
Abstract
Linkage and retention in care soon after HIV diagnosis improves clinical outcomes. Conversely, missed visits after diagnosis are associated with increased mortality in the public care setting. We analyzed mortality among newly diagnosed HIV patients ≥18 years old in a large private care setting between 01/01/1997 and 12/31/2009, comparing patients who missed visits in their first year following diagnosis (index period) with those who did not. Patients who died during the index period were excluded. Hazard ratios (HR) for association of missed visits and mortality were obtained by Cox proportional hazards regression, adjusting for patient demographics, CD4+ counts, and AIDS-defining conditions (CDC, 1993) at diagnosis. We also evaluated risk factors of missed visits by multivariable logistic regression. 2811 patients were included, of whom 65% had ≥1 missed visit, and 226 patients died during follow-up. Patients with ≥1 missed visit had a 71% increased mortality risk (HR=1.71, p=0.001) with 12% increased rate per missed visit (HR=1.12, p<0.001). Factors associated with missed visits were younger age (OR=1.69 compared to 60+ years), Black and Latino race/ethnicity (OR=1.54, 1.48 respectively, compared to Caucasians), injection drug use (OR=2.50 compared to men who have sex with men), and lower CD4+ (OR=1.43 for CD4+ 100–199 cells/μL, OR=1.39 for 50–99 cells/μL, and OR=1.63 for CD4+ <50 cells/μL, compared with CD4+ >500 cells/μL). In an insured patient population, missed visits in the first year of HIV care are common and associated with increased mortality. Early retention in HIV care is critical to improving outcomes.
Introduction
Mugavero and colleagues have shown that missing visits in the first year post-HIV diagnosis and care entry is associated with increased long-term mortality and reduced receipt of ART and other HIV-related medications and services. 6 However, this research was done at a single site with primarily an underinsured and predominantly indigent population. It is reasonable to hypothesize that there would be fewer missed visits in an insured and highly employed population with fewer economic and systems barriers to care, and possibly no association between early missed visits and subsequent mortality. Further, multiple factors related to greater odds missed visits include stigma, acceptance of diagnosis, and multiple unmet social needs. 8 9
Kaiser Permanente Northern California (KPNC) is an integrated healthcare system providing HIV care to over 20,000 insured HIV-positive patients cumulatively since the start of the epidemic, and to over 6600 patients currently. 10 We have previously shown that 89% of KPNC patients are linked to care within 90 days of HIV diagnosis, and 78% are subsequently retained in care. 11 Although these data are encouraging, the small percentage of our patients without adequate engagement in care may represent a particularly vulnerable group for adverse outcomes, including higher mortality. The objective here was to determine whether missed visits, an objective measure for engagement in care, contributes to higher mortality among an insured population, as has been reported among predominantly uninsured patients. 6
Methods
Study design
We performed a cohort analysis of HIV-positive patients at least 18 years old and newly diagnosed in KPNC between January, 1997 and December, 2007. We determined the number of missed visits for each patient during the 12 months after HIV was diagnosed (index period). We examined only those visits scheduled to take place and excluded from consideration any appointments that were cancelled (either by patient or provider) prior to the scheduled visit time, consistent with previous studies. 6 Visits were recorded as missed if the patient failed to keep the appointment and it had not been cancelled by the provider or patient. Our primary objectives were first, to determine the impact of early missed visits on subsequent mortality, and second, to identify demographic and clinical factors associated with missed visits.
