners need to address disclosure and provide women with strategies as to how to disclose their HIV status. Awareness of a woman's positive HIV status may provide incentive for the negative partner to learn about techniques that protect the HIV-negative partner prior to conception and when trying to conceive. Clinicians also need to be able to explain or refer couples for an explanation of these techniques for safer conception (e.g., use of ovulation predictor testing, home insemination, timed unprotected intercourse with a partner who is on antiretroviral therapy and who has an undetectable viral load, and PrEP). Questions about desire for pregnancy and possible need for pregnancy planning need to be asked, not only at the time HIV-infection is confirmed but repeated at subsequent visits. Templates within the burgeoning options of electronic medical records may be used to remind clinicians of what they need to ask and when. Documentation efforts should be increased to include partner HIV status and methods utilized to attain pregnancy.
In conclusion, we identified a high rate of serodiscordant relationships among HIV-positive pregnant women and suboptimal rates of disclosure of HIV status, particular among HIV-positive women who have a partner with an unknown HIV status. Our results suggest that mixed HIV status does not preclude people from engaging in sexual intercourse and having children. Education of clinicians and individuals living with or affected by HIV on how to lower and prevent periconceptual transmission to the HIV-negative partner is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.