
Abstract
We conducted a single-center prospective study to evaluate the utility of cytomegalovirus (CMV) antigenemia assay for the diagnosis of CMV-gastrointestinal disease (GID). The study subjects were HIV-infected patients with CD4 count ≤200 μL/cells who had undergone endoscopy. A definite diagnosis of CMV-GID was made by histological examination of endoscopic biopsied specimen. CMV antigenemia assay (C10/C11 monoclonal antibodies), CD4 count, HIV viral load, history of HAART, and gastrointestinal symptoms as measured by 7-point Likert scale, were assessed on the same day of endoscopy. One hundred cases were selected for analysis, which were derived from 110 cases assessed as at high-risk for CMV-GID after endoscopy screening of 423 patients. Twelve patients were diagnosed with CMV-GID. Among the gastrointestinal symptoms, mean bloody stool score was significantly higher in patients with CMV-GID than in those without (2.5 vs. 1.7, p=0.02). The area under the receiver-operating characteristic curve of antigenemia was 0.80 (95%CI 0.64–0.96). The sensitivity, specificity, positive likelihood ratio (LR), and negative LR of antigenemia were 75.0%, 79.5%, 3.7, and 0.31, respectively, when the cutoff value for antigenemia was ≥1 positive cell per 300,000 granulocytes, and 50%, 92.0%, 5.5, and 0.55, respectively, for ≥5 positive cells per 300,000 granulocytes. In conclusion, CMV antigenemia seems a useful diagnostic test for CMV-GID in patients with HIV infection. The use of ≥5 positive cells per 300,000 granulocytes as a cutoff value was associated with high specificity and high positive LR. Thus, a positive antigenemia assay with positive endoscopic findings should allow the diagnosis of CMV-GID without biopsy.
Introduction
The CMV blood antigenemia assay is a noninvasive method to detect CMV viremia and its utility has been evaluated previously for the diagnosis of CMV end-organ diseases in patients with HIV infection. 7 –10 However, many of those studies included various types of CMV end-organ diseases such as CMV retinitis and pneumonia. To our knowledge, there are no studies that have investigated the value of CMV antigenemia assay in the diagnosis of CMV-GID, especially in HIV-infected patients.
We conducted a prospective study to assess the utility of the CMV antigenemia assay for the diagnosis of CMV-GID in patients with HIV infection.
Methods
Subjects
We prospectively recruited 423 HIV-infected patients who had undergone endoscopy between 2009 and 2012 at the National Center for Global Health and Medicine (NCGM), a 900-bed hospital located in the Tokyo metropolitan area and the largest referral center for HIV/AIDS in Japan. These patients were generally referred for endoscopy by the attending physician, based on the presence of gastrointestinal symptoms or for asymptomatic screening. Patients with CD4 count ≤200 were included in the analysis. We excluded patients who had received endoscopy for follow-up evaluation less than 3 months after treatment of gastrointestinal disease, who were under treatment for other CMV end-organ diseases, and those who were free of antigenemia.
The institutional review board of our hospital approved this study (approval No. 715).
Clinical factors
Gastrointestinal (GI) symptoms, CD4 count, HIV-RNA, history of HAART, and sexual behavior were collected before endoscopy. To evaluate GI symptoms, the modified gastrointestinal symptom rating scale (GSRS) rating on a 7-graded Likert scale was used. 11,12 The modified GSRS consists of the original GSRS (abdominal pain, heart burn, acid regurgitation, sucking sensation in the epigastrium, nausea and vomiting, borborygmi, abdominal distention, eructation, increased flatus, decreased passage of stools, loose stools, hard stools, urgent need for defecation, feeling of incomplete evacuation), plus odynophagia, chronic diarrhea, and bloody stool. Chronic diarrhea was defined as an episode lasting longer than 4 weeks.
Antigenemia assay
Antigenemia assay using C10/C11 monoclonal antibodies (Mitsubishi Chemical Medience, Tokyo, Japan) was performed as described previously. 13 –15 A positive result of the CMV antigenemia assay was defined as ≥1 CMV-positive cell per 300,000 granulocytes applied. The assay was performed on the same day of endoscopy. For patients who were empirically prescribed anti-CMV therapy before endoscopy, CMV antigenemia obtained before initiating the therapy was used for analysis.
