
Abstract
Antiretroviral medications can be taken by HIV-negative persons to prevent HIV infection, also known as pre-exposure prophylaxis (PrEP). PrEP was first shown to be effective during the iPrEX study. We conducted a survey involving HIV healthcare providers to document their attitudes and prescribing practices about PrEP in response to this study. An online survey was completed by 189 members and credentialees of the American Academy of HIV Medicine between April 2011 and September 2011. Ninety percent of respondents were familiar with the results of the iPrEx study, and most (78%) were familiar with CDC's interim guidance regarding the use of PrEP in MSM. Only 19% of respondents had prescribed PrEP. The majority of PrEP prescribers were compliant with CDC interim guidance; however, only 61% screened for hepatitis B. Of PrEP prescribers, 78% prescribed to MSM, 31% to MSW, and 28% to WSM. Greatest concerns about prescribing PrEP included development of antiretroviral resistance (32%), potential increase in high-risk behavior, (22%) and poor medication adherence (21%). Fifty-eight percent stated that HIV serodiscordance within a relationship most influenced their decision to prescribe PrEP to the HIV-seronegative partner. This study demonstrates that, despite awareness of the efficacy of PrEP, its use is limited. Survey participants used PrEP most commonly in MSM; however, a significant percentage also prescribed PrEP to women. The best candidate for PrEP is felt to be individuals in an HIV-serodiscordant relationship. Limitations to our study included a low response rate, changes in the evidence base, and the novelty of PrEP.
Introduction
H
PrEP has been shown to be both safe and effective in both oral and topical formulations in several studies. 4 –7 The iPrEx study was a multinational, randomized, placebo-controlled trial of daily oral tenofovir disoproxil fumarate-emtricitabine (FTC/TDF) in HIV-seronegative men who have sex with men (MSM) and transgender women. The study demonstrated that FTC/TDF reduced HIV acquisition risk by 44%. Subgroup analyses showed even higher efficacy (73%) in those patients with ≥90% adherence. 4 Following publication of the iPrEx study results, the CDC issued interim guidance for use of PrEP for HIV prevention in MSM. This was done to prevent unsafe practices, such as using unproven antiretrovirals, using alternate dosing schedules, or not screening for acute HIV infection before beginning PrEP. 8 Subsequent to this study, FTC/TDF was approved by the FDA for use in HIV prevention in July 2012. 9 Also since the publication of the iPrEx study, other trials have demonstrated that PrEP can be effective if high-level medication adherence is maintained. The Partners PrEP study demonstrated that both oral TDF and FTC/TDF prevent HIV acquisition in the HIV negative heterosexual partner. 5 The TDF2 study group further demonstrated that daily FTC/TDF prophylaxis prevented HIV infection in heterosexually active but not partnered men and women. 6 In contrast to these studies, the FEM-PrEP study, which evaluated daily FTC/TDF in African women to prevent HIV, did not demonstrate a reduction in the rate of new HIV acquisition. However, drug adherence was low. 10 The VOICE trial demonstrated that PrEP in the form of a vaginal gel or an oral tablet did not prevent HIV infection in young, mostly single African women. Again, poor medication adherence was found to be the probable cause. 11 Myers and Mayer have summarized the status of current research in PrEP for HIV prevention in a recent review. 12
Little is known about the knowledge base, perceptions, attitudes, or prescribing practices of healthcare providers in the United States surrounding PrEP. One study, conducted at the University of California-San Francisco (UCSF), reported on interviews with medical care providers to ascertain their views on implementing PrEP. These providers included primary care physicians, HIV specialists, community health clinic providers, and public health officials. A majority of the participants expressed optimism regarding their use of PrEP in their practices. However, there was little consensus on the optimal target population for PrEP, and there were concerns about monitoring patients appropriately and ensuring adherence. 13
In order to further examine these issues, we conducted a nationwide survey of HIV healthcare providers in the United States, to evaluate their knowledge, attitudes, perceptions, and prescribing practices regarding PrEP.
