
Abstract
This 10-year study (N=177) examines how people with HIV use spirituality to cope with life's trauma on top of HIV-related stress (e.g., facing death, stigma, poverty, limited healthcare) usual events. Spirituality, defined as a connection to a higher presence, is independent from religion (institutionalized spirituality). As a dynamic adaptive process, coping requires longitudinal studying. Qualitative content-analysis of interviews/essays yielded a coding of specific aspects and a longitudinal rating of overall spiritual coping. Most participants were rated as spiritual, using spiritual practices, about half experienced comfort, empowerment, growth/transformation, gratitude, less than one-third meaning, community, and positive reframing. Up to one-fifth perceived spiritual conflict, struggle, or anger, triggering post-traumatic stress, which sometimes converted into positive growth/transformation later. Over time, 65% used spiritual coping positively, 7% negatively, and 28% had no significant use. Spirituality was mainly beneficial for women, heterosexuals, and African Americans (p<0.05). Results suggest that spirituality is a major source of positive and occasionally negative coping (e.g., viewing HIV as sin). We discuss how clinicians can recognize and prevent when spirituality is creating distress and barriers to HIV treatment, adding a literature review on ways of effective spiritual assessment. Spirituality may be a beneficial component of coping with trauma, considering socio-cultural contexts.
Introduction
P
Pargament 2 has developed a transactional model of spiritual coping, defining spirituality as the search for the sacred, and religiousness as the search for the sacred within a religious denomination. 3 However, due to the moral stigma associated with HIV within many religious institutions, PLWH often consider themselves rather more spiritual than religious. 3 –5
Our own findings in PLWH 4 dovetail Pargament's research, 3 but emphasize the connection aspect of spirituality rather than the sacred component. In line with others, 6 –10 we define spirituality as the connection to a higher presence (e.g., within oneself, others, nature, or the transcendent), and religion as an organized, institutionalized spirituality. Thus, spirituality is a broader individualistic concept that includes people who reject organized religion. 6,8,9
The transactional model of stress and coping of Folkman and Lazarus 11 defines coping as a reduction of the discrepancy between the primary appraisal of the stressor and the secondary appraisal of one's ability to cope. The theoretical framework of the present study is based on our functional components model of coping, 12 which is similar to the transactional model but with an important added component. In addition to appraisals of the stressor and the self, a third appraisal involves the reaction to the stressor. Coping involves continuous formative evaluation of the three functional components, the stressor, the self, and the reaction. In other words, people react to stressful situations by adjusting their coping strategies, sometimes multiple times, until finding a strategy that works. For example, a gay man who prayed to God “to make him straight” finally became angry that his prayer remained unfulfilled. After developing his individual spiritual path, he came to terms with being gay. 4 This example illustrates that the dynamics of the three functional components of coping need to be viewed in a longitudinal context.
The main shortcoming of prior research was that most of the studies on spiritual coping were cross-sectional or of short duration. 12,13 For example, in people using spirituality to cope with trauma, a cross-sectional analysis may show a potentially spurious link between spiritual coping and depression. 14 Another common pitfall of cross-sectional research on coping is the stratification of aspects of coping strategies into adaptive and maladaptive. A cross-sectional snapshot does not provide us with information about the long-term consequences. As our prior research showed, spiritual struggle at the time of trauma was often a trigger of post-traumatic growth and positive spiritual transformation. 4,15 –18 Our longitudinal study has shown that a positive view of God 19 and an increase in spirituality after diagnosis 20 predicted significantly slower disease-progression (better preservation of CD4-cells and viral load decrease), 21 whereas a negative view of God predicted significantly faster disease progression over 4 years.
Traditionally, spiritual and cognitive coping have been subcategorized under emotion-focused coping. 12 Therefore, measurements of coping do not differentiate whether positive-reframing or meaning-making are based on spirituality or cognitions. 22 –24 However, we view spiritual coping, cognitive coping, and emotion focused coping as three distinct entities. 12 Spirituality is a broad construct, which may include cognitive, emotional, and behavioral aspects, and this spiritual coping may also involve concrete spiritual activities that are either cognitive or emotionally driven.
In line with others, 6 –10,25 we conceptualize spiritual coping as a focus on the connection to a higher presence that aids in meaning-making, positive reframing, self-empowerment, and growth/transformation on a personal and/or spiritual level. Ultimately, the use of spiritual coping can lead to spiritual transformation—a long-lasting profound change of one's behaviors, attitudes, beliefs (including spiritual beliefs), and self-views. 4,15 –18 Notably, spiritual coping can also be the “fork in the road” that turns life towards a negative path. 17
Consistent with Lazarus and Folkman, 11 our functional components model 12 emphasizes the importance of adapting one's coping style to the stressor—using problem-focused coping for changeable situations, and spiritual, cognitive, and emotion focused coping for unchangeable situations. For example, a woman survived before effective treatment became available because she firmly believed that God would heal her from HIV. However, her spiritual control belief became detrimental when she refused available effective treatment. Thus, the same coping strategy can have either positive or negative effects depending on the context.
