
Abstract

Dear Editor,
Our urban setting clinic currently provides care to approximately 250 HIV-infected individuals. Since the clinic opened in 2008, baseline resistance testing has been performed in newly diagnosed patients, but the rates of baseline drug resistance have never been quantified. The main objective of this retrospective study was to quantify TDRM rates, 2008–2011.
Due to some data suggesting that patients in urban clinic settings may not achieve the same high levels of virologic success rates as patients in large prospective HIV clinical trials, 3 –5 the secondary objective of our study was to evaluate virologic outcomes in treatment-naïve patients after initiation of highly active antiretroviral therapy (HAART).
All treatment-naïve HIV-1-infected adults who had baseline genotype testing performed (2008–2011) were retrospectively evaluated. Analysis of the HIV pol and protease genes was performed by Virco Laboratory. Antiretroviral drug resistance was defined based on the International AIDS Society 2011 definition 6 and the CDC surveillance mutation list 2009. 7
To evaluate virologic outcomes, only patients who started HAART 2008–2010 were included, since 12-month data for the year 2011 were not available at the time of data analysis. Persistence in care was defined as availability of ≥12 months of follow up data. Virologic success was defined as HIV-1 RNA <50 copies after 12 months of therapy.
The primary objective, the prevalence of TDRMs between 2008 and 2011, was assessed using Pearson's chi-square analysis and the Fisher's exact test as appropriate. Predictors of persistence with care and the ability to achieve HIV-1 RNA <50 copies/mL were examined using logistic regression. Age, gender, ethnicity, new HIV diagnosis, baseline CD4 count, baseline HIV-1 RNA level, type of initial of HAART therapy, and baseline pharmacist counseling were entered into the regression analysis. These predictors were chosen based on previous studies, and variables we predetermined to be of interest. Descriptive statistics were also used as appropriate.
We conducted analyses using SPSS version 15.0. Tests were two-tailed with statistical significance set at a p value of less than 0.05. Wingate University's research review board approved this study.
Between 2008 and 2011, 189 treatment-naïve HIV-1-infected adults had resistance testing performed. Baseline characteristics were as follows: male, 131 (69%); mean (SD) age, 36 (11); African American, 164 (87%); Hispanic, 7 (4%); Caucasian, 15 (8%); viral subtype B, 181 (96%); median baseline CD4 count (range), 299 (1-1,299); median log10 baseline HIV-1 RNA (range), 4.6 (2.6–6.9); median number of months between HIV diagnosis and resistance testing (range), 4 (0.25–240); recent HIV diagnosis (i.e., within 12 months of resistance testing), 137 (72%); baseline counseling by a clinical pharmacist, 80 (42%).
Of the 189 patients, 19 (10.1%) had baseline resistance to ≥1 drug class. In the 137 recently diagnosed patients, baseline resistance was seen in 17 (12.4%). Baseline resistance to two drug classes was seen in only 1 patient. Year-to-year comparisons indicated a 0% TDRM rate in 2008, 12% in 2009, 8% in 2010, and 16% in 2011 (χ
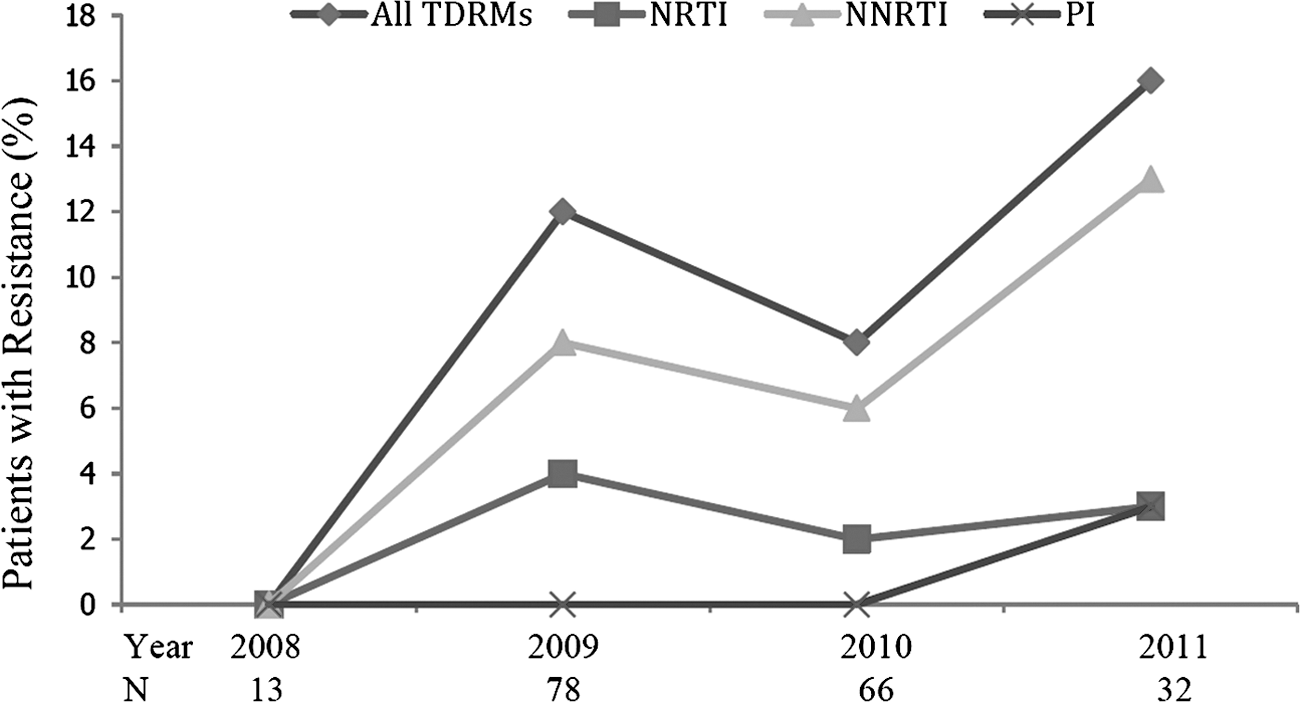
Prevalence of TDRMs, 2008–2011.