Methods
The study was conducted using an online survey from April 2011 to September 2011. The survey was sent to members of the American Academy of HIV Medicine (AAHIVM), HIV specialists credentialed by the AAHIVM, and other HIV healthcare providers. Approximately 1800 surveys were distributed. No personal identifying information was collected with the survey. It was distributed via a professional mailing list server using the Survey Monkey platform (SurveyMonkey.com, 285 Hamilton Avenue Palo Alto, CA 94301, United States). The survey consisted of 21 multiple choice, true-false, and short answer questions, and took approximately 10–12 min to complete. There were no time constraints given, and respondents were free to complete the survey at their leisure. Participants were asked about their knowledge, attitudes, perceptions, and concerns about PrEP, as well as their prescribing practices of PrEP. This survey was conducted after the iPrEx study was published in the New England Journal of Medicine in November 2010. 4 Following this, in January 2011 the CDC issued interim guidance regarding the use of PrEP in MSM. 8 During the time of this survey, Family Health International (FHI) released a news bulletin on April 18, 2011, announcing the lack of efficacy of PrEP in women and closure of accrual to the FEM-PrEP study. 14 The results of the Partners PrEP trial and TDF2 study demonstrating the safety and efficacy of PrEP in preventing heterosexual HIV transmission, were presented at the International AIDS Society (IAS) conference in July 2011, but had not yet been published in a peer-reviewed journal at the time of the survey. 15
Results
Demographics
One-hundred eighty-nine HIV practitioners responded to the survey. Of 189 participants, 56% (N=105) were male, and 44% were female (N=84). Forty-seven percent (N=83) were>50 years old. Eighty-five percent of participants (N=161) cared for>20 HIV+ patients monthly.
Knowledge about PrEP and prescribing practices
The great majority of survey respondents were familiar with the results of iPrEx study (90%, N=133) and the CDC's interim guidance regarding the use of PrEP in MSM (78%, N=147). Although 43% (N=82) had patients who requested PrEP, only 19% (N=36) prescribed it. Of these, 83% (N=30) prescribed FTC/TDF, and 17% (N=6) prescribed a “triple-drug HIV regimen.” Only 3% (N=6) provided PrEP on more than five occasions. Seventy-eight percent (N=28) prescribed PrEP to MSM, 31% (N=11) to heterosexual males, and 28% (N=10) to heterosexual women.
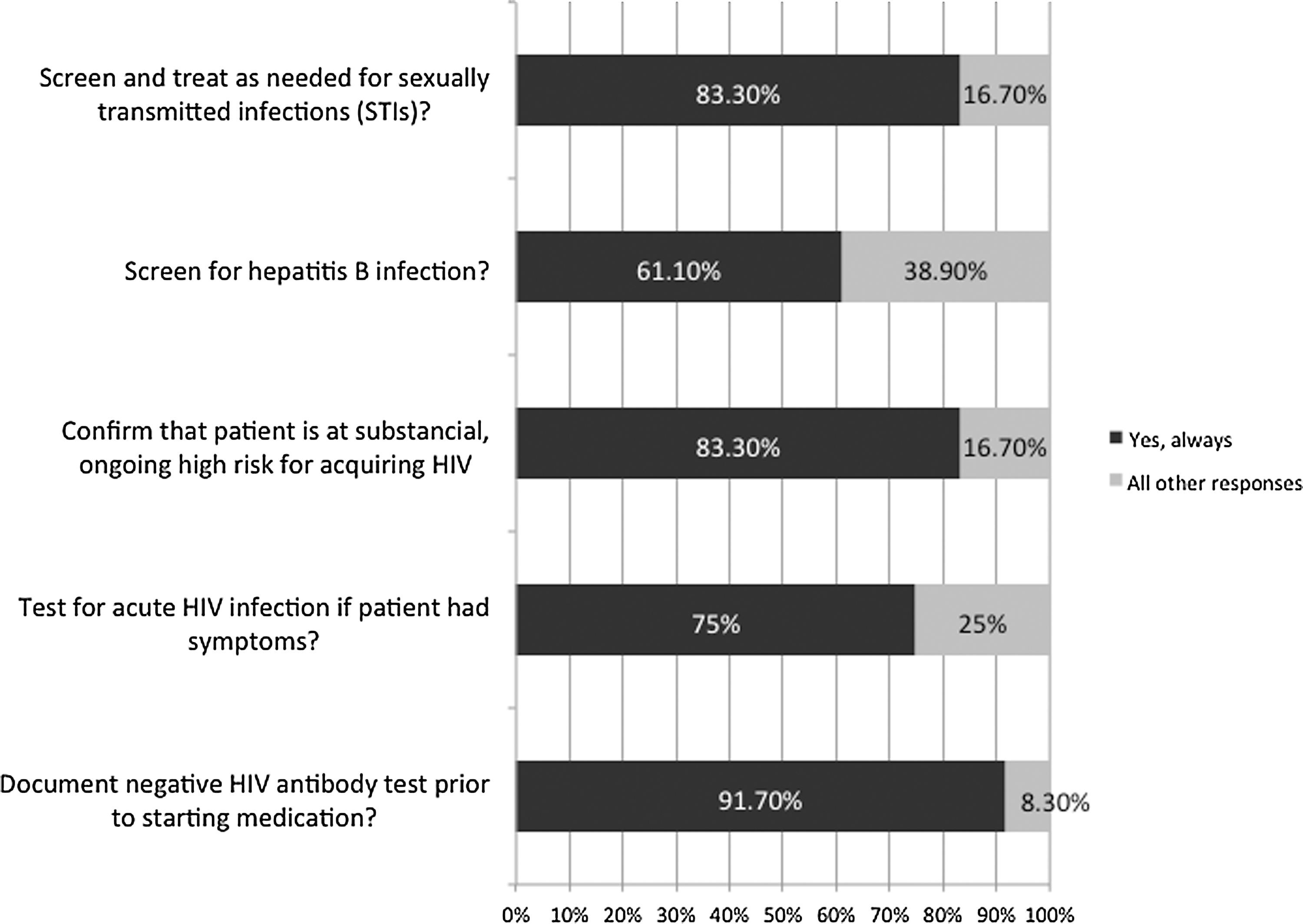
We asked providers if they had acted in accordance with the CDC's interim guidance recommendations in providing PrEP to their patients (Fig. 1). Ninety-one percent documented a negative anti-HIV antibody test prior to starting PrEP, and 75% tested their patient for acute HIV infection if the patient had signs or symptoms of the acute retroviral syndrome. Eighty-three percent confirmed the patient was at high-risk of developing HIV infection, and 83% screened and treated patients for sexually transmitted infections. However, only 61% percent of respondents indicated that they had screened for hepatitis B (HBV) infection prior to prescribing PrEP.
