
Abstract
We sought to develop individual-level Early Warning Indicators (EWI) of virologic failure (VF) for clinicians to use during routine care complementing WHO population-level EWI. A case-control study was conducted at a Durban clinic. Patients after≥5 months of first-line antiretroviral therapy (ART) were defined as cases if they had VF [HIV-1 viral load (VL)>1000 copies/mL] and controls (2:1) if they had VL≤1000 copies/mL. Pharmacy refills and pill counts were used as adherence measures. Participants responded to a questionnaire including validated psychosocial and symptom scales. Data were also collected from the medical record. Multivariable logistic regression models of VF included factors associated with VF (p<0.05) in univariable analyses. We enrolled 158 cases and 300 controls. In the final multivariable model, male gender, not having an active religious faith, practicing unsafe sex, having a family member with HIV, not being pleased with the clinic experience, symptoms of depression, fatigue, or rash, low CD4 counts, family recommending HIV care, and using a TV/radio as ART reminders (compared to mobile phones) were associated with VF independent of adherence measures. In this setting, we identified several key individual-level EWI associated with VF including novel psychosocial factors independent of adherence measures.
Introduction
V
The factors that contribute to VF are complex and interact at multiple levels. 2,3 The World Health Organization (WHO) developed a set of early warning indicators (EWI) designed to identify programs and regions where HIVDR may be of great concern. 4 These EWI include retention on first-line ART, on-time drug pickup at the pharmacy and clinic appointment keeping, and viral load (VL) suppression 12 months after ART initiation. Several countries are using EWI in order to focus efforts towards improving healthcare delivery in those settings with suboptimal EWI scores. 4 –6 Although these “system-level” factors are useful at a programmatic and regional level, clinicians need “individual-level” factors that could help identify and predict which patients may be at risk of VF while on ART or prior to initiation. While many studies have explored psychosocial, structural, or clinical factors associated with clinic retention, ART adherence or VF, none have attempted a comprehensive assessment in this setting. 7 –9
The Risk Factors for Virological Failure (RFVF) study was undertaken to ascertain individual-level factors associated with VF on ART in order to develop EWI for clinicians. For programs that lack resources for systematic VL monitoring, these risk factors can also identify those individuals with potential VF for more targeted use of VL monitoring.
Methods
Clinical setting
The RFVF study was conducted at McCord Hospital (MCH) in Durban, South Africa, which is a regional referral center that has been treating patients with ART since 2002. MCH received partial support from the President's Emergency Plan for AIDS Relief and South African government funding for ART which began in February 2004. Patients pay a monthly fee ($15 USD) for clinic services. Routine viral load (VL) monitoring occurs 5 months after starting ART. All patients receive initial ART education. Pharmacy refills and pill counts are recorded for each patient in the clinic. If the VL was≤1000 copies/mL (cpm), patients are maintained on this regimen and followed with annual VL monitoring thereafter. If the VL was>1000 cpm, a repeat VL is done 1–3 months later with concurrent adherence counseling. If the VL remains>1000 cpm, regimen changes are considered based upon the level of adherence and resistance testing which is performed on all cases.
Study participants
From October 2010 through June 2012, all individuals with HIV attending the MCH HIV clinic≥18 years who were receiving≥5 months of their first ART regimen (substitutions allowed for toxicity) were offered participation in this study if they met the criteria for a case or control.
Study design
An unmatched case-control design was chosen for this study because the rate of VF was too low to justify a prospective cohort study and the intention was to allow for investigation of all potential risk factors. Cases were defined as patients having an initial VL>1000 cpm after≥5 months of their first ART regimen. Controls (2:1) were defined as patients with virologic suppression (VL≤1000 cpm) on≥5 months of their first ART regimen. In general, cases were identified as having VF within 1–2 weeks of a visit to the clinic (which corresponded to a pharmacy refill). These patients were notified and enrolled into the study if they agreed to participate within 1–2 weeks from that date. Their enrollment date was therefore 2–3 weeks from the most recent refill. Controls were randomly selected patients in the clinic who met the eligibility criteria and agreed to participate. Their date of enrollment corresponded to a pharmacy refill date.
