
Abstract
HIV-infected patients are at increased risk for developing HIV-related Hodgkin lymphoma (HIV-HL) despite the success of combination antiretroviral therapy (cART). To study the incidence of HIV-HL in HIV-patients with respect to the general population of Brescia, Italy, we conducted a single-center cohort study of HIV-patients followed from 1999 to 2009. The incidence of HIV-HL was compared to the incidence in the general population of Brescia using standardized incidence ratios (SIRs). Poisson analysis was used to study the association between covariates and HL. A total of 5085 HIV-patients were observed among 30,946 person-years; 30 patients developed HIV-HL. The incidence rate was 9.9 (95% confidence interval [CI], 6.7–14.1) per 10,000 person-years of follow-up. HL was substantially more frequent in HIV-patients than in the general population living in the same district area [standardized incidence rate, SIR=21.8 (95% CI, 15.33–31)]. The risk of HIV-HL tended to increase with lowering CD4+ cell counts at time of HL diagnosis [adjusted incidence relative risk (IRR) for CD4 cell count<50 cells/μL: 41.70, p<0.001]. HL risk had been elevated during the 6 months after combination antiretroviral therapy (cART) initiation (IRR: 26.65, p<0.001). Twenty-two HIV-HL cases were matched to 3280 controls. In the year preceding HIV-HL diagnosis the mean change in CD4+ cell counts between cases and controls was significantly different (-99 cells/μL for cases vs. +37 cells/μL for controls, p<0.0001). Compared with the general population, HIV-infected patients showed an increased risk for developing HL. The risk of HIV-HL increased significantly in the first months after cART initiation.
Introduction
The clinicopathological characteristics of HIV-related HL (HIV-HL) are widely reported to differ from those of HL in HIV-uninfected population. 11 HIV-HL is characterized by a more aggressive clinical presentation, with an unfavorable histological subtype as opposed to the predominant nodular sclerosis histological subtype observed in HIV-negative young adults. Indeed, histological subtypes of HIV-HL are predominantly mixed cellularity (MC)—in > 50% of cases—followed by lymphocyte depletion (LD) and the predominant subtypes are rich in neoplastic cells named Reed-Sternberg (RS) cells. From a clinical standpoint, >75% of patients at the time of diagnosis present “B” symptoms (i.e., fever, night sweats, and/or weight loss of >10%), a higher percentage of stage IV disease, according to Ann Arbor classification, with a greater involvement of extra nodal sites (bone marrow, liver, and spleen being the most frequent sites). 11 Moreover, Epstein Bar virus (EBV) co-infection is present in 80% out of 100% of HL cases among HIV-infected patients, 12 while in the general population EBV is present in around half of all HL cases. 13 The prognosis of HIV-infected patients with HL has considerably improved with the introduction of cART and it approaches that of the general population when they are treated with Hodgkin's tailored combination chemotherapy. 14 Nevertheless, in the cART era, rates of deaths due to non-AIDS malignancies, such as HIV-HL, and cardiovascular disease are increasing. To our knowledge, only one study has explored HL risk in Italy after the introduction of potent cART in 1996. 15 In this record-linkage study, an increased risk in HL was found (standardized incidence rate, SIR 20.7) among 37 HL patients from the Italian AIDS Registry. However, the reliance on AIDS case limited this analysis mainly to late presenter patients who had never taken cART and were severely immune-compromised.
The aims of this study were to assess the incidence of HL in a large single-center cohort of HIV-infected patients, with or without AIDS events with respect to the general population living in the same area, and to evaluate the possible factors for HIV-HL occurrence.
Methods
Patients and definitions
We conducted a retrospective cohort study from January 1999 through December 2009 of HIV-infected patients residing in the Local Health Authority (LHA) of Brescia (Northern Italy) and followed in the University Division of Infectious and Tropical Diseases of the University of Brescia. LHA has a population of >1.1 million inhabitants; 16 it is the first Italian province for HIV incidence and the third province when considering HIV prevalence. 17 Moreover, general characteristics of our study population are similar to those described in other Italian multi-center cohorts. 18,19 Both cART-naïve and experienced HIV-infected patients who were >18 years of age at cohort entry have been included in the analysis.