Subjects
KPNC is an integrated health care system composed of 17 medical centers (inpatient and outpatient facilities) that currently provides comprehensive care including pharmacy, medical, and hospital care to over 6600 HIV-infected health plan members, who represent 17.5% of the total HIV-infected population in the counties of Northern California served by KPNC. 10 Patients in KPNC receive multidisciplinary health care, including HIV specialty care. The HIV-infected population in KPNC is demographically representative of HIV patients across California. 12 Data also indicate that KPNC members overall are very similar to the general population with regards to age, gender, and race/ethnicity, with only slight under-representation of those in lower and higher income and education categories. 13,14
KPNC maintains electronic health records (EHR), which store data on patients' demographics, diagnoses, laboratory results, hospitalizations, office visits, and prescriptions. Additionally, KPNC maintains an HIV registry of all health plan members with a confirmed HIV diagnosis as determined by manual chart review. The HIV Registry also compiles data from the EHR specific to HIV care management, including inpatient and outpatient encounters, vital status, HIV-related medications (e.g., antiretroviral medications) and laboratory results (e.g., HIV RNA levels and CD4+ cell counts). In addition, the chart review identifies other patient characteristics, including HIV risk behavior and date of initial HIV diagnosis. Like the general KPNC patient population, most HIV-infected patients (>90%) receive their medications through the KPNC pharmacy system, including medications funded through the state's AIDS Drug Assistance Program. 15
We identified all newly diagnosed HIV-infected patients in KPNC who were at least 18 years of age at time of diagnosis from January 1, 1997 through December 31, 2007. We excluded 131 patients who died within the first year after their HIV diagnosis (index period). Mortality was recorded for all patients after the index period, through December 31, 2009. To ensure complete ascertainment of vital status through the follow-up period, we captured mortality from the KPNC electronic health record, State of California death records, and from Social Security Administration datasets. Ascertainment of death using this approach enabled us to assign vital status even for patients who had left KPNC prior to 12/31/2009 and thus continue follow-up for all patients through 12/31/2009.
Measurements
We identified all outpatient visits to a KPNC physician or nurse practitioner, whether kept or missed. All primary care in KPNC is provided by physicians or nurse practitioners. Other measurements included date of birth, gender, race/ethnicity (as White, Black, Latino, Asian, or other/unknown), HIV risk (men having sex with men [MSM], injection drug use [IDU], heterosexual, or other/unknown; MSM with IDU were recorded as IDU), year of HIV diagnosis, and AIDS-defining criteria (1993 CDC criteria 16 ) at time of HIV diagnosis (yes/no). We also recorded whether the patient's care was funded through Medicare/Medicaid (yes/no), as well as the patient's CD4+ count and HIV RNA levels (first measure within 90 days of diagnosis), and whether antiretroviral therapy (ART) was initiated in the index period.
Statistical analysis
Our primary predictor variable was missed visits during the index period, which was the first year post-HIV diagnosis. Missed visits were classified four ways: (1) dichotomous (any missed: yes/no); (2) categorical (0 [reference], 1–2, 3–5, >5 missed visits); (3) continuous (count of missed visits: 0 [reference],1,2,3, etc.); and (4) percentage of all noncancelled visits (0% [reference], 1–10%, 11–25%, and >25%.) Our primary outcome was mortality after the index period, measured through December 31, 2009.
Survival was assessed after the first 365 days post-HIV diagnosis, with subjects who died in those first 365 days excluded from the analysis. The Kaplan-Meier method was used to estimate survival distributions for strata defined by number of missed visits, with differences in crude survival assessed by the log-rank test (Fig. 1). Next, adjusted hazard ratios (HR) for mortality associated with missed visits were obtained from Cox proportional hazards regression models. Cox models were fit for each of the four missed visit variables described above, with adjustment for gender, age at HIV diagnosis, race/ethnicity, HIV risk behavior, AIDS-defining criteria and CD4+ count at diagnosis, HIV RNA level at diagnosis, evidence of at least 90 days combination ART dispensed in the first year post-HIV diagnosis, Medicare and/or Medicaid (“public insurance”; compared with private insurance), and year of HIV diagnosis. Finally, we used logistic regression to determine which of the above demographic and clinical factors were associated with increased odds of having at least one missed visit during the index period, reported as adjusted odds ratios (OR). All analyses were performed with SAS (Version 9.1, Cary, North Carolina, USA), using TPHREG for Cox modeling and LOGISTIC for logistic regression analysis.