Data collection
All participants who provided consent and were enrolled into the study underwent a single, semi-structured interview in their preferred language with the research coordinator who was blinded to the participant's case-control status. This interview consisted of a questionnaire, validated neurocognitive assessment, 10 the Kessler 10 (K-10) depression scale, 11 and an unannounced pill count. The questionnaire contained demographic, socioeconomic (including a wealth index, 12,13 employment, education, and cohabitants), psychosocial (including substance abuse, 14 food insecurity, 15 –17 traditional African medicine use, safe sex practices, faith, stigma, 18 and intimate partner violence 19 ) and clinic satisfaction indices. 20 There were also specific questions about ART adherence and clinic attendance based upon a modified AIDS Clinical Trials Group (ACTG) adherence questionnaire. 21 The study physician met with each patient to review their medical history, as well as to administer the symptom screen and Karnofsky score. 22 Clinical information, 1 pharmacy refill dates/quantities, and laboratory data were abstracted from medical records and entered onto a case report form (CRF). Further details of the data collected can be found in Table 1. Study data were managed using REDCap electronic data capture tools hosted at Emory University. 23
ACTG, AIDS Clinical Trials Group; ART, Antiretroviral Therapy; ARV, Antiretroviral; DHS, Demographic and Health Survey; HFIAS, Household Food Insecurity Assessment Scale; MPR, Medication Possession Ratio.
Statistical analysis
Two explanatory covariates were derived from the primary data collected. The “Access” covariate incorporated antiretroviral (ARV) refill dates and quantity dispensed. This formula was based on the medication possession ratio (MPR) 24 accounting for all refills occurring in the 180 days following the earliest refill date until enrollment. The “Adherence” covariate utilized the enrollment date pill count and incorporated the dispensed pills over the previous 180 days. 25,26 The primary outcome assessed in this study was the dichotomized participant assignment as a case or control. Separate sensitivity analyses used a VL threshold of >50 cpm. All variables from the questionnaire and CRF, as well as explanatory covariates, were independently analyzed for their association with the primary outcome in univariable analyses. Although all variables were examined, only significant (p<0.05) and epidemiologically important factors were further analyzed. Individual analyses by domain were undertaken to identify appropriate variable categories, correlations, and interactions between variables and ascertain which variables have the highest likelihood of success in multivariable models. Several logistic regression multivariable models were constructed using model selection to arrive at each final model. Model 1 (baseline factors) attempted to identify the factors present at the initiation of ART most associated with the primary outcome. Model 2 included all time-updated variables except for the Access or Adherence measures. Model 3 included those socioeconomic and psychosocial variables from Model 2 that were likely to be correlated with the Access measure. Model 4 included those psychosocial, symptom, and clinical variables from Model 2 that were likely to be correlated with the Adherence measure. Model 5 was considered the full model including all time-updated variables and the Access and Adherence measures. Receiver operator characteristic (ROC) curves were constructed for each model. Subgroup analyses were performed to assess variables associated with VF among those individuals having only 12 months of first-line ART. All statistical analyses were performed in SAS (SAS Institute, Version 9.3, Cary, NC).
Ethics
The RFVF study was approved by the ethics committee at McCord Hospital and by the institutional review board at Emory University in Atlanta, Georgia.
Results
Cohort description
Only the significant and otherwise important characteristics of study participants are shown in Table 2. Overall, the mean age was 39.6 years old and 64.6% were women. Over 78% received an income and 19.0% were unemployed. Sixty-five percent reported having a current partner, and 41.5% reported disclosing their status to a partner. The mean (SD) K-10 score was 12.8 (3.4) with 55.0% scoring >12. The most commonly reported symptoms were depression (34.5%), a rash (32.5%), and fatigue (32.1%). Nearly half (43.9%) felt their symptoms were related to ARVs. Only 34.7% of participants had no obvious neurocognitive impairment, while 35.4% had evidence of HIV-associated dementia. Lipodystrophy was documented in 29.5% of participants. The median (IQR) CD4 count was 300.5 cell/μL (183.5–448.0), and tuberculosis was the most frequent opportunistic infection (54.8%). The mean (SD) duration of ART was 30.2 months (24.3). The vast majority of participants (88.9%) used their mobile phone to remind them to take ARVs or visit the clinic. The median (IQR) MPR was 1.03 (0.96–1.07), and median (IQR) pill count adherence ratio was 1.12 (1.05–1.17). Cases and controls differed substantially across all of the domains examined using univariable comparisons.
ANI, asymptomatic neurocognitive impairment; ART, ARV treatment; ARVs, antiretrovirals; ETB, ethambutol; HAD, HIV-associated dementia; INH, isoniazid; K-10, Kessler 10 depression scale; MND, mild neurocognitive disorder; MPR, medication possession ratio; RIF, rifampicin; TM, any form of traditional (African, Chinese, Indian) or alternative/complimentary medicine; TS, trimethoprim-sulfamethoxazole; UE, unemployed (seeking work or not seeking work); VL, viral load.