The study was approved by the local institutional review board and the patients gave written informed consent for the collection of their data at the first visit of follow-up. Sociodemographic characteristics, laboratory test results, treatments for HIV/AIDS, clinical complications including opportunistic infections, cancer, and death were recorded on a regular basis. These data were all included in the electronic database utilized for routine management.
HL diagnoses were retrieved from this electronic database and combined with those recorded in the administrative database of the Local Heath Authority (LHA) of Brescia and of the population-based Cancer Registry of the LHA: the details of this record-linkage between our clinical database and the LHA general database and the Cancer Registry has been described elsewhere. 20 All HIV-HL cases were defined on the basis of histological exam.
We excluded malignancies already diagnosed at the start of observation or that occurred prior to HIV-infection diagnosis or with inadequate clinical history and follow up.
Cancer type or site were coded according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision (World Health Organization, 1992). 21
For each person included in the study, the relevant time period for the calculation of person-years at risk began on January 1, 1999 or at the date of enrollment in the cohort and it ended with cancer diagnosis, last follow up visit, December 31, 2009 or death, whichever came first.
Baseline CD4+ cell count was defined as the first CD4+ count measured during a visit after January 1, 1999. The baseline plasma HIV-RNA viral load was taken as the closest measurement to the baseline CD4+ cell count. The nadir CD4+ cell count was defined as the lowest CD4+ cell count ever measured. In patients who developed HIV-HL, the nadir CD4+ cell count had to be measured before the diagnosis of HL. We defined cART as a regimen with at least three antiretroviral drugs from at least two drug classes, including protease inhibitors (PIs), nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and fusion inhibitors (FIs).
Statistical analyses
The incidence rates (IRs) of HIV-HL and their 95% confidence intervals (95%CI) were determined using the number of individuals at risk by year and were age-adjusted. The expected number of HL was calculated by multiplying the person-years at risk by appropriate age- and gender-specific incidence rates, as derived from the incidence rates obtained from the Cancer Registry of Brescia LHA in the general population for the periods 1999–2001 and 2004–2006, standardized by age. Age-standardized incidence ratios (SIRs) and their corresponding 95%CIs (Poisson distribution) were calculated as the ratio between observed HL incident cases recorded in HIV-infected patients and expected numbers of HL cases during the study period. The beta coefficient of the regression line of age-standardized incidence rate for HIV-HL per year of follow-up was considered as a measure of linear trend of cancer frequency over the period.
Poisson regression analysis was used to evaluate the univariate and multivariate associations between covariates and cancers. A p value of 0.05 was used for all the two-tailed statistical tests. Age, reported HIV risk behavior, sex, and prior AIDS event were included in the fitted models as possible confounders, regardless of statistical significance. For all other variables, only those with a p value<0.05 at univariate analysis were included in the multivariate model.
Results are presented as medians with interquantile ranges (IQRs), incidence rates per 10,000 person-years.
To examine if the change of CD4+ cell count during the year before HIV-HL diagnosis had a predictive role in HL occurrence, a complementary nested case-control analysis was also undertaken. HIV-infected patients with <12 months of follow-up before the event or CD4+ cell count missing at that time-point were excluded from the analysis. For HL cases, we considered the CD4+ cell count 12 months before the diagnosis of HL. For controls (we considered all patients of the cohort who were not diagnosed with HL during the follow-up) CD4+ cell counts were extracted from our database 12 months before the reference date, defined as the date after an identical median length of follow-up since entry in the cohort as cases.
All analyses were performed using STATA 12 (StataCorp LP, College Station, Texas).
Results
Baseline characteristics of cohorts and patients
The database included a total of 5086 patients followed in the University Division of Infectious and Tropical Diseases of the University of Brescia during the period 1999–2009. Median age was 36 years (IQR, 31–41) and most patients were males (n=3642, 72%) and born in Italy (n=4163, 82%). Intravenous drug use was the most frequent risk factor for HIV transmission (43%), followed by heterosexual contact (35%), and male homo/bisexual contact (16%). The median baseline CD4+ cell count was 336 cells/μL (IQR, 171–527 cells/μL) and the median plasma viral load was 6915 copies/mL (IQR, 279–54,000 copies/mL). We identified 31 cases of Hodgkin lymphoma (HL) between 1999 and 2009. One case was excluded from further consideration owing to inadequate clinical history and follow up.