Diagnosis of CMV-GID
CMV-GID was suspected based on endoscopic findings, such as patchy erythema, edematous mucosa, multiple erosions, and ulcers. 16,17 Biopsy was performed when such endoscopic findings were encountered. CMV-GID was defined as the detection of large cells with intranuclear inclusions, alone, or in association with granular cytoplasmic inclusions on histological examination of biopsy specimens. 1 Biopsy sections were stained with hematoxylin and eosin, and also immunohistochemically stained with anti-CMV. The results were considered positive when the above-mentioned cells showed marked brown coloration in both nuclei and cytoplasm.
Statistical analysis
We divided patients into two groups based on the presence or absence of CMV-GID. Patient characteristics and clinical findings were then compared in the two groups using the Mann-Whitney U test, χ2test, and Fisher's exact test for quantitative and qualitative variables, respectively. Area under the receiver-operating characteristic curve (ROC-AUC) analysis was used to quantify the accuracy of CMV antigenemia assay. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), positive likelihood ratio (LR), negative LR, and diagnostic odds ratio for the diagnosis of CMV-GID were also calculated for different cutoff values (≥1 positive cells per 300,000 granulocytes and ≥5 positive cells per 300,000 granulocytes). In a subgroup analysis stratified by patients with and without history of HAART, the sensitivity, specificity, PPV, and NPV were calculated using the cutoff value of CMV-positive cells of ≥1 per 300,000 granulocytes. All statistical analyses were performed using Stata software (version 10, Stata Co., USA).