Baseline risk factors (Model 1)
Younger age and male gender were associated with VF in nearly all MV models (Table 3). Additional risk factors for VF that were likely present at ART initiation included having a treatment supporter (OR 1.991), not having or not being active with a religious faith (1.634), having at least one family member living with HIV (1.613), having had a family member recommend the individual to seek ART, use of stavudine (d4T) in the current ART regimen, and use of fluconazole (4.973). The ROC area under the curve (AUC) for baseline risk factors was 0.7824 (Fig. 1A).
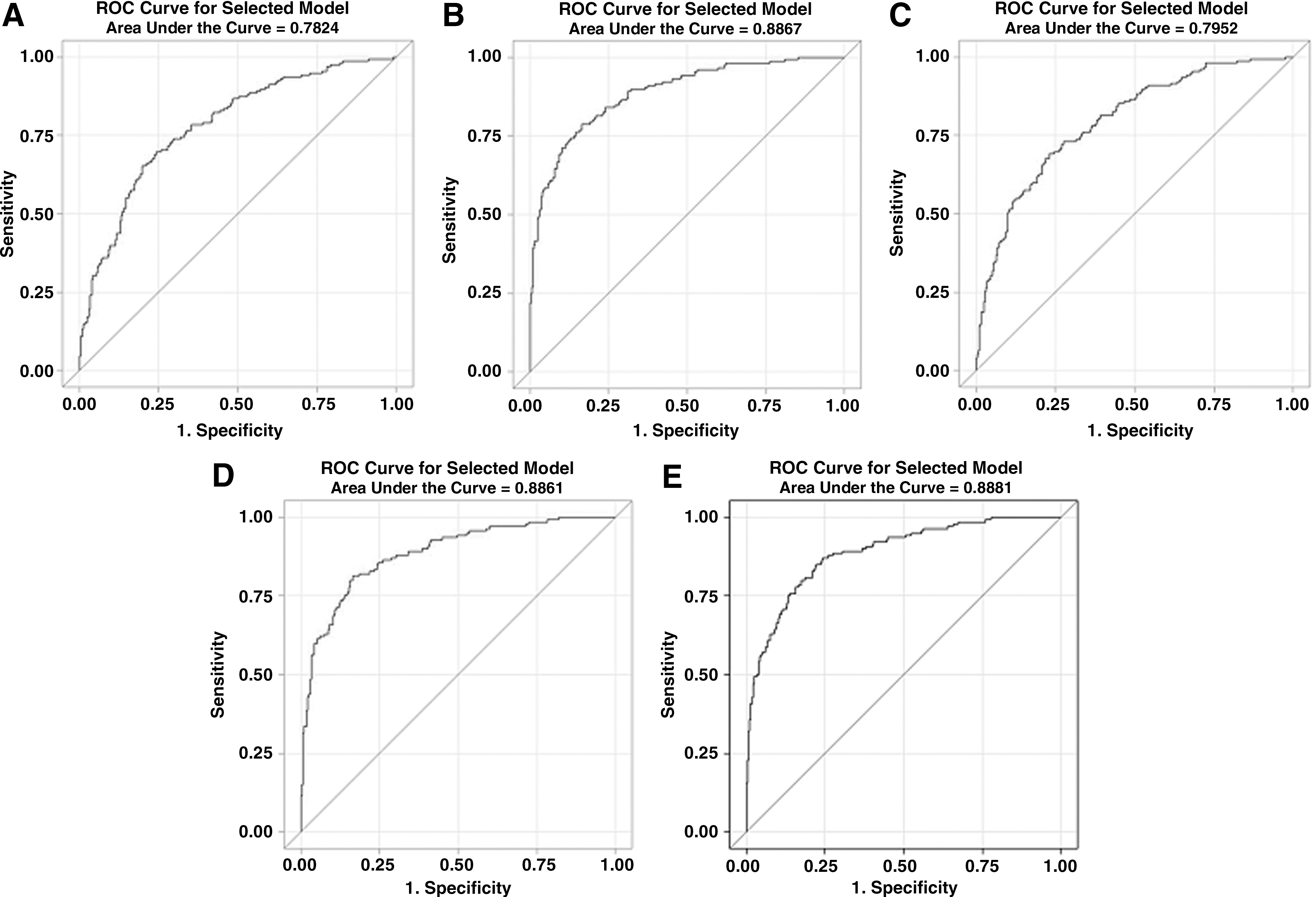
Receiver operator characteristic curves for multivariable models 1–5
Odds ratios presented; a p<0.10, b p<0.05, c p<0.01, d p<0.001; eAdjusted for ARV duration which was significant; ARV, antiretroviral; Model 1, baseline variables (excluding any time updated variables); Model 2, full model without access or adherence variables; Model 3, socioeconomic and psychosocial adjusted for access (forced); Model 4, psychosocial, symptoms, clinical events and meds adjusted for adherence; Model 5, full model with Access and Adherence forced; — variable or domain was excluded a priori.