Table 1 compares the 30 patients who developed HIV-HL with the 5055 who did not. No statistically significant differences were found.
Baseline indicates first visit after January 1, 1999. HL, Hodgkin lymphoma; IQR, interquartile range.
Clinical characteristics of patients at the time of Hodgkin lymphoma (HL) diagnosis
Table 2 shows the characteristics of the 30 patients with HIV-HL at the time of cancer diagnosis. More than half of the patients were current smokers, 13 (43%) patients were former drinkers, and two (7%) had a history of alcohol abuse. A family cancer history was present in 13 (43%) patients.
Treatment was heterogeneous with regard to the type of regimen and the number of cycles applied. Seven patients received Stanford V regimen (12 weeks with doxorubicine, vinblastine, mechlorethamine, vincristine, bleomycin, etoposide, and prednisone), 14 the VEBEP regimen (vinorelbine, epirubicin, bleomycin, cyclophosphamide, and prednisone) plus involved-field radiotherapy applied in 6 among these cases, and 2 the ABVD scheme (doxorubicin, bleomycin, vinblastine, dacarbazine). One patient received R-CHOP (monoclonal antibody rituximab, cychlophosphamide, doxorubicin, vincristine, prednisone) for concomitant non-Hodgkin lymphoma and one COPP-ABV (cychlophosphamide, vincristine, procarbazine, prednisolone/adryamycin, bleomycin, vinblastine) hybrid chemotherapy. Eight patients also received second line chemotherapy, due to the progression of the disease (n=5) or to the HL relapse (n=3).
cART, combination antiretroviral therapy; IQR, interquartile range; HIV-HL, HIV-related Hodgkin lymphoma.
HIV-HL diagnosis occurred at a median age of 42 years (IQR: 36–45 years), after a median of 9 years (IQR: 1.5–13 years) from the diagnosis of HIV. One of the patients (3%) received a diagnosis of HIV infection and HL simultaneously. Eleven patients (37%) had a previous AIDS event, and 3 patients (10%) had an AIDS-defining disease at the same time of HL diagnosis. Nodular sclerosis was the most common subtype occurring in 9 (30%) of the 30 patients, followed by mixed cellularity occurring in 3 (10%). Most patients presented with advanced-stage disease (57%), with systemic “B” symptoms and extra-nodal involvement (60%).
Five out of 30 patients (17%) did not receive any antineoplastic treatment because the performance status was too poor (n=4) or HIV-HL was diagnosed postmortem (n=1). Twenty-four of 30 patients (80%) underwent curative intended chemotherapy (Table 2).
At the end of the study, 11 patients had achieved the complete remission and were alive and disease free. Median time on remission after antineoplastic treatment was 1.372 days (IQR: 1064.5–2182.5 days). Of the 19 patients who died, the cause of death in 17 was HIV-HL, one patient died of AIDS, and one of an unknown cause. Excluding the patient with a postmortem diagnosis, median survival after HL diagnosis was 197 days (IQR: 79.5–461.5 days).
Incidence rates and risk factors for developing HL
The incidence rate (IR) was 9.9 (95% confidence interval, CI 6.7–14.1) per 10,000 person-years. HL was substantially more frequent in HIV-infected patients compared with the HIV-negative population living in the same health-district, (SIR=21.8, 95% CI 15.3–31), with a higher incidence of HL cases in women (SIR=23.1, 95% CI 11.6–46.3) than in men (SIR=21.4, 95% CI 14.2–32.2). Table 3 shows the number of HIV-HL cases, person-years of follow-up, IRs, and crude and adjusted incidence relative risk (IRR).