For the 36 respondents who had provided PrEP in the past, we questioned if they performed CDC interim guidance recommendations.
When PrEP was discontinued, 25% (N=9) stated this was secondary to patient preference, 25% (N=9) indicated patients were no longer at high-risk for HIV infection, 14% (N=5) cited medication non-adherence, and 22% (N=8) reported high cost of medication as the reason for discontinuing PrEP.
Attitudes towards PrEP
When assessing a patient's risk factors for acquiring HIV as a stimulus to prescribe PrEP, 58% of respondents (N=109) stated that a patient having an HIV-positive partner would most influence their decision to prescribe PrEP. Having multiple sexual partners was the next highest risk factor influencing PrEP prescription (29%, N=54), followed by failure to use condoms (26%, N=49), and lastly followed by a patient with a history of sexually transmitted infections (23%, N=44) (Fig. 2). The most commonly voiced concerns about prescribing PrEP included the development of antiretroviral resistance (32%, N=61), a potential increase in high-risk behavior (22%, N=42), patient nonadherence with medication (21%, N=40), and high cost of the drugs (12%, N=22) (Fig. 3). Sixty-two percent of respondents (N=118) stated that potential adverse effects of antiretrovirals would influence their decision to prescribe PrEP to an otherwise healthy individual. Only 13% of respondents felt that PrEP was the “most effective” method