Overall risk factors excluding Access or Adherence measures (Model 2)
In a full MV model that included all domains except Access and Adherence, the factors that were associated with VF at the time of study enrollment included less than always practicing safe sex (5.500), not being pleased with their clinic experience (2.232), K-10 score >12 (3.136), symptoms of fatigue (2.532) and diarrhea (2.555), the absence of lipodystrophy (2.366), having lower recent CD4 counts (12.658), having a family member recommend the individual to seek ART, and having used a TV or radio as a reminder to take their ARVs (3.519) instead of a mobile phone. The ROC AUC was 0.8867 (Fig. 1B).
Access-related risk factors (Model 3)
In a MV model that included the Access measure, the following remained significant after adjusting for the Access variable: practiced unsafe sex (3.108), K-10 >12 (3.064), and not being pleased with their clinic experience (2.584). The ROC AUC was 0.7952 (Fig. 1C).
Adherence-related risk factors (Model 4)
Factors known to influence Adherence that remained significant after adjusting for the Adherence variable included not having or not being active with a religious faith (1.854), not being pleased with their clinic experience (1.934), practiced unsafe sex (5.905), K-10 >12 (2.689), symptoms of fatigue (2.471) or rash (2.011), low recent CD4 count (12.821), family member recommended the patient to seek ART, the use of d4T in the current regimen, and using a TV/radio as a reminder for ARVs (3.363). The Adherence measure was also significant (1.328). The ROC AUC was 0.8851 (Fig. 1D).
Overall risk factors including Access and Adherence measures (Model 5)
After adjusting for both the Access and Adherence variables, the following remained associated with VF: practiced unsafe sex (5.023), having at least one family member living with HIV (2.000), not being pleased with their clinic experience (1.965), K-10 >12 (3.021), symptoms of fatigue (2.470) or rash (1.992), low recent CD4 count (12.821), family member recommended the patient to seek ART, and used a TV/radio as a reminder for ARVs (3.681). Again, Adherence was significant (1.311), while Access had to be removed due to high collinearity with Adherence. The ROC AUC was 0.8881 (Fig. 1E).
Sensitivity and subgroup analyses
The following sensitivity and subgroup analyses (data not shown) are described in terms of how they differed from the whole cohort analyses. When the outcome was changed to a VL threshold of>50 cpm, there were 265 controls and 193 cases (35 participants, 7.64%, were reclassified). Only six participants had a VL between 200 and 1000 cpm. For model 1, ART duration and ethambutol (ETB) use were significantly associated with VF. Models 2 and 3 did not differ from the whole cohort models respectively. In model 4, diarrhea, the current ART regimen, and fluconazole use were significantly associated with VF, whereas Adherence was not significant. In model 5, age, diarrhea, and fluconazole use were significant, whereas Adherence was not. When only participants with 12 months of ART were included in the analyses, model 1 was largely unchanged. For model 2, being recommended by a family member to receive HIV treatment, the absence of lipodystrophy, and symptoms of fatigue and diarrhea were no longer significantly associated with VF. In model 3, being employed was associated with VF. In model 4, the first clinic ART the participant received ART and the current regimen were associated with VF whereas fatigue and family recommendation for ART were not. Finally in model 5, fatigue and family recommendation for ART were not associated with VF.
Discussion
The RFVF study sought to define the individual-level determinants for VF which could be used in this setting to identify patients at risk and what their specific barriers are prior to ART initiation and while on treatment (Table 4). This would enable targeted approaches for interventions and could serve as surrogate measures for VF in settings where VL monitoring is not available. Most of the determinants found were consistent across a large number of models and subgroup analyses. Key demographic, socioeconomic, psychosocial, and clinical elements were associated with VF independent of adherence measures.