Adjusted for age, sex, HIV risk behavior, AIDS event, duration of cART treatment, CD4 cell count at cancer diagnosis, HIVRNA at cancer diagnosis. cART, combination antiretroviral therapy; 95%CI, 95% confidence interval; HBsAg, HBV surface antigen; HCVAb, HCV antibody; HL, Hodgkin lymphoma; IRR, incidence relative risk.
The annual standardized incidence rates for HIV-HL are shown in Fig. 1. A constant standardized incidence rates was observed overtime (rates ptrend=0.29).
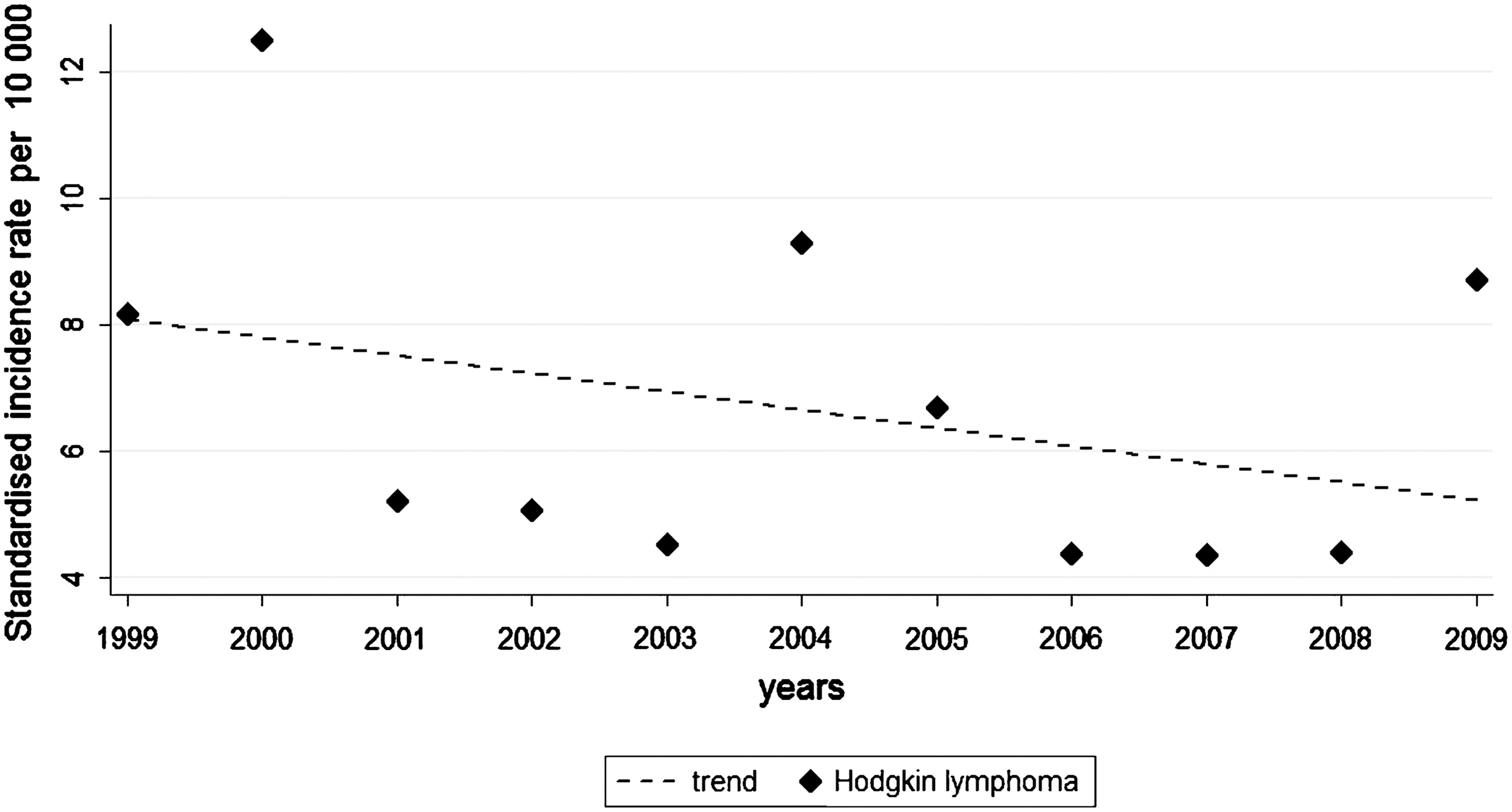
Standardized incidence rates for HIV-associated Hodgkin lymphoma overtime.