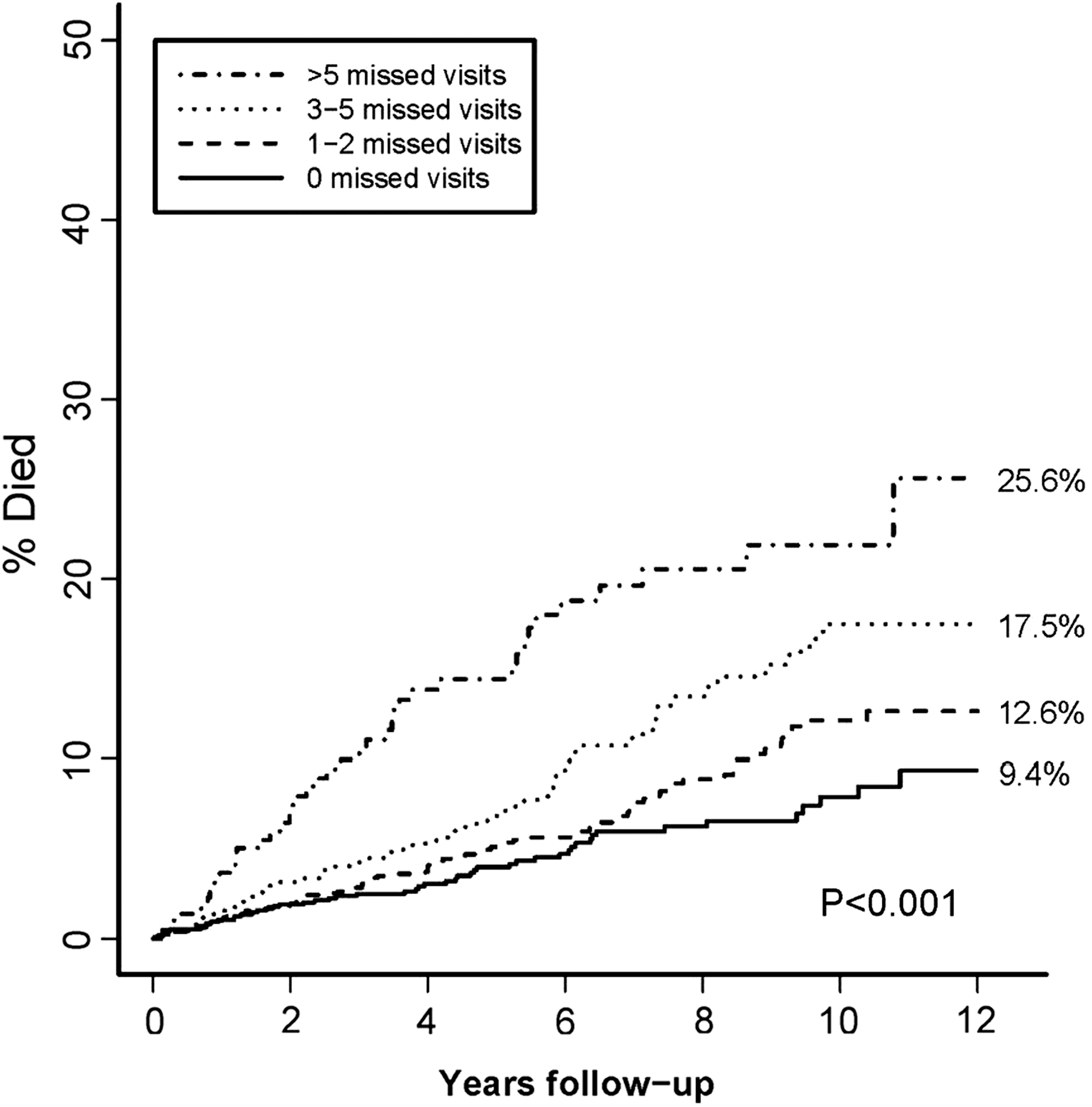
Kaplan-Meier plots show risk of death during follow-up by number of missed visits in the first year post-HIV diagnosis. P value determined by log-rank test statistic compares mortality by missed visit strata. Percentages listed on plot represent risk of death at 12 years follow-up.