These factors do not include those that were identified as baseline risk factors.
Within the Demographic domain, younger age was a predictor of VF at baseline and had a trend towards being associated with VF when examining all variables but was not independent of Access or Adherence. This indicated that age impacts VF largely through obtaining and taking ARVs. Poor adherence and higher rates of VF for younger individuals have been described in many different settings. 27 –33 Additionally, male gender was associated with VF at baseline and in all other models confirming findings from previous studies. Not always dependent on adherence, these studies have shown men have poor health-seeking behaviors, higher baseline VL, lower ARV concentrations, late presentation with advanced disease, and inadequate retention in care, although women tend to have more ARV-related adverse events. 34 –39 From the Socioeconomic domain, relying on one's own vehicle for transportation to clinic had a trend towards an association with VF and appeared to be independent of the Access variable, which was unexpected based on previous reports. 9,40 It is likely that this variable is highly correlated with another significant factor such as male gender.
From the Psychosocial domain there were several novel variables identified. Symptoms consistent with depression and fatigue, as well as practicing unsafe sex, were markedly associated with VF in all models where those variables were examined independent of Access and Adherence. Depression has been linked to poor adherence but is also associated with other factors that could be independently associated with VF such as alcohol abuse, which was infrequent in this study. 41 –43 Unsafe sex may be a marker for behaviors leading to VF such as neglecting other health-related advice given during ART training and adherence counseling. It could also be more directly linked with VF through HIV superinfection or sexually transmitted infections that could cause an increase in VL. 44 Not being active with a religious faith and having at least one family member with HIV were associated with VF in all models but was not highly significant. Religious faith has been shown to improve adherence, but some studies have shown that certain practices could encourage prayer in lieu of ART. 45 –47 In contrast to other studies, stigma and traditional African medicine use was not specifically identified as a risk factor for VF. 9,48,49 Although having a family member with HIV could promote mutual support, if the family member is ill, time, attention and ARVs may be diverted away from the participant and to that family member. 50 Individuals who were pleased with their clinic experience were more likely to be controls in all models as has been shown in other studies that described the influence of the healthcare environment on clinic attendance and adherence. 9,40,51 –55 .
Several clinical factors were associated with VF. Low CD4 count at start of ART was highly associated with VF in all models and independent of Access or Adherence, confirming findings from previous studies. 56 It is important to note that, although a low CD4 count is highly associated with VF, it may be a consequence rather than a cause of VF. The absence of lipodystrophy was found to be a risk factor for VF but was not significant after controlling for adherence. This likely represents a strong correlation between ART adherence and fat redistribution syndrome, contrary to a previous report from Rwanda. 57 The use of d4T was also associated with VF at baseline when compared to TDF (most commonly used), ZDV, ABC, and ddI. The ART regimen only had a trend towards significance when more variables were included in the model. Side effects and toxicity-related treatment discontinuation may be more frequent for d4T compared to ZDV-containing ART. 58,59 Despite this finding, rates of overall virologic suppression were not statistically inferior when comparing d4T+3TC and ZDV+ddI with non-nucleoside reverse transcriptase inhibitor (NNRTI) 59 or indinavir-containing ART 60 in previous studies. TDF-containing regimens have been shown to be better tolerated and have fewer side effects than d4T-containing ART but comparably effective. 61,62 However, amongst participants failing a TDF-containing regimen, we and others reported a high rate of the K65R mutation (>65% 63 and 46%, 64 respectively). This finding is under surveillance to assess if this is a unique association in subtype C.
If a family member recommended the individual for ART, they were more likely to be a case in all models and independent of Access or Adherence. It is not entirely clear how family member referral could impact treatment outcomes. It is possible that family-driven stigma could be playing a role, but it is more likely that this represents a lack of connection to primary care services or access to ART such as is common for men in this setting. 65 This may alternatively reflect the fact that this is a proxy for more symptomatic disease at baseline prompting immediate family referral and subsequent association with poor outcomes. Finally, use of a television or radio to remind individuals to take their ARVs was suboptimal compared to using a mobile phone. Mobile phone reminders have been shown in clinical trials to promote adherence when weekly text messaging, daily calls, or alarms are used. 66 –68
Access and Adherence measures were highly correlated, ρ=0.68 (p<0.0001) (Fig. 2). Although poor Access (measured by the MPR) was significant in a UV comparison (≥70%), it was not significant in any of the MV models as a continuous measure. The MPR does identify major interruptions in ART, which is ideal for NNRTI-based therapy and was effective in this setting for identifying second-line VF, 69 but with the limitation in mind that it does not necessarily represent the proportion of days covered, which is a more accurate measure of adherence. Suboptimal Adherence (measured by pill count), however, was significantly associated with VF in all models where it was examined.