The univariate analysis (Table 3) showed that the risk of HIV-HL increased significantly soon after cART initiation, with a higher risk in the first 6 months of therapy (IRR 13.60, 95% CI 5.23–35.41, p<0.001). The strong association with the initiation of cART remained when adjusted for age, gender, risk group, prior AIDS event and CD4+ cell count, and plasma viral load at the time of HL diagnosis. In the multivariable analysis (Table 3), the risk was also increased in patients with CD4+ cell counts<50 cell/μL at the time of HL diagnosis (p<0.001) with CD4+ cell counts between 50 and 100 cells/μL (p=0.005), compared with patients with CD4+ cell counts of 350 cell/μL or more. In contrast, when current CD4+ count and ART use were considered, HIV load was unrelated to HL risk (p=0.13).
Case-control study of CD4+ cell count
For the analysis, HIV-HL cases with at least 12 months of follow-up before the event and CD4+ cell count available were selected. Twenty-two HIV-HL patients were matched to 3280 controls. At HL diagnosis for cases and reference date for controls, cases and controls were similar regarding gender, co-infection status with hepatitis viruses, HIV risk behavior, and prior AIDS events. Cases were older than controls (median age 42 years vs. 38 years; p=0.03). As expected, CD4+ cell count was higher in controls than in cases (median CD4+ cell count 422 vs. 299 cell/μL; p=0.001). On the contrary, 12 months before the reference date for controls, no difference between cases and controls in CD4+ cell count was found (median 382 cell/μL for cases vs. 359 cell/μL for controls; p=0.36). Notably, during the year preceding HL diagnosis, a statistically significant difference was found in the CD4+ cell count change. Indeed, cases lost 99 CD4+ cells/μL (95% CI, 37–161) whereas controls gained 37 CD4+ cells/μL (95% CI, 32–43) (p<0.0001).
Discussion
This is a large single-center HIV cohort study during the cART era that compares HIV-infected patients to a reference population living in the same health-district. This is of relevance since environmental and epidemiological risk factors have been one of the most important issues in HL epidemiological research. We found that the incidence of HL was close to 10 new cases per 10,000 person-years of follow-up in HIV-infected patients with or without AIDS event. Previous studies have produced conflicting data on whether HIV-HL incidence is increasing, 9,10,22 –24 which more likely reflect the differences among the cohorts (i.e., cART use, CD4+ cell count, HIV risk factors) and environmental risk factors. In the present analysis, the HIV-HL risk was approximately 20-fold higher compared with the reference population, similar to a previous Italian study considering only AIDS cases and Italian general population as reference. 15 Interestingly, HIV-HL standardized incidence was stable overtime (rates ptrend=0.29, Fig. 1). The aging of the HIV-infected population with cART may account for increasing numbers of Hodgkin lymphoma cases compared to the general population. 1 However, currently most people who live with HIV infection are between 40 and 59 years old, 25 when HL risk in the general population is relatively low, so that aging cannot fully explain the higher risk found in the HIV-infected population, compared to the general population. Indeed, in our cohort, median age of HIV-HL cases was 42 years (IQR 36–45). In this study, 11 patients treated with multi-agent chemotherapy achieved complete remission. HIV-infected patients with HL have more extensive disease with more adverse prognostic factors than the general population. However, recent studies demonstrated that HIV infection does not adversely affect overall survival when patients are treated with multi-agent chemotherapy and the prognosis for these patients may approach that of HIV-negative patients with HL. 14,26
In our analysis, baseline risk factors did not alter the risk of HIV-HL occurrence. Indeed, we did not find any association between baseline HIV viral load or CD4+ cell counts and risk of HL. The role of immunity in HIV-HL etiology is still unclear, and timing of CD4+ cell counts with respect to HL diagnosis complicates comparisons between findings. The risk of malignancies during HIV infection has been described as particular pronounced for tumor entities related to co-infections (HCV, HBV, HHV-8, HPV) which are probably particularly affected by immunodeficiency although its relationship with CD4+ cell count (i.e., nadir, baseline, time-updated CD4+ cell count, or cumulative time with a determinate CD4+ cell count) or cART is difficult to ascertain. 19,27 –29 In previous studies, the risk of HIV-HL seemed to be higher with moderate immune-suppression or a baseline CD4+ between 100–199 cells/μL and with a nadir CD4+ of 50–99 cells/μL, 2,10 supporting the hypothesis that some level of immune competence may be required for HL to develop. However, when CD4+ cell counts are considered at the HL-HIV diagnosis, the present study and other cohort studies 2,30,31 have found that the risk of HL increased substantially as the CD4+ cells declined.
