
Abstract
HIV/AIDS is a chronic illness, with a range of physical symptoms and psychosocial issues. The complex health and social issues associated with living with HIV mean that people living with HIV/AIDS (PLWHA) have historically often turned to complementary and alternative medicine (CAM). This article provides an overview of the literature on HIV and CAM. Databases were searched using keywords for CAM and HIV from inception to December 2012. Articles in English and in Western countries were included; letters, commentaries, news articles, articles on specific therapies and basic science studies were excluded. Of the 282 articles identified, 94 were included. Over half reported prevalence and determinants of CAM use. Lifetime use of CAM by PLWHA ranged from 30% to 90%, with national studies suggesting CAM is used by around 55% of PLWHA, practitioner-based CAM by 15%. Vitamins, herbs, and supplements were most common, followed by prayer, meditation, and spiritual approaches. CAM use was predicted by length of time since HIV diagnosis, and a greater number of medications/symptoms, with CAM often used to address limitations or problems with antiretroviral therapy. CAM users rarely rejected conventional medicine, but a number of CAM can have potentially serious side effects or interactions with ART. CAM was used as a self-management approach, providing PLWHA with an active role in their healthcare and sense of control. Clinicians, particularly nurses, should consider discussing CAM with patients as part of patient-centered care, to encourage valuable self-management and ensure patient safety.
Introduction
HIV is now a manageable chronic illness, 4 –6 with life expectancy in the developed world similar to that of people without HIV. 7 PLWHA experience a range of physical symptoms and psychosocial issues, some in common with other chronic diseases, some unique. These include abnormal psychology, mood and related disorders, personal and social uncertainty, identity issues, stigma, social isolation, poor quality of life, and unemployment, 5 and a range of side effects from ART such as gastrointestinal and dermatological effects, cardiac and liver problems, and bone loss. 8 The impact of HIV on physical and emotional health may be worse than for many other chronic diseases. 9 CAM is still often used to address these complex health and social issues associated with living with HIV/AIDS, 10 including stress reduction, relieving side-effects and symptoms, and boosting the immune system. 11
It is important that conventional clinicians are aware of CAM use and, where appropriate, discuss its use with their patients, both to improve the practitioner-patient relationship and adherence to ART, and to identify potential safety issues. 12,13 Practitioners therefore need to have up-to-date knowledge regarding CAM use. Previous reviews have often focused only on the prevalence and determinants of CAM use, often with a methodological rather than clinical focus; 14,15 this review aims to provide a broader overview of the current literature on the use of CAM for PLWHA to identify issues which may have implications for patient care.
Methods
The following databases were systematically searched in December 2012 with no date limits: Medline, Cinahl, PsycArticles, AMED, Sciencedirect, Cochrane library. Search terms were for HIV and complementary therapy/medicine (Table 1).
In order to identify studies with relevance for patient care in the UK and other Western countries, inclusion criteria were: about complementary or alternative medicine and HIV; in English; based in a Western country. Exclusion criteria were: studies on a specific CAM therapy; letters, commentaries, news articles; basic science studies (animal or lab-based).