We obtained approval from Kaiser Permanente Northern California Institutional Review Board, which waived the requirement for informed patient consent.
Results
A total of 2811 patients were eligible for analysis. Of those, 967 (34%) had no missed visits and 1844 (66%) had at least one missed visit during the index period (Table 1). Of the 1844 patients with at least one missed visit in the index period, 35.6% had only one missed visit, and 11.9% had over five missed visits. Those with and without missed visits were similar with respect to age and gender (Table 1). The study population was predominantly MSM, although among those with missed visits there was a lower percentage of MSM and a larger percentage of heterosexuals and IDU. A low percentage of patients had Medicare/Medicaid during the index period or had been diagnosed with AIDS-defining conditions at time of HIV diagnosis. Patients with missed visits had lower median CD4+ counts at diagnosis and higher median HIV RNA levels. A high percentage (>80%) in both groups initiated ART in the index period (not statistically different), although a statistically significant fewer percent among the no missed visit group had at least 90 days of adherence to ART in that period (p<0.001).
There were 226 deaths in the follow-up period, including 50 among those with no missed visits, 82 among those with 1–2 missed visits, 55 among those with 3–5 missed visits, and 39 among those with >5 missed visits. As shown in Fig. 1, the corresponding risk of death over 12 years was 9.4%, 12.6%, 17.5%, and 25.6% for patients with 0, 1–2, 3–5, and >5 missed visits respectively, a highly statistically significant difference across these categories (p<0.001).
Table 2 presents adjusted HRs for death for any missed visits compared with no missed visits. Any missed visit was associated with a highly significant HR of 1.71 (p=0.001), after adjustment for other risk factors. Increased risk of mortality also was associated with CD4+ counts <100 cells/μL (0–49/μL: HR=2.03, p=0.01; 50–99: HR=1.94, p=0.03). However, meeting AIDS-defining criteria at time of HIV diagnosis, HIV RNA levels at HIV diagnosis, nor ART during the first year post-HIV diagnosis were not associated with increased risk. Of note, only baseline CD4+ count <50/μL had a greater risk impact than any missed visit. Younger age (<60 years of age) was associated with decreased risk of mortality, compared with patients over 60 years old. Also, Latinos had a lower risk of mortality compared with Whites (HR=0.64; p=0.04).
All results are adjusted analyses using Cox proportional hazard regression. Covariates included in the model are as listed above.
p values reflect class variable.
Analyzing missed visits in the index period as a multilevel categorical variable (Table 3), we found increased risk of mortality if the number of missed visits was three or greater (3–5 missed visits: HR=1.86, p=0.002; >5: HR=3.56, p<0.001). A statistically significant increased risk was not seen among persons with 1–2 missed visits, although a trend for such was observed. Further, examining missed visits as the percent of total noncancelled visits, there was a corresponding increased risk of mortality, particularly if the percent of visits missed exceeded 25% (HR=2.42; p<0.001). When we analyzed the number of missed visits as a continuous variable, there was a 12% increased risk of mortality with each additional missed visit (p<0.001).
All results are adjusted analyses using Cox proportional hazard regression. Covariates included in the models: missed visit (as listed above per model), gender, age, year of HIV diagnosis, race/ethnicity, HIV risk behavior, AIDS defining condition at baseline, Medicare/Medicaid, and HIV RNA level at diagnosis, CD4+ count at diagnosis, and on antiretroviral therapy for at least 90 days in index period.