for reducing HIV acquisition, while 47% felt that expanding HIV testing would be the most effective method (Fig. 4).
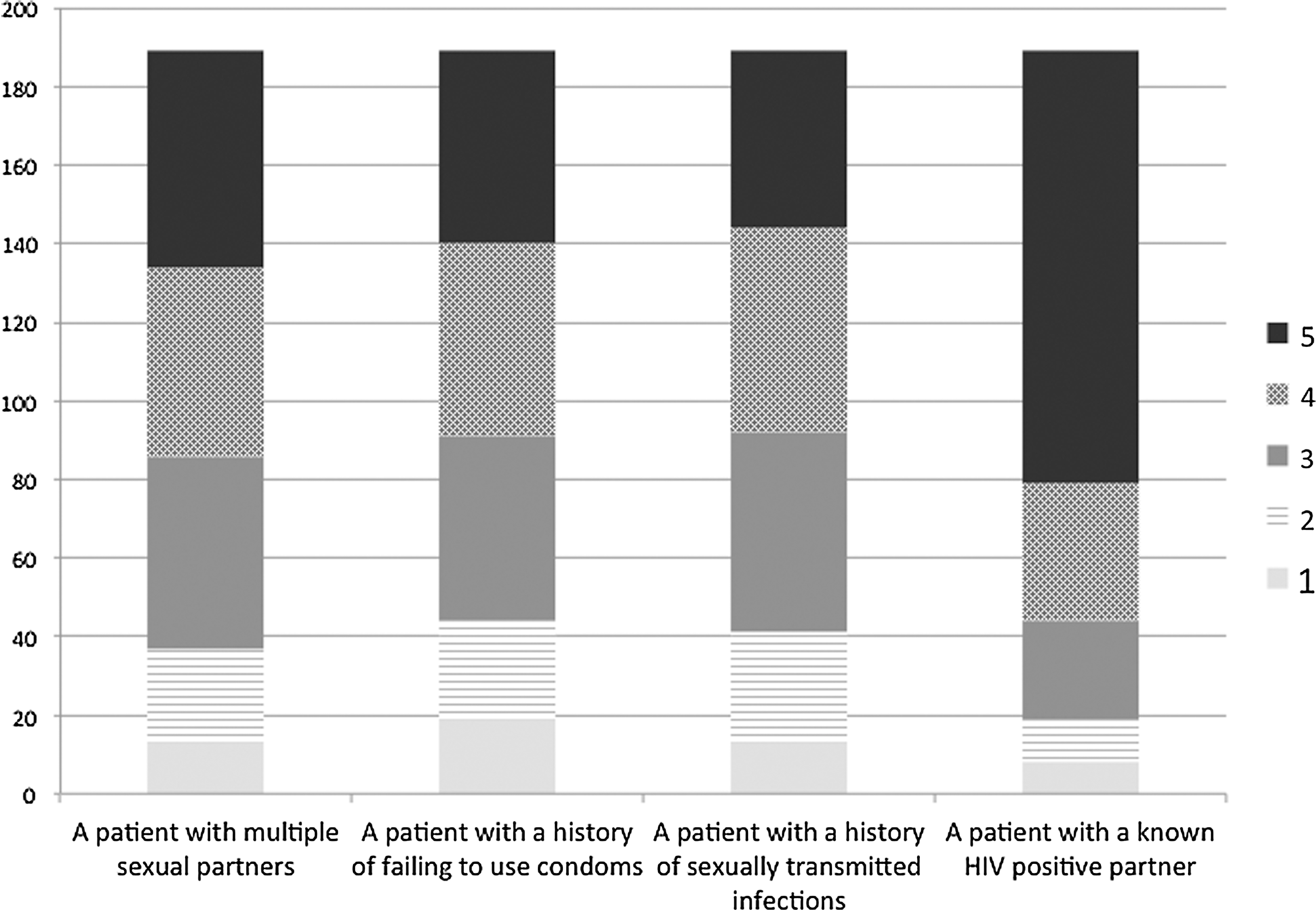
Summary of responses to PrEP survey question: “How would the following factors influence your decision to prescribe PrEP (1-least likely to prescribe, 5-most likely to prescribe)?”
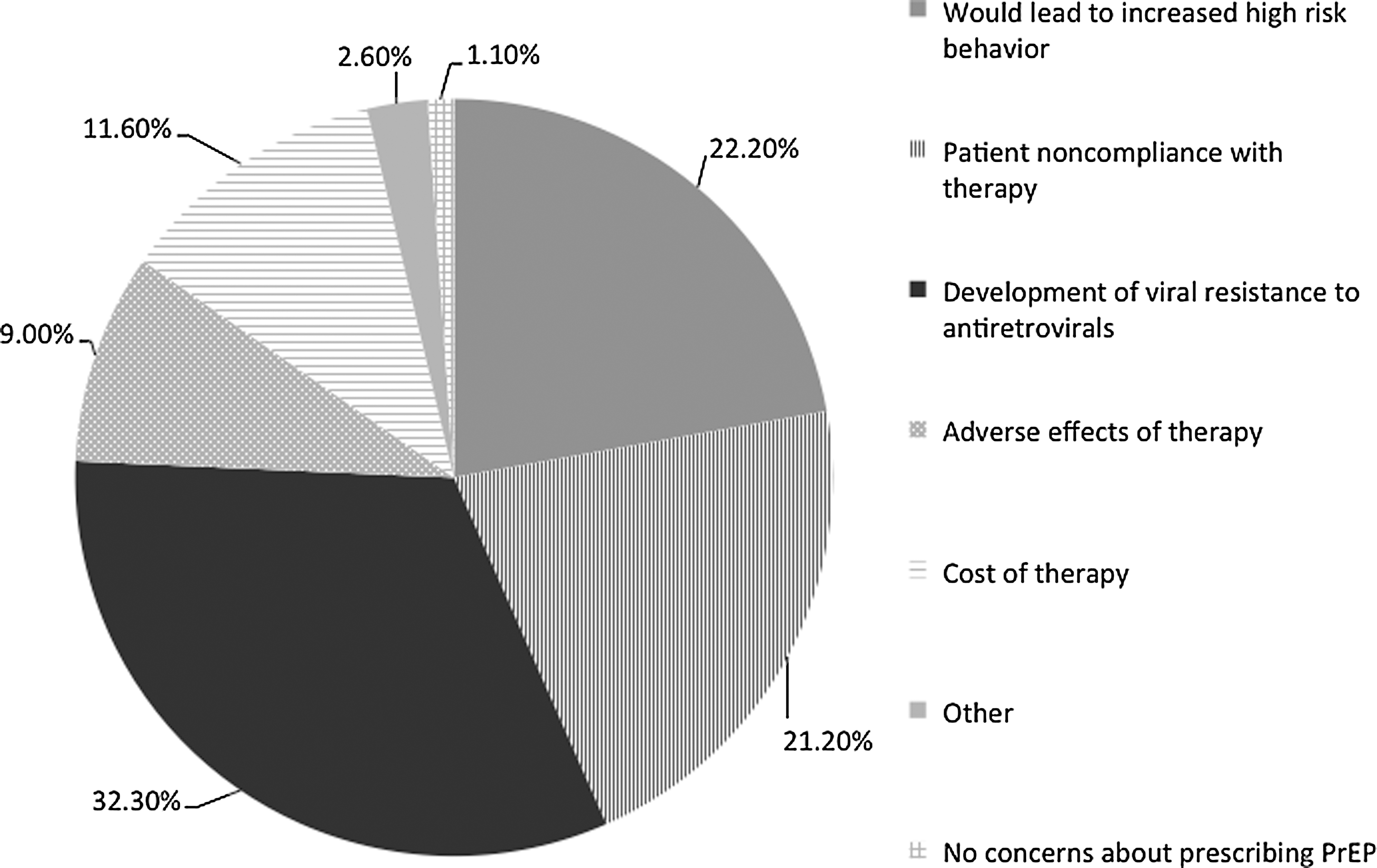
Chart summarizing responses to PrEP survey question: “What is your greatest concern about prescribing PrEP?”
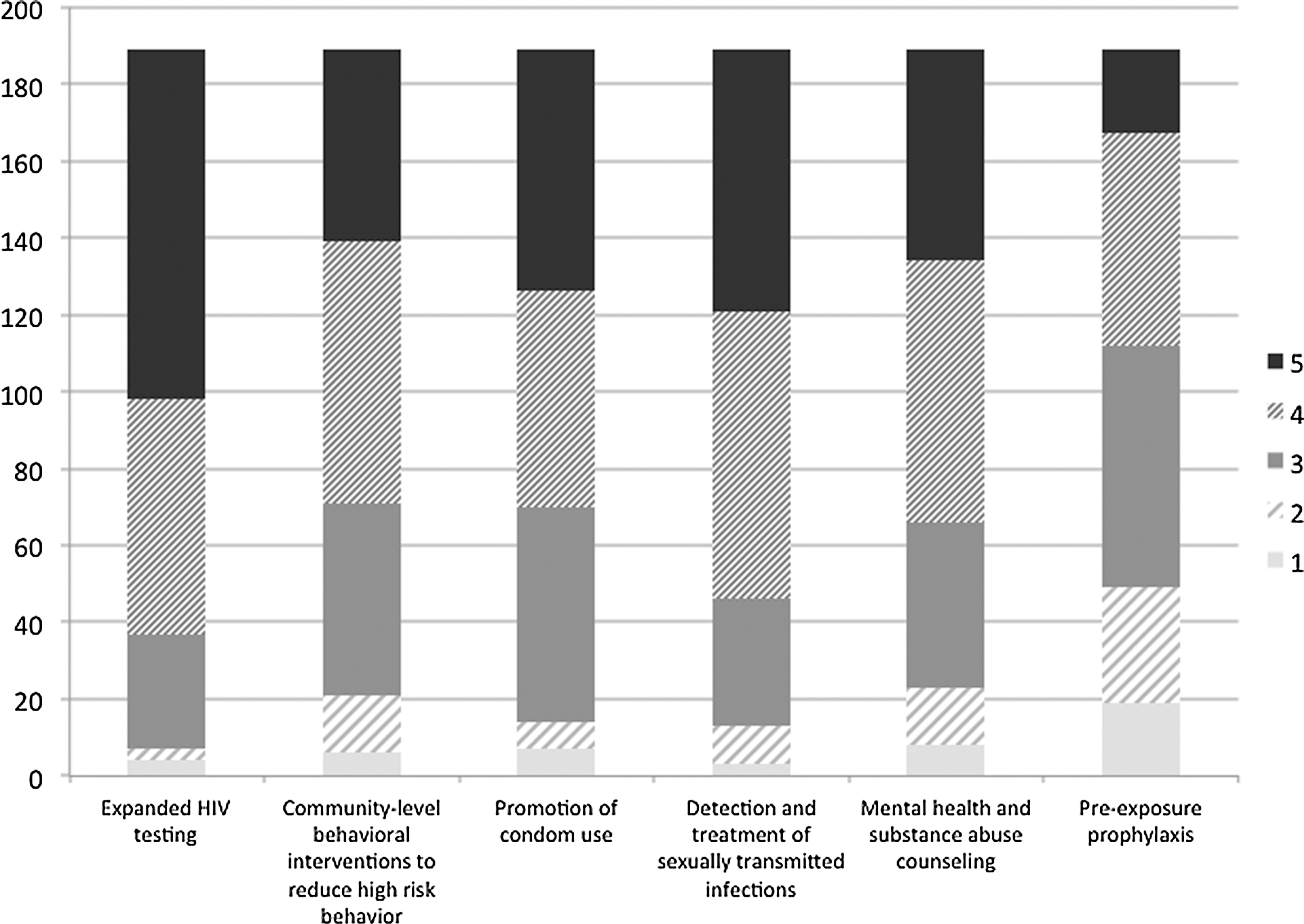
Summary of responses to PrEP survey question: “How would you rate each of the following factors in its ability to decrease the acquisition of HIV infection (1-least effective, 5-most effective)?”