Results
A total of 282 articles were identified, 119 were excluded from reviewing the titles, and a further 71 from screening abstracts, leaving a total of 91 articles for review. See Fig. 1 for details. Many of the studies were conducted in the USA. The 91 articles were published between 1989 and 2012 and were grouped as below:
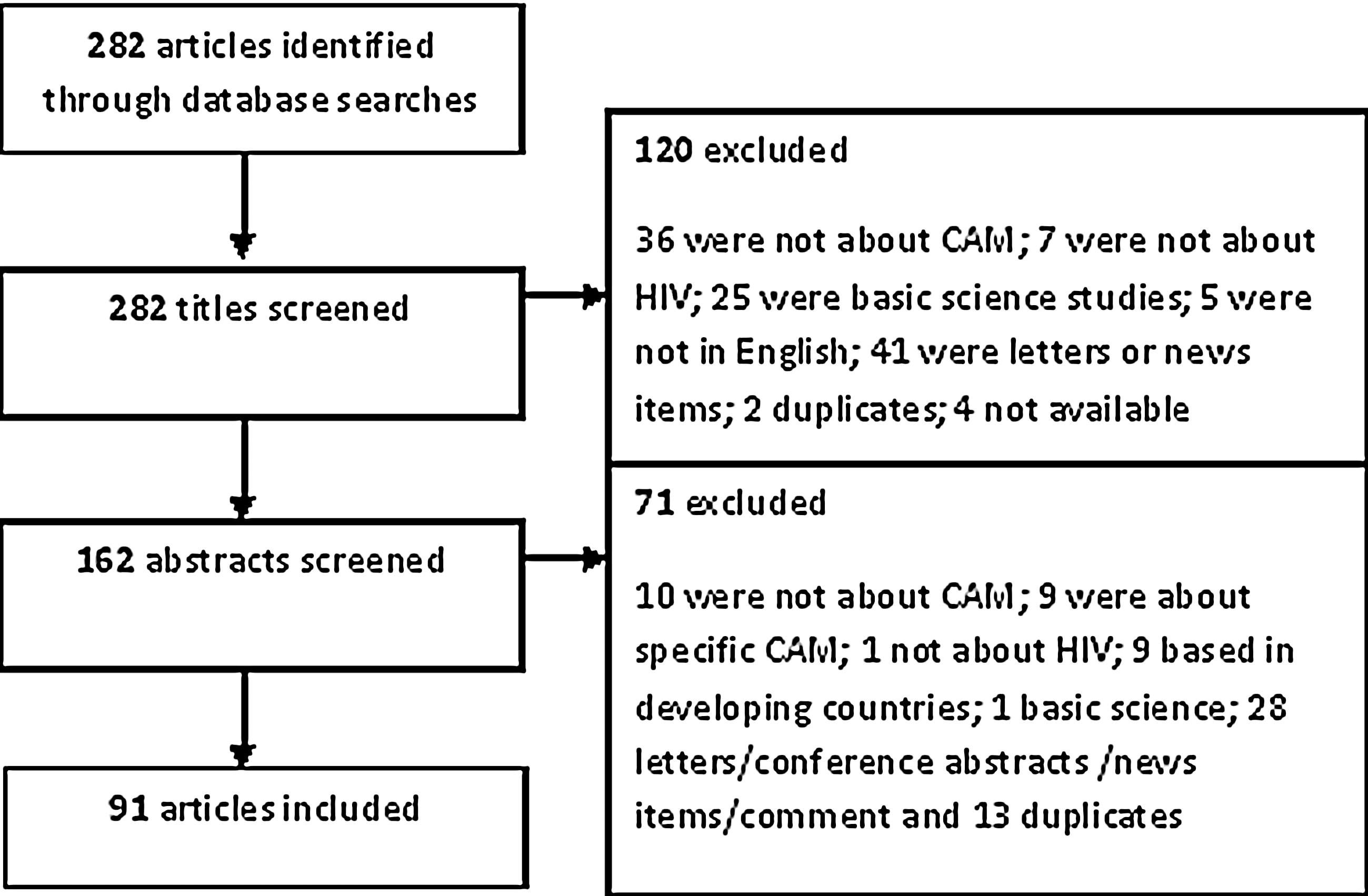
Flowchart of study selection.
• Studies of the prevalence and determinants of CAM use for PLWH—54 articles 14 –68
• Studies of PLWHA attitudes to CAM, reasons for use and decision-making process—15 articles 10,69 –81
• Overviews of the evidence for CAM—nine reviews 82 –90 and one two-part overview of the use of CAM in HIV 91,92
Prevalence
Of the 54 articles identified on the prevalence of CAM use, one was a systematic review 15 and there were three other reviews. 14,45,46 Thirty-five were carried out in North America, 16,19 –56,64 five in Europe, 57 –61 and two in Australia. 62,63 Three studies used national samples. 52,63,64
Prevalence figures for lifetime use of CAM varied from 30% to 90%; use over the past 6–12 months ranged from 15.4% to 100%. Variations in prevalence figures are partly due to differing definitions of CAM, for example, when restricted to practitioner-based CAM, prevalence was only 15–16%. 32,35 The three national studies 35,63,64 and two multistate studies 32,34 give the most externally valid results. They suggest that CAM is used by around 55–60% of PLWHA; 63,64 15–16% practitioner-based CAM. 32,35
Vitamins, herbs, and supplements were the most common approaches used, followed by prayer, meditation and spiritual approaches, massage, and acupuncture.