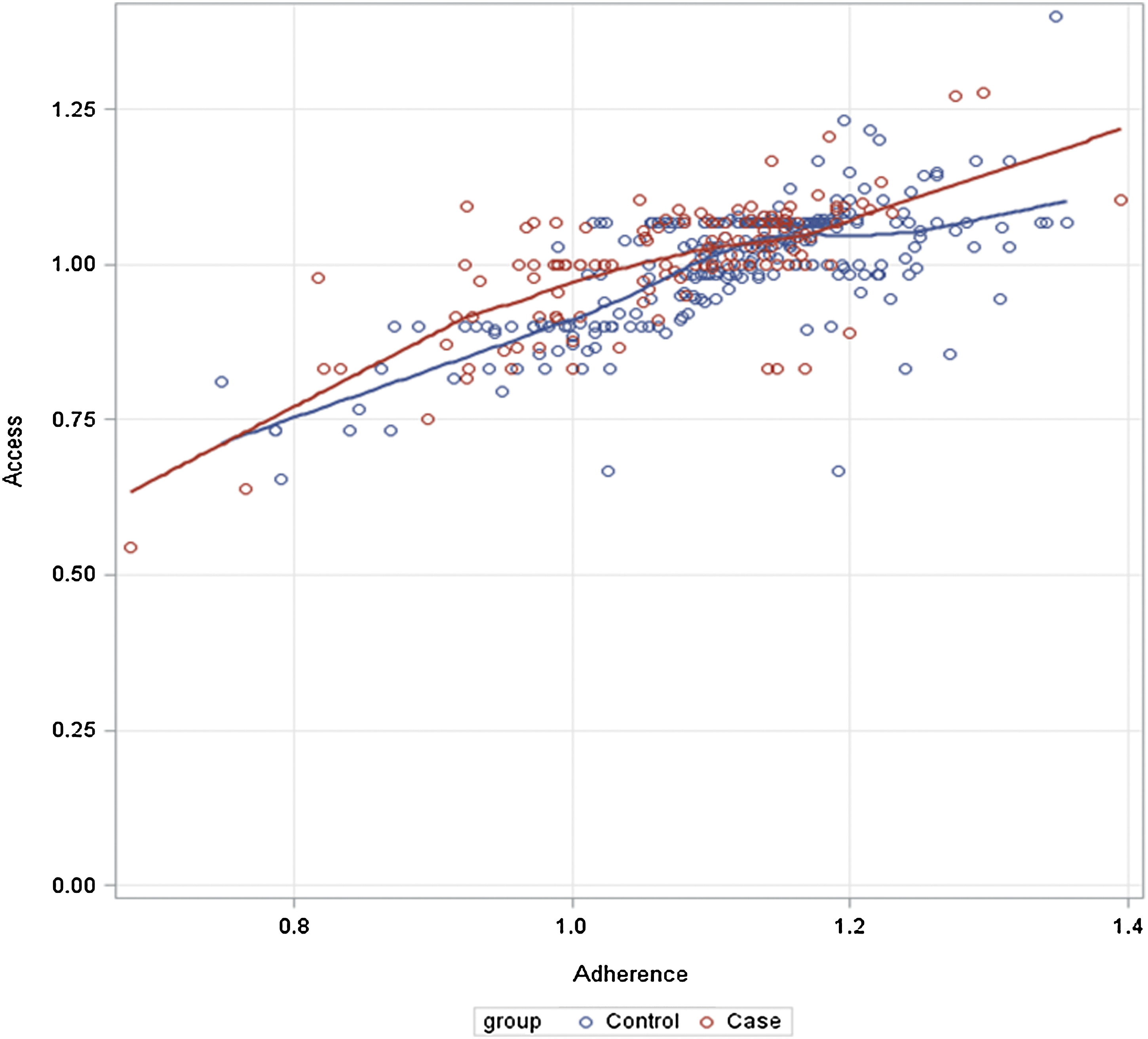
Correlation between Access and Adherence variables for cases and controls. (Color for this image can be found at
When a VL >50 cpm was used to define cases, only 35 participants were reclassified, indicating that the lower threshold identified only a small percentage of additional cases. A recent modeling study showed greater cost-effectiveness when using the higher VL threshold in this setting. 70 Using the lower cutoff, diarrhea and fluconazole use were associated with VF. While diarrhea could lead to diminished absorption, fluconazole increases ARV concentrations. Although this could lead to increased side effects and reduced ARV adherence, this association seems less plausible. When restricting the analyses to individuals with only 12 months of ART, fatigue and family members recommending ART were no longer associated with VF.