A scenario was provided regarding a healthy, 50-year-old heterosexual female in a monogamous relationship with an HIV-positive partner who does not use condoms. Sixty percent of respondents indicated that they would provide PrEP to a female patient in this setting. Twenty-six percent would not provide PrEP based on lack of scientific evidence, and 14% would not provide PrEP for other reasons.
Seventy-nine percent of respondents felt that PrEP should be covered by private insurance policies or publicly funded sources for individuals at highest risk for HIV infection, provided they are willing to be adherent to the medications or that they meet specific eligibility criteria for PrEP. Forty percent of respondents felt that funding for PrEP research and development could be spent on other methods of HIV prevention and treatment.
Post-exposure prophylaxis
In order to compare survey respondents' experiences with a related medical intervention for HIV prevention, which has not been completely proven to be efficacious, 16 they were asked if they had ever prescribed post-exposure prophylaxis (PEP) for the prevention of HIV infection to healthcare workers. Seventy-nine percent (N=150) of providers stated they had prescribed PEP in this setting. Twenty-two percent of providers (N=42) indicated they provided PEP to healthcare workers more than 10 times.
When asked if they had ever prescribed PEP for the prevention of HIV for non-occupational exposures, such as for sexual or drug use-related exposure. Seventy percent of providers (N=132) indicated they had provided PEP for this purpose. Twenty-three percent of providers (N=44) indicated they had provided PEP for this scenario more than 10 times.
Discussion
This is the first nationwide survey to document the knowledge, attitudes, and prescribing practices of HIV healthcare providers regarding PrEP in the United States. While HIV providers were the group targeted in this study, PrEP may ultimately be more prescribed by primary care clinics, as opposed to HIV clinics. Thus, while this study may be a good starting point to establish the attitudes of providers towards PrEP, nonspecialty providers would be an important group for future studies. Other surveys conducted in the United States questioning providers about their attitudes and use of PrEP have been limited to specific geographic areas. 13,17,18 While these studies have suggested a willingness of providers to adopt PrEP, these studies documented providers' concerns about PrEP's safety, efficacy, and cost.
Most surveys about PrEP conducted in the United States have interviewed potential patient populations. These surveys have focused on MSM, transgender populations, and HIV-serodiscordant male couples. MSM community members have reported mixed perceptions on PrEP. Surveys have documented a lack of awareness of PrEP in this population, and one study demonstrated that participants had reservations about using PrEP, even when aware of data from randomized clinical trials. 19,20 The results of surveys documenting the attitudes and perceptions of PrEP among HIV-serodiscordant male couples have also been mixed. One study demonstrated low endorsement of PrEP uptake, while another demonstrated a high level of acceptability of PrEP. 21,22 Another study identified the attitudes towards PrEP in a heterosexual population. The authors found that despite having knowledge about HIV transmission risks, high-risk participants did not recognize their risks, and this was correlated with a lack of interest in PrEP. 23
Our survey was completed by members of and HIV Specialists™ credentialed by the AAHIVM, which has members in all 50 states and some international members and credentialees as well. A majority of these healthcare providers were familiar with both the results of iPrEx study and the 2011 CDC interim guidance for PrEP use in MSM. Thus, this survey is best interpreted as a baseline of the attitudes and prescribing practices that developed in response to these two publications.