The present study was informed by our literature review on spirituality and coping with HIV. 12,13 In a meta-analysis on effective ways of coping, Moskowitz 26 pointed out the need for qualitative research to focus on aspects that may not be covered in quantitative research.
This is the first study based on the functional components model of coping that examines spiritual coping longitudinally in a large sample with qualitative and quantitative methods. The primary aims of this study are to identify and quantify which specific aspects of spirituality are relevant for coping with trauma in PLWH and to develop a longitudinal measurement of the effect, use, and dynamics of spiritual coping. A secondary aim is to identify socio-demographic factors predisposing one to use spiritual coping with a positive effect. The overall goal is to discuss the implications for PLWH, as well as healthcare workers, so they may help guide PLWH to find their best possible path to cope with trauma.
Methods
In our longitudinal study, we have followed 177 people with HIV for up to 10 years to examine psychosocial and spiritual factors related to health. 19 –21 In this secondary data analysis, we use a mixed method approach, applying qualitative techniques to examine aspects of spiritual coping and to develop an overall rating of spiritual coping. Quantitative variables were then derived from frequencies of these codes and ratings.
Study population and sampling
At entry, between 1997–2000, the study selected people in the mid-range of HIV disease (150–500 CD4-cells/mm3, CD4-nadir >75 cells/mm, no prior AIDS-defining symptoms). People with dementia, active substance use disorder, and/or psychosis (based on the SCID, DSM-III-R) were excluded. Participants were recruited via flyers (distributed through doctors' offices, community events, support groups, HIV organizations), newspaper ads, and word of mouth.
Procedures
The study was IRB approved; all participants gave informed consent and received $50 compensation. Our interviewers contacted the participants every 3 months by phone and scheduled them every 6 months for office visits. Either Dr. Ironson (P.I.) or a master-level mental health staff conducted the interview. We made efforts to maintain continuity of the interviewer, three of them employed between 9–14 years.
We collected in-depth interviews and essays in 6-month intervals, asking participants how they cope with HIV and traumatic events as they occur. At the initial and every follow-up interview, we explored HIV disclosure (and sexual orientation) and how the reaction to the disclosure was. We further asked how their life changed since the diagnosis; how they spent their daily life; which activities they looked forward to; if they had a partner, and if they were sexually active and practiced safer sex; if and how their partners were helpful to them, if they had someone to take care of them if needed and to share their deepest feelings with; and if they had partners or friends who died from AIDS and how they coped.
Other questions tapped into their spiritual and afterlife beliefs, estimated life expectancy, and healthcare information—we asked how they found their physician and if they were satisfied with their medical care; what they were doing to keep themselves healthy; what percentage of their well-being was due to their own attitudes and behaviors vs. medical care; if they were getting complementary or alternative treatment; and if they were taking prescribed medication and the reason behind it.
Finally, we asked about what enabled them to keep going in the face of HIV and if anything positive had resulted from being HIV-positive or anything else was relevant to maintaining their health in the face of HIV. In addition, interviews and essays captured how they coped with the most difficult life event over the past 6 months.
On the life-event scale (from −3 to +3), 27,28 participants rated the stress of events that had happened to them in the past 6 months. They also wrote a “trauma” essay, which asked participants to describe the most stressful event that had happened to them in the past 6 months, including their deepest thoughts and feelings. To transcribe the most relevant interview/essay, we chose a time-point with the highest distress rating (closest to −3, very stressful) during the first 3-year period of the longitudinal study (1997 to 2000). Besides this interview/essay, a team of ten trained transcribers summarized the content of all other interviews and essays for up to 10 years.
All transcripts were quality controlled and entered in the qualitative software ATLAS.ti® and rated using directed qualitative content analysis, 29–31 an empirical reliability controlled analysis of texts that allows both qualitative and quantitative operations. This method allowed us to develop a coding agenda for aspects of spiritual coping and to develop an overall rating of spiritual coping over time.
Qualitative content analysis
After completion of a transcript, the transcriber worked with the research team inductively line by line through the entire text to capture quotes and anchor examples for the coding of aspects and the overall rating of spiritual coping. At a point of saturation (after more than 70 interviews), we compiled tentative coding and rating definitions and anchor examples. Analyzing 20 interviews, ten raters established independent inter-rater reliability. For each Cronbach's alpha <0.80, definitions were revised. Next, chance-corrected inter-rater reliability of two raters was established for 20 further interviews. The definitions were fine-tuned until reliability of the coding was substantial (Cohen's Kappa above 0.60), and reliability of the overall spiritual coping rating was excellent (Kendall's tau B=0.81, p<0.001). Finally, two raters analyzed all 177 transcripts independently. Each rater provided quotes for each coded spiritual strategy and gave an overall rating of longitudinal spiritual coping. Any discrepancies on codings or ratings were either consensually agreed or discussed in the team. 32 For the rating, any discrepancies >1 were quality controlled by another rater-couple, again coding independently and reviewing discrepancies consensually. In one case, there was not enough information to rate overall longitudinal spiritual coping reliably.