Higher levels of education and being female were the most common predictors of CAM use (reported as significant in 13 16,20,22 –24,28,30,32,36,57,59,62,63 and seven 19,23,31,59,62,63,66 studies, respectively). Other determinants were Caucasian, 23,28 higher income, 20,35 gay/lesbian, 24,35 younger, 20,63 and having depression. 25,35 HIV-specific predictors included longer disease duration/time on ART (5 studies 16,21,36,57,62 ), and using a higher number of medications (2), 19,60 more symptoms/infections (3), 25,36,57 and ART side effects (2). 16,59 CAM use was associated with having an HIV diagnosis; 43 and Carwein and Sabo 27 found that 100% of participants with HIV used CAM, compared to 16% before HIV diagnosis. Other predictors suggest an association with having a more active role in healthcare, for example, reading more information or having more health promoting behaviours. 25,26,35,63
Reasons for use varied, from reducing symptoms and improving well-being to improving immunity. Five studies reported the use of CAM for people with specific symptoms (depression, 51,65 anxiety, 56 peripheral neuropathy, 55 and pain 52 ). In these studies, prayer and meditation were preferred options and use varied from 18% to 52% of respondents. CAM use was associated with less illicit drug use in one study. 48 Four prevalence studies specifically focused on adherence to HAART therapy, 47 –49,61 but results were equivocal, with no firm pattern suggested as to whether adherence was improved as a result of CAM use.
Given the strong influence of the introduction of HAART, particularly the latest one-pill-once-daily regimens, on the behaviour, treatment, and lifestyle of PLWHA, 101 we compared prevalence articles published pre- and post-modern HAART regimens (i.e., before/after 2005 when single dose regimens became widely available and recommended). 4,102 –104 However, there were no differences in prevalence figures, determinants, or reasons for use, suggesting that ART does not have a strong influence on CAM use by PLWHA, discussed further below.
Attitudes to CAM, reasons for use and decision-making
Fifteen studies were identified regarding patients' attitudes to CAM, reasons for use and decision-making. Ten were north American, 67,69,71 –74,77 –79,81 four from Australia, 10,70,76,80 and one from Switzerland. 75
One of the key reasons for using CAM was to provide a method to self-manage health or to give a sense of control, 10,71,77,80 to cope with uncertainty, 71 manage symptoms, 71 give freedom from and additional choice to medical regimens, 10,71,76,80 and attempt to normalize health status, maintain health, or find wellness. 71,77,78 CAM was also used for personal growth or fulfilment 77,78 with different CAM used along a journey, from those focusing on the physical self to those facilitating inner awareness, such as meditation. 77
Another key reason was to address the limitations or problems with conventional ART. 70,80,81 However, most studies found that CAM users did not reject conventional medicine; 78 only one study found that a preference for CAM predicted non-use of ART. 74 In fact, one study found that patients used conventional parameters such as CD4 counts to make their decisions about CAM. 79
One study described the decision-making process of selecting a CAM, often based on friends and family, judging which approaches work and are safe, from subjective personal experience, attempting to combine conventional medicine and CAM. 73 Cultural values appear likely to influence the decision to use CAM. 69,78 One study found that psychologically needier people were more likely to seek CAM. 75
Barriers to CAM use include cost, access, time/discipline/energy needed, overwhelming choice, and the need for evidence. 72,73
Guidance for clinicians
Six articles were identified giving guidance for clinicians, looking at the issues of combining CAM with HIV conventional medication. 12,13,93 –96
Four articles provided guidance for nurses to make decisions regarding CAM, advising that nurses discuss CAM use with their HIV patients. 13,93,95,96 Irish, although this article is now very outdated, suggests that discussing CAM with patients is part of nurses' obligation to provide patient-centred care, and that nurses should assess whether CAM are harmful and encourage disclosure by being nonjudgmental, which can help to maintain health. 13 Palmer provides an overview for HIV nurses on CAM, CAM use and reasons, safety issues, and benefits. 93 He concludes that nurses have an ethical obligation to provide patients with up-to-date information about CAM products so that they can make an informed choice. 93 Haddad presents a clinical scenario of a patient with HIV who wishes to use CAM instead of conventional treatment. 95 She discusses the need for nurses in this situation to avoid jumping to the conclusion that they should dissuade the patient and instead suggests exploring the reasons behind the patient's wishes, particularly any concerns about conventional treatment, and ensuring the patient makes an informed decision. Freeman and MacIntyre also advise that nurses have an understanding of CAM in order to improve their relationships with patients. 96