Ultimately these factors interact in highly complex ways in determining an individual's virologic response to ART (Fig. 3). Pill adherence is a necessary final step required for VL suppression (assuming optimal pharmacokinetics) and can be a reasonable surrogate for actual pills ingested, although pill dumping has been described in this setting, 71 as well as poor counting performance by clinical staff. Access to clinic refills as measured by the MPR is not always a reliable indicator of adherence, as it is not necessarily indicating ingested pills and individuals can obtain ARVs through other unmeasured sources. Although socioeconomic barriers have been well-described as leading to treatment interruptions, missed visits, and poor adherence, 8,72,73 these factors appear to be overshadowed by psychosocial and clinical factors in our study, reinforcing the importance of a comprehensive approach to assessing determinants of health. Socioeconomic and institutional barriers can often be more readily addressed with discrete interventions (transportation and food assistance or improving the clinic environment), 9 whereas psychosocial barriers can be more challenging to address.
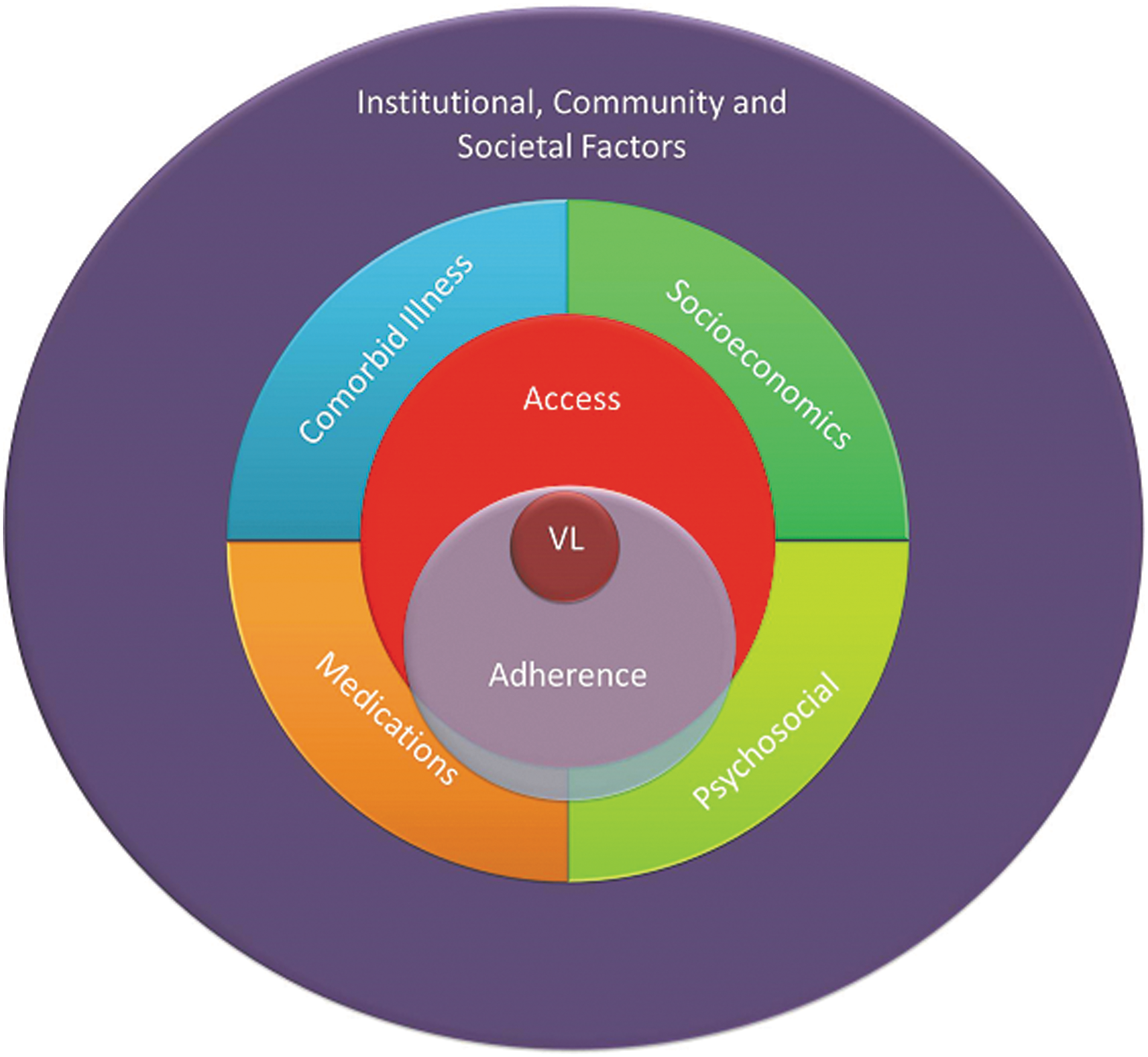
Schema of social, behavioral and clinical factors related to virologic response for individuals receiving antiretroviral therapy (ART). Pill adherence is necessary for viral load (VL) suppression; however, access to ART is neither necessary nor sufficient. Individuals can obtain ART from family or friends and may not swallow pills despite obtaining them. Socioeconomic factors (i.e., transportation to clinic) and co-morbid illnesses have a more direct effect on ART access. Likewise, concomitant medications and psychosocial factors (i.e., stigma, disclosure, and depression) are more directly associated with ART adherence but also impact ART access. Institutional (healthcare, religious, governmental), community (neighborhood, dyadic) and societal (cultural, infrastructure, policy) factors have more global impact at all lower levels in this paradigm. (Color for this image can be found at
There were limitations to the current study. The RFVF study used a case-control design and as such, recall bias is a possibility since many of the variables obtained from the questionnaire relied upon a participant's recollection of events that had occurred over the past 6 months. Moreover, causality has not been established through this analysis, and in fact, reverse causation may even exist. Despite this suggestion, we have identified surrogate markers that can be used by large programs to focus their counseling and monitoring efforts on those individuals at risk before VF or HIVDR occurs. Although most cases were told of their virologic status within a week or two prior to their interview, this could have impacted some of the responses about overall well-being. While we did not assess for HIVDR prior to ART initiation, which could be a risk factor for VF within the first 6 months of ART initiation, the rates of transmitted HIVDR have been reportedly low to non-existent in KwaZulu-Natal. 