While a majority of providers prescribed PrEP for MSM patients, our survey demonstrated that many providers prescribed PrEP to heterosexual males and females. In our survey, 60% of respondents stated that they would provide PrEP to a female patient with an HIV-positive partner who does not use condoms. Before the survey began, the CDC interim guidance only recommended PrEP in MSM populations. 8 At the beginning of the survey period, a press release announced the discontinuation of the FEM-PrEP study due to the futility of oral PrEP in women. 14 In the latter half of the survey period, the results of the Partners PrEP and the TDF-2 trials, demonstrating the efficacy of PrEP in heterosexual adults, were presented at the IAS conference, but had not yet been published. 15 While a large majority of survey respondents reported familiarity with both iPrEx study results and CDC interim guidance for use of PrEP in MSM, it appears that respondents extrapolated that PrEP can be used with at-risk women, despite conflicting data during the survey period. Potentially, assumptions were made regarding PrEP use in women even prior to or in spite of research data at the time of the survey. After this survey was completed, new CDC interim guidance for PrEP use in at-risk heterosexual adults was published. 24 This guidance states that PrEP can be one of several options to reduce the chances of an HIV-negative partner in an HIV-serodiscordant relationship from acquiring HIV.
A majority of HIV care providers were compliant with CDC interim guidance in their use of PrEP. The lowest level of compliance (61%) was found in screening for HBV infection before the initiation of PrEP. Additionally, only 75% screened for acute HIV infection if their patient had typical symptoms. Per CDC guidance, PrEP should not be started in patients with signs or symptoms of acute retroviral infection. In such cases, HIV-negative status should be confirmed by an undetectable HIV RNA assay or a negative repeat anti-HIV antibody test following the illness to minimize the risk of antiretroviral resistance. 8 Thus, our survey indicates a need for increased education of potential prescribers of PrEP regarding optimal pre-screening prior to use of PrEP. Since missing either pre-existing HBV infection or acute HIV infection can have serious detrimental health effects on patients receiving PrEP, efforts aimed at these points provide a significant medical education opportunity.
Respondents indicated that the most common reasons for discontinuing PrEP were either that the patient was no longer at high risk for HIV or the patient preferred to stop the medication. Adverse effects of FTC/TDF were not a major reason for discontinuation of PrEP in our survey. However, on a subsequent question, 62% of respondents (N=118) stated that possible adverse effects of antiretrovirals would influence their decision to prescribe PrEP to an otherwise healthy HIV-seronegative individual. Despite this concern, several clinical trials of PrEP have documented the relative safety of FTC/TDF compared with placebo. In the Partners-PrEP study, there were no significant differences in the frequency of serious adverse events or serum creatinine abnormalities across the three study groups. 5 The iPrEx study found no difference in the rates of discontinuation of FTC/TDF versus placebo, although there were more serum creatinine elevations in the FTC/TDF arm. However, most of these were found to be self-limited and were not confirmed on repeat testing. 4
The fact that some survey respondents noticed less high-risk behavior reported by their patients, and thus discontinued PrEP, may suggest a beneficial longer-term effect of using PrEP. During the iPrEx study, the total numbers of sexual partners reported by study subjects decreased and condom use increased. 4 The iPrEx study investigators surmised that taking daily medication may serve as a reinforcement to decrease high-risk sexual behavior. Similarly, in the TDF2 study, risky sexual behavior did not increase among the participants receiving the study medication. 6 Likewise, the Partners-PrEP trial also demonstrated a decrease in high-risk sexual behavior after enrollment. 5
A common concern about PrEP by HIV healthcare providers in this survey was the potential for the development of antiretroviral resistance. None of the PrEP trials published to date have documented any significant antiretroviral resistance among the participants taking PrEP. Interestingly, in the iPrEx study, no FTC or TDF resistance was detected among study subjects who became infected with HIV during the trial in either study arm. 4 In the Partners-PrEP study, four participants became infected with HIV that was resistant to non-nucleoside reverse-transcriptase inhibitors (NNRTIs). However, this was felt to be secondary to transmitted resistance, as opposed to selection of resistance mutations by the study medication. 5 Drug resistance is predicted to occur if patients acquire HIV infection while receiving PrEP and obtain refills without seeing their PrEP provider. Thus, regular medical follow-up is mandatory to ensure that patients remain HIV seronegative. Currently, the CDC interim guidance for use of PrEP in both the MSM and heterosexual populations indicate that no more than a 90-day supply of FTC/TDF should be prescribed, and that an HIV antibody test should be performed every 2–3 months and even more frequently for patients with inconsistent adherence. 8,24
Medication adherence was also a concern by many survey respondents. Both the iPrEx and Partners-PrEP studies showed the efficacy of PrEP depends largely on the degree of medication adherence based on plasma drug concentrations. As mentioned previously, in both the FEM-PrEP and VOICE studies, neither oral FTC/TDF or TDF nor TDF gel was found to be effective in preventing HIV acquisition in women at-risk for HIV. In the VOICE study, this was attributed to the fact that less than 30% of the women in each of the three active agent groups had detectable plasma TDF levels. 11 In the FEM-PrEP study, less than 40% of HIV-uninfected women in the FTC/TDF group had evidence of recent pill use. 10 Thus, regular medication adherence plays an essential factor in the utility of PrEP.