The other two articles, 12,94 although somewhat outdated, potentially provide useful HIV-specific guides to a range of CAM. Steinberg 94 also provides some suggestions for how conventional practitioners, or PLWHA themselves, can integrate CAM and conventional treatment. This includes ‘finding the right balance’, ‘dealing with uncertainty’ regarding new symptoms and illness progression, ‘anger’ related to the social/financial impact of HIV, ‘nonexclusivity’ (using CAM to complement other treatments), and encouraging patient responsibility and empowerment. Elion and Cohen 12 emphasise the need for discussion and disclosure of CAM use, for safety reasons, but also issues of cost, fraud and the evidence-base.
These articles illustrate how a discussion of CAM can form part of nurses' holistic and patient-centered care of PLWHA and emphasize the need for primary care providers and nurses to engage in dialogue with patients regarding CAM, and encourage disclosure by being nonjudgmental.
Reviews of treatments
Nine review articles provided descriptive information on various treatments 82 –90 and a two-part review additionally covered a range of other issues. 91,92 Reviews on the effect of CAM were generally positive and suggest that CAM has a potential use for a range of health issues, 84,86 –89,105 although many highlighted that the evidence base is still inconclusive. Massage therapy 84,105 and stress management 86,87 were highlighted as the CAM most likely to be beneficial treatments. Two reviews highlighted the limitations of the evidence base, which was seen as insufficient to support use of any CAM. 85,90
Safety
Only four articles were identified regarding the safety of CAM and HIV, plus the Spanish study by Vaszquez et al., which includes safety information. 61 Ernst 97 described some of the risks of CAM, although these were not HIV specific, and then gave a single case study example of an HIV patient being exploited by an ‘energy’ therapy. An article by Gilmour et al. 98 is not specifically about HIV; they describe natural health product–drug interactions in general and the need to ask patients about CAM use, using the case example of an HIV -positive patient taking St Johns wort, which interacts with indinavir. Ladenheim et al. 99 provide a more thorough study of the potential health risks of CAM for PLWHA, using a survey of the use of herbal medicine and supplements among PLWHA to identify any potential risks. They identified 59 patients (20% of those using CAM) whose CAM use necessitated a warning, 29 of whom were advised to stop their CAM use due to concerns about serious interaction with ART or adverse effects. The most common adverse effect was with echinacea (used by 22 patients) which, in theory, could increase the number of infected leucocytes by stimulating the immune system, resulting in increased HIV viral load. Eight patients were using garlic, and two were using St Johns wort, which can both interact with ART, reducing its therapeutic levels. One patient was using kava, which may cause hepatotoxicity. Other CAM being used were not as high a safety risk but patients were advised to use with caution. These included aloe vera, gingko biloba, and vitamin C megadoses, which can reduce the effectiveness of ART, and cat's claw, DHEA, ginseng, liquorice, milk thistle, and red yeast, which can cause ART-related side effects. Vaszquez et al. (included above as a prevalence study) 61 additionally documented potential herbal medicine-ART interactions, which also included echinacea, milk thistle, garlic, ginseng, and cat's claw, as well as grapefruit (can reduce concentrations of indinavir and saqyinavir), valerian (can increase hepatotoxicity), marijuana (reduces Cmax), hypericum (reduces ART effectiveness). Ladenheim et al. highlighted that the main risk of CAM use in PLWHA is potential ART–interaction, through the cytochrome pathways, making CAM use with protease inhibitor and non-nucleoside reverse transcriptase inhibitor ARTs particularly risky. A focus group study identified that safety of CAM is important in patients' decision making, but that they had limited knowledge, although this study was nearly 10 years old. 100
Discussion
CAM appears to be popular with PLWHA, although there is a paucity of recent, large-scale, national survey data, particularly outside of the USA. Prevalence figures vary widely, though this is known to be a common issue in studies of CAM. 106 Vitamins, herbs, and supplements emerge as the most common approaches used, followed by prayer, meditation, and spiritual approaches.