In the 19 cases with TDRMs, resistance to NNRTIs was seen in 13 (68%) patients (K103N, n=10; Y181C, n=2; V106M, n=1), resistance to NRTIs was seen in 5 (26%) patients (M41L, n=2; D67N, n=1; K219Q, n=1, M41L and L210W, n=1), and 1 (5%) patient had dual class (NNRTI and PI) at baseline (K103N and L90M).
Of the 137 patients initiated on HAART 2008–2010, 103 (75%) patients remained in care for ≥12 months and 81 (59%) achieved HIV-1 RNA level of <50 copies after 12 months of therapy. The virologic success rate is 79% (81/103) in the as-treated analysis of the 103 patients who remained in care. Recent HIV diagnosis was the only factor significantly associated with persistence with care (OR 3.53; 95% CI 1.49 to 8.36; p=0.004) and with achieving HIV-1 RNA <50 copies/mL after 12 months of therapy (OR 3.78; 95% CI 1.68–8.53; p=0.001) (Table 1).
p=0.004; b p=0.001.
This study suggests that the prevalence of TDRMs in our clinic is similar to that reported in other clinical trials performed in the United States. Recent data from the CDC National HIV Surveillance System (2006–2009) showed a 14.7% prevalence of TDRMs in patients with established infections and 19.1% prevalence in patients with recent infections. 1 The prevalence of TDRMs in recently diagnosed patients in our practice was also higher than the overall prevalence (12.4% vs. 10.1%). Importantly, the prevalence was highest in 2011 compared to 2008, 2009, and 2010, alarmingly so in the recently diagnosed patients (20%). Our limited sample size most likely resulted in a lack of a statistically significantly difference in the year-to-year comparisons.
Our retrospective evaluation showed low patient retention rate (75%) and virologic success rates (ITT, 59%; as-treated, 79%). These findings are similar to other studies performed in inner city clinics. An evaluation of retention rates in a county HIV clinic for uninsured patients found that out of 404 patients, only 53% had established care with a physician. 8 Another retrospective analysis in an urban HIV clinic found a similar virologic success rate to ours (73%). 5 Even more dismal patient retention and virologic success rates (<50%) have been described by other inner city HIV studies. 3,4
Our evaluation of baseline demographics and type of initial HAART showed that a recent HIV diagnosis was the only factor statistically associated with persistence in care and virologic suppression at 12 months. In other urban city retrospective studies, substance abuse, younger age, and nonadherence to clinic visits have been associated with failure to establish care as well as virologic failure. 4,8 Whether the choice of initial HAART regimen plays a major role is controversial, as one inner city HIV study showed that a NNRTI-based initial regimen was the only factor associated with a lower risk of treatment failure; 5 whereas another study showed that NNRTI-based initial regimens were independently associated with virologic failure. 3 Some data also suggest that adherence counseling by a HIV clinical pharmacist improves clinical outcomes in HIV-infected individuals. 9,10 The HIV clinical pharmacist at our site provided counseling to 42% of our study patients, but this was not statistically associated with persistence in care or virologic success. Several inner city HIV studies have discussed efforts that should be taken to improve patient outcomes, such as improving the quality of patient-physician relationships, 11 providing treatment for mental illness and substance abuse, 12 and focusing more on adherence counseling. 10
Although our study answered some important questions regarding our site's baseline TDRM rates and rates of virologic success, it has several limitations. It was a retrospective single-center study at an urban outpatient clinic, so our results may not be applicable to other patient populations. Our very limited sample size may have prevented us from detecting statistically significant changes in year-to-year comparisons of TDRM rates or statistical associations between demographic factors other than “recent HIV diagnosis” and clinical outcomes. Data regarding patients' illicit drug or alcohol use, adherence rates, or mental illness were not collected; these factors may have helped us to further identify reasons for dropping of out care or virologic failure. Despite these limitations, we learned that baseline resistance testing plays an important role in our clinic. Additionally, strong efforts to treat mental illness and substance abuse need to be undertaken in order to improve patient retention and virologic outcomes at our clinic.
Author Disclosure Statement
No competing financial interests exist.