Recently, data from the Collaboration of Observational HIV Epidemiological Research Europe (COHERE) cohort show as the declining CD4+ cell counts may represent an early signs of HIV-HL. 2 Indeed, in our study, the mean CD4+ cell count in HIV-HL patients fell during the year prior to HL diagnosis by 99 cells/μL (95% CI, 161–37) compared to a mean rise of 37 cells/μL (95% CI, 32–43) in controls (p<0.0001).
Here, we observed that the adjusted incidence relative risk of HIV-HL increased among cART-naïve patients and the risk of HIV-HL seems to be higher during the first 6 months after starting cART, as already reported by the French Hospital database study. 8 The influence of cART on this risk remains uncertain, with both modest elevations and no effects or reductions in risk reported. 1,6,9,30 Our data may imply that during the first 6 months of c-ART, the increases in immunity may have placed HIV-infected patients at higher risk of HIV-HL. Indeed, an essential feature of HL is the non-neoplastic milieu of reactive cells in the tumor mass, so that the neoplastic Hodgkin-Reed Sternberg (H-RS) cells need to recruit lymphocytes and histiocytes for their survival. 10 Because cART treatment has a strong influence on CD4 cell count, this higher risk could be in part explained by a causal relationship between c-ART treatment period (including cART-naïve group) and CD4+ cell counts. The majority of HIV-HL tumors have clonal infection with EBV and express high levels of a classic EBV-transforming protein, latency membrane protein 1 (LMP-1). 12 It is likely that the ability to control latent EBV infection of B lymphocytes following cART initiation may be a key element in HIV-HL pathogenesis.
Our study has several strengths. Thanks to the record-linkage procedure among three different sources, we were able to complete HIV-HL cases missing in our electronic clinic database and to compare the incidence of HL occurring in our cohort to the incidence rates extracted from the Cancer Registry of Brescia, where our center is located and where all study patients had their legal residence. In our cohort, male and female are well represented. We chose the 1999 as start year of the study in order to limit our analysis exclusively to the era cART introduced in 1996. Different from other Italian 4,15 and US 10 record-linkage studies, we considered all patients infected by HIV and not only those who developed AIDS. The principal weakness of the study was that the relative small number of HIV-HL cases still limited the possibility of stratified analysis with respect to the different antiretroviral regimens or histological subtypes of HL. Moreover, we lacked data on EBV serology.
In conclusion, our results showed that in the cART era, the risk of HL is elevated in HIV-infected patients compared to the general population and there may be some additional risk resulting from immune reconstitution during the first few months after cART initiation. Although the introduction of cART has markely improved the prognosis of patients with HIV-HL, this new analysis underscores that non-AIDS defining malignancies remain a problem, and clinicians should increase surveillance and should be sensitive to the risk factors for their development. More studies are necessary to confirm the association between an important CD4+ decline preceding the HIV-HL during effective cART. Changes in CD4+ cell counts and EBV contribution to pathogenesis of HIV-HL should be further evaluated by prospective studies.
Footnotes
Acknowledgments
The authors would like to thank all the participants and clinical staff of the the Infectious and Tropical Diseases Department.
Author Disclosure Statement
The authors declare that they have no competing interests.