We explored which patient level factors were associated with any missed visits compared with no missed visits (Table 4). Despite being associated with decreased risk of mortality, younger age was associated with increased odds of missed visits (p=0.01). Furthermore, being Black or Latino (compared with White, OR=1.54 and 1.48, respectively) was highly associated with increased odds missed visits (p<0.001 for each). IDUs (OR=2.50; p<0.001 compared with MSM), and heterosexuals also had increased odds for missed visit (OR=1.38; p=0.01 compared with MSM). CD4+ count <200/μL was significantly associated with missed visits (OR=1.43 for CD4+ 100–199 cells/μL, OR=1.39 for 50–99 cells/μL, and OR=1.63 for CD4+ <50 cells/μL, compared with CD4+ >500 cells/μL). However, HIV RNA level or being on ART was not associated with missed visits during the index period. Of note, more recent entry into the cohort (2004–2007) was associated with decreased odds of missed visits compared with 1997–1999 (OR=0.78, p=0.02).
All results are adjusted analyses using logistic regression modeling. Covariates included in the model are as listed above.
p values reflect class variable.
Discussion
In an insured and mostly employed population of HIV-positive patients, we found that missed office visits were common in the first year post-HIV diagnosis, and were highly significantly associated with subsequent mortality. Furthermore, we found that the mortality risk increases substantially the more visits a patient misses during that first year. These results suggest that the threshold for successful engagement in care should be set to reduce or even eliminate all missed clinical visits for new patients in their first year of care. Additionally, we identified several factors associated with missed visits including younger age, Black or Latino race/ethnicity, IDUs and heterosexuals, and CD4+ count <200/μL.
The association of increased risk of mortality with missed visits in the first year of care among HIV-infected patients has been described previously in a public healthcare setting. 6 Specifically, Mugavero and colleagues from a predominantly publicly-insured HIV clinic reported an HR of 2.9 for mortality comparing those with any missed visits with those having no missed visits. This is comparable to our reported HR of 1.7 despite very different patient demographics and practice settings. Results similar to ours have been described in reports from Africa, Spain, and China, and also showed a step-wise increase in risk for mortality with increased number of missed visits. 17 –19 The fact that our results among insured patients were similar to these public healthcare settings implies that early missed visits may be a universal indicator of potentially negative outcomes. 20,21 In fact, in our data, missed visits was the strongest predictor of mortality, save for extremely low CD4+ counts.
The similarity in findings from both the public and private healthcare that missed visits are clearly associated with increased risk for mortality suggests this is related to factors other than access to care. However, compared with prior studies, our results were attenuated, albeit highly statistically significant. Our lower hazard ratio estimates could be due to KPNC offering equal access to care to all KPNC members. Our integrated care environment and case management approach might also explain our lower mortality risk estimates. The presence or absence of integrated care might differentially impact care access in other settings. 11,22 Alternatively, other factors among KPNC patients might lower their risk of mortality despite missing some visits. For example, homelessness is associated with decreased access to medical care, but is not a significant issue among our patients. 23
Patients in the latter time period (2004–2007) were less likely to miss appointments. Possible explanations for this phenomenon is that clinics in our system may have started paying more attention to patients who failed to keep appointments and prescribed closer follow-up and offered more convenient appointment times. More effective and better tolerated ART regimens being used in the latter time periods could be associated with greater adherence to both medications and clinical visit adherence. 24 Also, over time, there has evolved greater experience of providers and higher patient satisfaction, as evidenced by public survey results, 25,26 both of which can lead to greater appointment adherence.