Results
A total of 100 patients were selected for analysis after the application of the aforementioned exclusion criteria (Fig. 1). The majority of patients were males, and the median age was 40. The median CD4 count was 84 [interquartile range (IQR) 33.3–148.8] and 58.0% of the patients had history of HAART. Twelve patients were diagnosed with CMV-GID based on the abovementioned criteria (Fig. 2). In these patients, the median CMV antigenemia value was 4 positive cells per 300,000 granulocytes (range, 0–786). CMV-GID was localized to the upper GI tract in one patient, in the lower GI tract in 11, and in both parts in two.
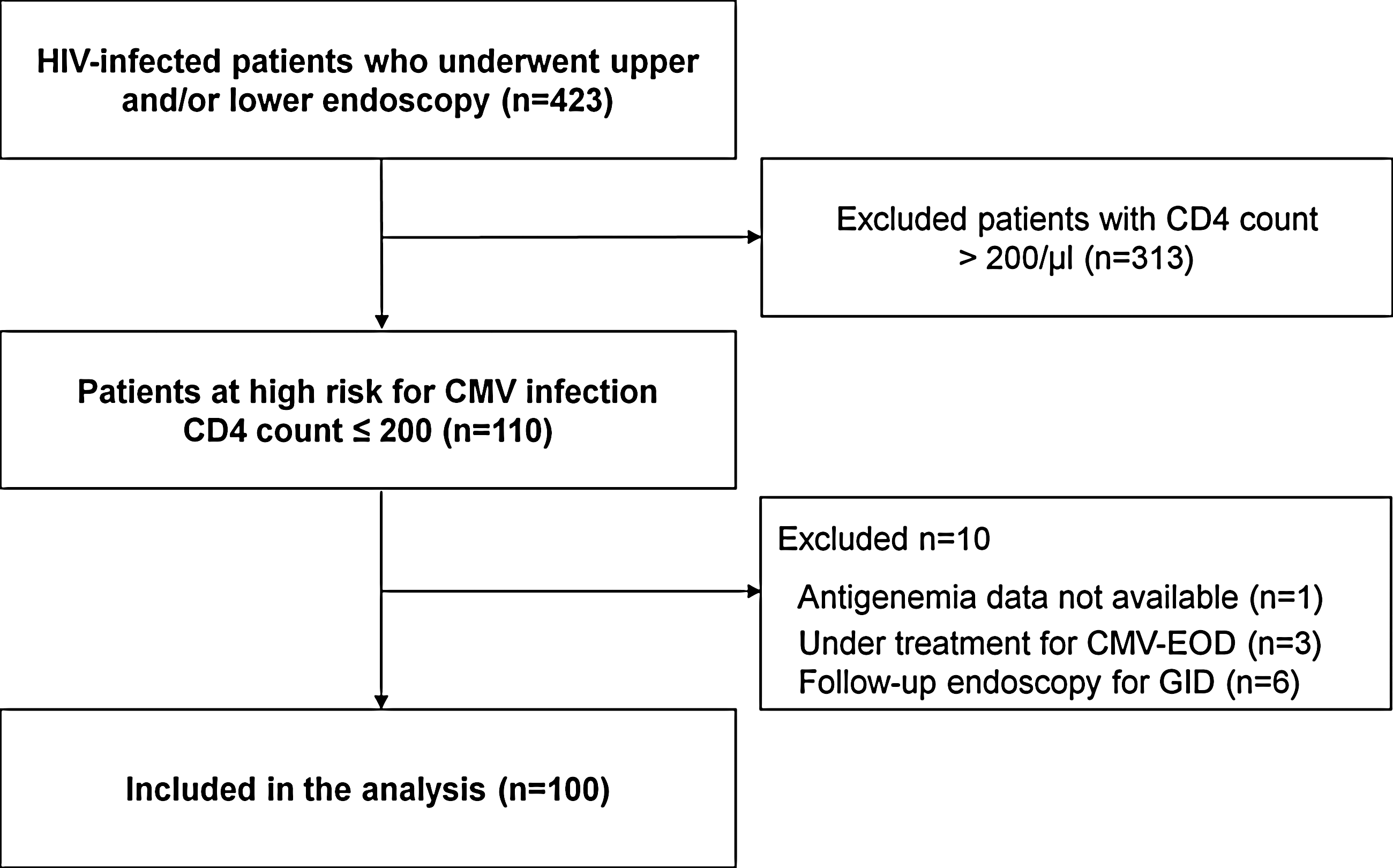
Flow diagram of patient selection. CMV, cytomegalovirus; EOD, end-organ disease; GID, gastrointestinal disease.
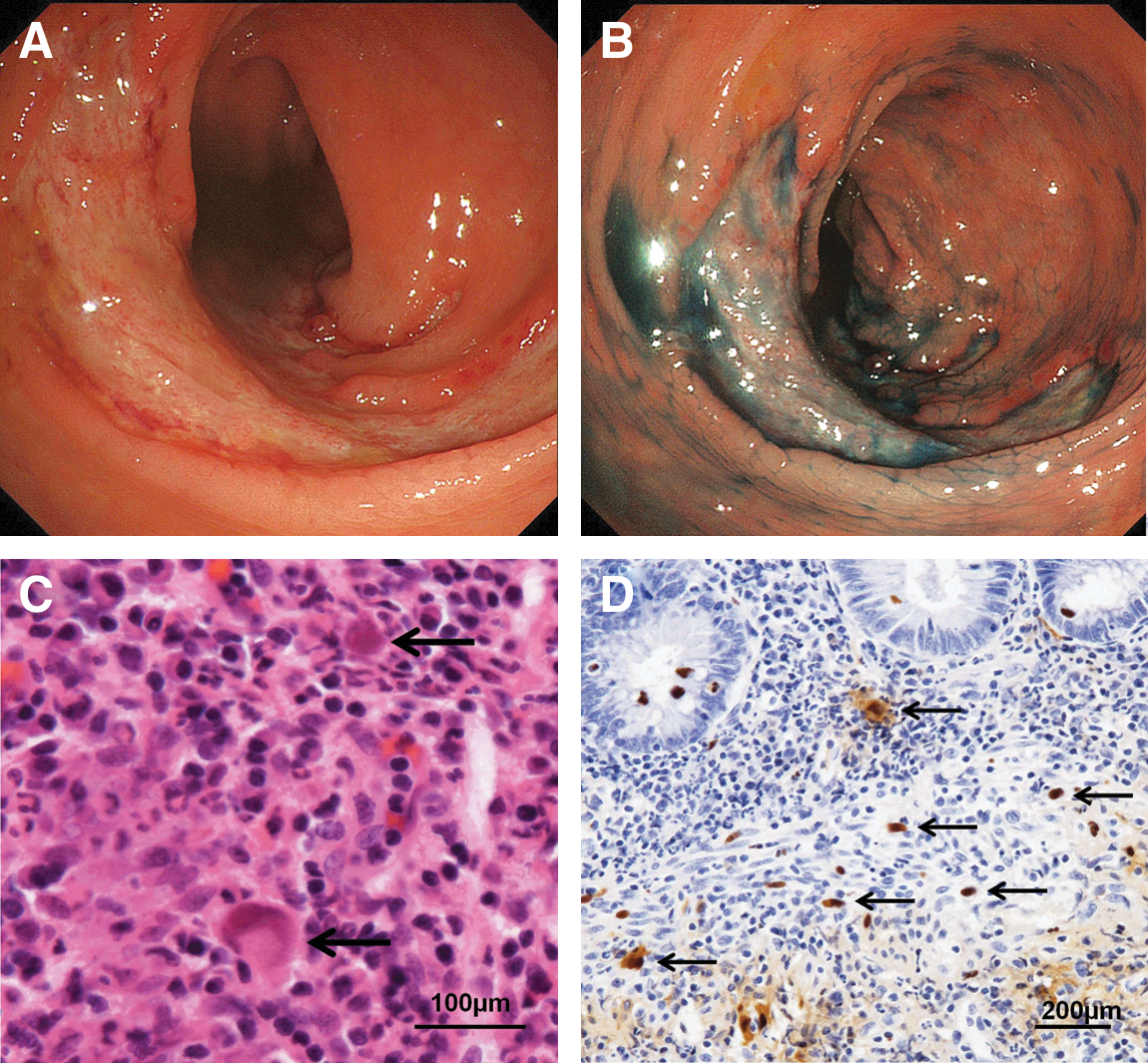
Endoscopic and pathological features in representative cases.
Table 1 shows the baseline and demographic characteristics of the participating patients. Univariate analysis showed that significantly fewer patients with CMV-GID had history of HAART than those without CMV-GID (p=0.016) and median CD4 count was not significantly different between the two groups (p=0.356). The number of patients with positive CMV antigenemia was significantly higher in those with CMV-GID than those without (p<0.01). The mean bloody stool scores was significantly higher in patients with CMV-GID than in those without