74 Furthermore, baseline HIV genotyping is not routinely available in South Africa and could therefore not be integrated into clinical algorithms at this time. Finally, only one clinical site was examined, which does not permit comparisons across diverse programs or geographic settings (rural or peri-urban).
In summary, the RFVF study provided real-world indicators which could be used to identify patients—either at the time of starting ART and or while receiving ART—for VF, an event with important long-term consequences. This would enable programs to tailor specific interventions for individuals with the intention to reduce the likelihood of VF and HIVDR. Furthermore, these determinants could be used in settings that do not have resources for routine VL monitoring to assist clinicians in making decisions about more targeted use of VL testing. It is important to validate this questionnaire in other urban as well as rural settings. Eventually a more refined questionnaire could be tested prospectively in order to develop a risk score.
Footnotes
Acknowledgments
We would like to express our deepest admiration and appreciation for the patients who participated in the study and the work of the Sinikithemba Clinic at McCord Hospital in Durban, South Africa for their commitment to improve patient care and support research. The tremendous contributions on the part of the counselors, medical records staff, nurses, and medical officers have been essential to the success of this study. Sabelo Dladla, Roma Maharaj, Kristy Nixon, Melisha Pertab, Sifiso Shange, and John Klopfer provided vital assistance for the data collection and analysis. A special thanks to Daniel and Alessandra Marconi for forbearance.
Author Disclosure Statement
D.R.K. is a consultant to, or has received research funding from Abbott, Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Merck, and Roche. For the remaining authors, none were declared.
Funding: Grant support from Emory University Center for AIDS Research (CFAR) (P30 AI050409) and the Emory School of Medicine Division of Infectious Diseases, NIH (P30 AI60354 to Harvard University CFAR and K24 RR16482 to D.R.K.), Harvard University Program on AIDS, CDC Cooperative Agreement (U62/CCU123541-01), Elizabeth Glaser Pediatric AIDS Foundation as part of Project HEART, Research and Health Sciences IT Division (UL1RR025008), and the Gilead Foundation.