Supplements and herbs may be used for a range of reasons, including cleansing or strengthening the body. 88 Their popularity may be related to a generally high knowledge of nutrition amongst PLWHA, encouraged by the community and by healthcare clinicians. 107 These oral CAM can cause potential safety issues through interaction with conventional medication, in particular ART, with implications for the role of conventional clinicians. 98,99 However, as seen in this review, there is a lack of research on the specific safety implications of CAM use by PLWHA. 3
Prayer, meditation, and spiritual approaches may be used to provide an approach to understanding and coping with chronic illness and providing emotional support and a stabilizing force within daily life. 108 It is important that clinicians understand that these approaches may be important to patients, particularly within the context of patient-centred and culturally-competent care.
CAM use appears related to having an HIV diagnosis 27 and in many of the articles reviewed, CAM use was predicted by having a longer duration of time since HIV diagnosis and a greater number of medications and symptoms. This may relate in part to ART use, as CAM is often used to address the limitations of or problems with ART. This is most likely in a complementary rather than alternative manner, as most studies found that CAM users did not reject conventional medicine but used CAM as part of an integrated approach. 80 Thorpe et al. 10 explain that PLWHA did not want CAM to ‘re-medicalize’ health management but instead used CAM as part of a ‘return to normality’. As well as coping with the side effects of ART, CAM may be used for relaxation, to support a positive attitude and to improve energy levels. 108
A strong theme from the literature was the use of CAM to provide a method of self-management of health or give a sense of control for PLWHA, as evidenced by the high use by those who are active in their own healthcare. This theme has been identified for other chronic illnesses, including cancer. 108,109 Swenderman 110 emphasizes that self-management is as important, and complex, in HIV as in other chronic conditions, with additional HIV-specific challenges related to lack of self-monitoring, stigma, disclosure, and transmission routes. The emphasis on self-management may be related to the “AIDS movement” and activism in the HIV/AIDS community. 3 Encouraging effective self-management of health is important in HIV as it is associated with medication adherence, 111 although this review did not find evidence that CAM use was associated with adherence.
Although it places the emphasis on the patient, healthcare clinicians have a key role in self-management, both providing treatment and advice, as well as encouragement, motivation, and tools. 108,111 Only a quarter of HIV clinicians report asking patients about CAM use, 112 although PLWHA who use CAM still rely on biomedical knowledge and providers to provide certainty. 10 There is clearly a need, even an ethical duty, 3 for conventional healthcare providers to discuss CAM with their patients, including perhaps making informed decisions on the use of CAM and being aware of potential safety implications, particularly interactions between herbal and conventional medicines. 98,113 Although some evidence-based information is available for clinicians, for example, in a range of articles identified in this review, 14,82,83,91,92 there is a need for education of clinicians and perhaps for professional guidance to stipulate discussion of CAM as part of HIV clinicians' duty. 3 There is also a need for further research into CAM for HIV/AIDS, 3 perhaps starting with massage and stress management which show promising preliminary evidence.
Given the numerous similarities identified between HIV and other chronic diseases, emphasizing HIV as a chronic disease may help to encourage self-management, reduce stigma, and expand access to healthcare. 110
In conclusion, CAM is popular with PLWHA, particularly supplements, herbs, and spiritual approaches, and appears related to having an HIV diagnosis. The use of these complementary approaches appears to help PLWHA to cope with symptoms and side effects, but also, perhaps more importantly, to take control of their own health. Clinicians should consider discussing CAM with patients as it may encourage valuable self-management and ensure patient safety.
Footnotes
Acknowledgments
We are grateful to NHS Brent Primary Care Trust for funding this work.
Author Disclosure Statement
No competing financial interests exist.