CMV-GID (p=0.021). In addition, there was a trend toward higher scores for heartburn (p=0.064) and chronic diarrhea (p=0.078) in patients with CMV-GID. The proportions of patients with the other symptoms were not different between the two groups.
CD4 cell counts within 1 week and HIV-RNA viral load within 1 month were checked at the day of endoscopy. A positive result for real-time HIV RNA was defined as ≥40 copies/mL. History of HAART was collected from the medical records prior to endoscopy. Sexual behavior was defined as men who have sex with men (MSM) or heterosexual.
CMV, cytomegalovirus; GID, gastrointestinal disease; HAART, highly active antiretroviral therapy; IQR, interquartile range; MSM, men who have sex with men; SD, standard deviation.
ROC-AUC of the CMV antigenemia assay was 0.80 (95%CI 0.64–0.96). Table 2 lists the data that describe the diagnostic accuracy of CMV antigenemia assay. Using a cutoff value of ≥1 positive cell per 300,000 granulocytes for positive CMV antigenemia assay, the sensitivity, specificity, positive LR, and negative LR of antigenemia for CMV-GID were 75.0%, 79.5%, 3.7, and 0.31, respectively. The use of a cutoff value of ≥5 positive cells per 300,000 granulocytes yielded 50.0% sensitivity, 90.9% specificity, a positive LR of 5.5, and negative LR of 0.55 for the diagnosis of CMV-GID. Subgroup analysis showed a sensitivity of 66.7% and specificity of 83.6% for the assay for patients with history of HAART, while higher sensitivity (77.8%) and lower specificity (72.7%) were noted for those without ART.