PrEP prescribers differed in our survey as to the appropriate target populations for PrEP use. An HIV-negative person in a relationship with an HIV-positive partner (serodiscordance) carried the greatest weight when deciding to prescribe PrEP. This response was also most prevalent in the UCSF survey, described previously, in which serodiscordant couples were seen as the ideal candidates for PrEP. 13 In that study, it was noted that the target population may be ultimately decided by patients' insurance coverage. This was followed by a patient with multiple sexual partners. Privately insured patients may have a lower barrier to PrEP prescription, whereas public health clinics may selectively target only high-risk individuals. Although the cost of medication was a lesser concern for the HIV providers in our study, it is unknown whether insurers will cover PrEP, and without insurance, out-of-pocket expenses may make PrEP more inaccessible. 25
The great majority of the HIV providers in our survey prescribed post-exposure prophylaxis for both healthcare workers and for non-occupational exposures to HIV. These data interestingly indicate a greater willingness by HIV-treating providers to prescribe PEP, rather than PrEP, despite that the efficacy of PEP has not been proven by randomized-controlled trials. Possible explanations for this discrepancy in evidence-based practice could be the following: (1) personal experience with potential HIV exposures, (2) the longer history of PEP compared to PrEP use, and therefore comfort level, (3) a lack of confidence in the data from the multiple clinical trials discussed here regarding PrEP, or (4) a combination thereof.
There are several potential limitations to our survey results. First, only about 10% of the HIV providers who were sent our questionnaire submitted their responses. Thus, these responses may not be an adequate reflection of the knowledge levels, attitudes, and prescribing practices regarding PrEP for the majority of HIV specialists. Second, our survey was sent only to HIV-treating providers, and did not include community health clinics, primary care physicians, or sexually transmitted infection-treating clinics. Providers who primarily see HIV-seronegative patients, such as general practitioners and primary care physicians, may have significantly different levels of knowledge, concerns, attitudes, and prescribing practices regarding the use of PrEP. The majority of the individuals surveyed here are focused primarily on care of HIV seropositive individuals. Thus, these survey results may not reflect the attitudes and practices of healthcare providers who commonly care for persons for whom PrEP is recommended. Third, while the details of the iPrEx study and the CDC interim guidance for use of PrEP in MSM were published, details of other clinical trials were not yet published when the survey began. Given the novelty of the intervention at the time our survey was completed, this may have contributed to the lower use of PrEP. Additional studies that have been published, which supported the use of PrEP in other populations, may have contributed to further knowledge and usage of this intervention. Finally, our data were obtained entirely by the use of an anonymous on-line survey. Other studies that have documented the attitudes and prescribing practices of PrEP have used a one-on-one interview method. While fewer individuals may be questioned with an interview format, more information can be obtained from each interviewed subject, which may increase an understanding of their prescribing methods and attitudes.
This study demonstrates that while a majority of providers were aware of the efficacy of PrEP in preventing HIV acquisition, there were still concerns raised about the development of drug resistance, medication adherence issues, increased risky behavior, and potential medication side effects of using antiretrovirals in HIV-seronegative adults. The majority of responders felt that PrEP is best suited for use by the HIV-seronegative member of a serodiscordant relationship. HIV practitioners felt comfortable prescribing PrEP to women at the time of this survey, even though at least one study demonstrated a lack of efficacy during the study period. The clinical significance of this study is that it documents that more specific and detailed guidance of PrEP is needed, given the differing use and attitudes towards PrEP among HIV providers. If PrEP is going to be implemented on a widespread basis, this study gives light to the fact that providers need additional guidance for implementation and education on proper prescribing practices. Particularly, there is evidence from this study that more education and awareness of CDC recommendations would be useful, especially in testing for pre-existing HBV and/or recent HIV infection. While the majority of completed clinical trials clearly support the safety and efficacy of PrEP, its optimal delivery methods to at-risk persons, especially women, remains unclear. Of note, four of the trials discussed here have defined the critical relationship between medication adherence and efficacy. To realize the true public health impact of PrEP, additional studies will be needed to test novel dosing strategies and delivery methods among persons at high risk for HIV infection.
Footnotes
Acknowledgments
The authors thank Jim Friedman and Bruce Packett of the American Academy of HIV Medicine for assistance with collecting the data contained in this article.
Sources of Support: None.
Author Disclosure Statement
Dr. Tellalian and Dr. Maznavi have no conflicts of interest. For Dr. Bredeek: Contracted Research, Gilead Sciences; Speakers Bureau, Gilead Sciences; Honoraria For Consulting, Gilead Sciences. For Dr. Hardy: Contracted Research via Cedars-Sinai Medical Center, Gilead Sciences; Honoraria for Consulting, Gilead Sciences.