Our finding that certain populations have increased risk of missed visits is important. Like previous studies, we found younger age and Black race associated with increased missed visits. 6,27 –30 However, we also found that IDU was independently associated with missed visits, as seen in other studies. 27,28 Furthermore, we found that lower CD4+ count was associated with increased likelihood of missed visits; this finding is in contrast to other studies. 6,20 This phenomenon is likely due to patients with more advanced disease (as evidenced by lower CD4+ counts), associated with greater fragility and often less mobility, are less able to get to clinic appointments. 31 These patient-specific differences in risk of missed visits and risk of mortality should help clinical programs target specific populations for more intensive retention in care efforts. Patients with lower CD4+ counts may need additional efforts to ensure they keep their appointments, and failure to keep appointments should be closely monitored. Younger patients are more likely to miss appointments, and efforts to retain these patients in care are critical. Prior studies have shown that decreasing stigma, improving acceptance of the HIV diagnosis, and other unmet social needs will improve visit adherence. 8,9 Additionally, outreach to IDU HIV-infected patients is a priority, as they have increased risk of missed appointments and an increased risk of mortality.
An important next step is to determine why missed visits are an important marker for mortality. Missed visits are lost opportunities for services including immunizations, preventive health screenings, review of medications for tolerance and adherence issues, mental health check-ups, and screening for drug and alcohol abuse. 4 Prior studies from our institution have indicated that these services are provided to our general population at most visits, so it is likely they are also received by our HIV-infected patients, when and if they keep their appointments. 11 We did not find a significant difference in risk of mortality with ART initiation between those had no and any missed visits, so it does not appear that missed visits represent failure to start ART in a timely fashion. Lower CD4+ count (<100/μL) was associated with increased mortality, but having a prior AIDS-defining event or a higher HIV RNA level was not. Missed visits could indicate a lower level of attention and concern about one's own care, and be a proxy for lower ART adherence, greater levels of depression or mental illness, and other co-morbidities not evaluated here.
Strengths of our study include a comprehensive EHR able to determine kept or missed visits over time, our large sample size compared to prior studies, 6,32 multiple approaches to categorize and evaluate missed visits, and the comprehensive ascertainment of death. Consistency of findings across approaches to categorizing missed visits adds credence to the validity of our findings.
There are some limitations to our study. We did not measure other co-morbidities that could be associated with greater likelihood of missed visits and greater risk of mortality. However, to the extent that co-morbidities provide an impetus to avoid missed visits, they would not diminish the association between missed visits and increased mortality found here. There is also the possibility of reduced generalizability of study findings from an integrated care system to other healthcare models. However, it is notable that our findings were highly consistent with a prior study in a public health setting. Finally, we did not evaluate other factors, such as limited access to transportation, which has been previously reported to be associated with lower retention in care and greater mortality. 33 These limitations should not take away from the principal finding here of increased risk of mortality with missed visits.
In conclusion, we demonstrated that even in the private healthcare setting, where there should be improved and more consistent access to healthcare and services for all patients, missed medical visits are associated with increased risk of death among HIV-infected patients. We found a 69% increased risk overall with any missed visit and a 12% increased risk with each missed visit. In fact, missed visits were a greater risk factor for mortality than nearly all other factors evaluated. Given the call for lower mortality among HIV-infected Americans in the United States' National HIV/AIDS Strategy, 34 greater attention to patients who miss appointments is critical. In response to studies like ours which show the significance of missed visits in the care of HIV-infected patients, the National Quality Forum is expected to endorse a new HIV quality of care measure: did the patient have an HIV-related medical appointment in the last six months of the measurement year. 35 While not perfect, this metric would provide additional impetus to healthcare providers in all sectors to increase their focus on retention in medical care for their HIV-infected patients. Patients who miss visits early in the care process need to be identified as soon as possible and then intensive efforts should be initiated to lower their risk of mortality. 36
Footnotes
Acknowledgments
The authors wish to thank Courtney Ellis for her assistance with manuscript preparation. This work was supported by Kaiser Permanente Northern California Community Benefits Research Fund, and internal Kaiser Permanente funding mechanism. MJS was supported by grant number K01AI071725 from the NIAID of NIH.
Author Disclosure Statement
The authors have no further disclosures relevant to this article.