Cutoff value of ≥1 positive cell per 300,000 granulocytes was used in the analysis.
CMV, cytomegalovirus; HAART, highly active antiretroviral therapy; LR+, positive likelihood ratio; LR−, negative likelihood ratio; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value.
Discussion
The present study provides the first prospective analysis of the CMV antigenemia assay in the diagnosis of CMV-GID in HIV-infected patients with 75.0% sensitivity and 79.5% specificity. The antigenemia assay is one of the most widely used methods for detecting reactivation of CMV infection, but only a few studies have examined its diagnostic value for CMV-GID, 18 –21 and all were retrospective in design. Jang et al. 20 recently reported that the sensitivity and specificity of the CMV antigenemia assay for the diagnosis of CMV-GID were 54% and 88%, respectively, in patients with secondary immunodeficiency disease. Nagata et al. 21 also reported 65.4% sensitivity and 93.6% specificity of the CMV antigenemia assay for CMV-GID in patients with positive endoscopic findings. The present study demonstrated higher sensitivity (75.0%) and lower specificity (79.5%) than those studies. This difference in accuracy could be explained by the difference in the study population since only HIV-infected patients were included in our study, whereas previous studies included a substantial number of patients with immune deficiency due to etiologies other than HIV infection.
The sensitivity of antigenemia assay for the diagnosis of CMV end-organ disease in HIV-infected patients reported in previous studies was generally higher than that in the present study. 8 –10,22 –26 This difference could be explained by the fact that the current study focused on gastrointestinal disease, while previous studies included various CMV diseases such as retinitis, cholangitis, pneumonia, and encephalitis. 8 –10,22 –26 The diagnostic accuracy of CMV antigenemia may vary depending on the site and extent of organ/tissue involvement.
Identification of CMV cells in tissue samples obtained by endoscopic biopsy is considered the gold standard for the diagnosis of CMV-GID. 1,2,6 The endoscopic findings in CMV-GID include ulcer and mucosal inflammation; 16,17 however, physicians may not consider it necessary to take a biopsy in patients with only mucosal inflammation without ulceration. Even in cases of severe deep or bleeding ulcers, some physicians may hesitate to perform a biopsy. In such cases, no definite diagnosis of CMV-GID can be made. Our results suggest that the CMV antigenemia assay is to some extent useful for the diagnosis of CMV-GID in patients with endoscopic findings, especially when CMV positive cell counts are high. Considering the high specificity and high positive LR (5.5) of the positive CMV cell count ≥5, the use of this method before endoscopy could potentially avoid complications due to biopsy.
One limitation of this study was the single-center nature of the investigation. Significant differences in independent factors were not detected in the present study probably due to the small number of patients with CMV-GID. For example, we used gastrointestinal symptoms with score of 7 points on the Likert scale, but the differences in most symptoms between patients with or without CMV-GID did not reach statistical significance due to the small number of cases. Further studies based on larger population are needed. Another limitation is a selection bias related to the selection criteria applied in the present study: only patients who underwent endoscopy for such reasons as symptoms and screening were included in the study.
In conclusion, the CMV antigenemia assay showed relatively good sensitivity and specificity for the diagnosis of CMV-GID in patients with HIV infection. Furthermore, specificity and positive LR improved when the cutoff value of CMV cell count was increased from 1 to ≥5 positive cells per 300,000 granulocytes. Considering the high specificity of the test, the use of this method before endoscopy could potentially avoid complications due to biopsy.
Footnotes
Acknowledgments
We are grateful to Hisae Kawashiro (Clinical Research Coordinator) for help with data collection. The authors thank all other clinical staff at the AIDS Clinical Center and all the staff of the endoscopy unit.
This work was supported by Grants-in Aid for AIDS research from the Japanese Ministry of Health, Labor, and Welfare (H23-AIDS-001), and the Global Center of Excellence Program (Global Education and Research Center Aiming at the Control of AIDS) from the Japanese Ministry of Education, Science, Sports and Culture.
Author Disclosure Statement
The other authors declare no conflict of interest.