Statistical analysis
All qualitative data were aggregated and transferred into SPSS® version 19 for further statistical analysis. Descriptive statistics and group comparisons (ANOVA and Chi-square tests) were used to depict the frequencies and socio-demographic associations of spiritual coping.
Results
We summarized the codes, definitions, and examples of specific aspects of spiritual coping in Table 1, the longitudinal rating of spiritual coping in Table 2, and the respective frequencies in Figs. 1 and 2.
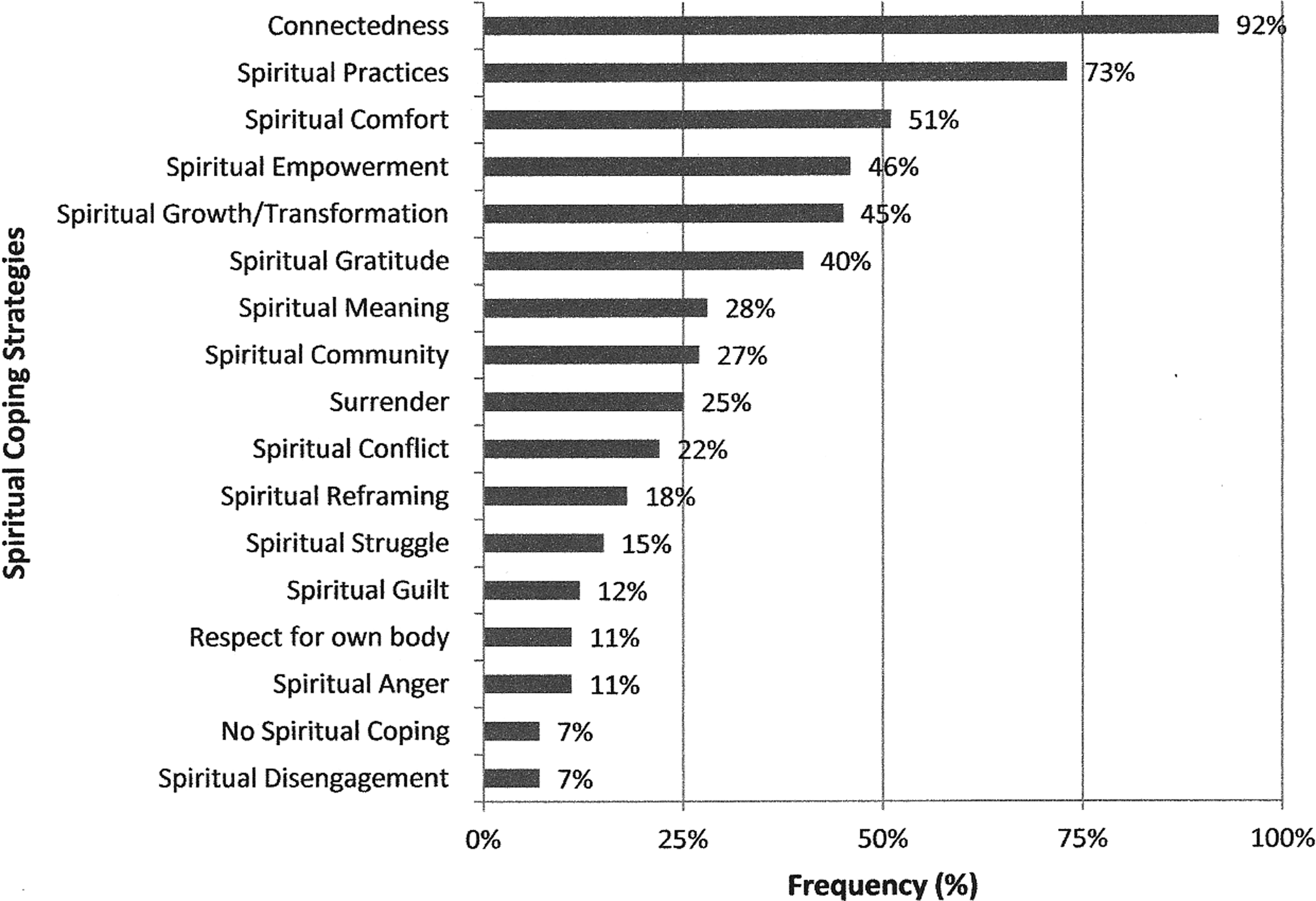
Specific aspects of spiritual coping (% frequency).
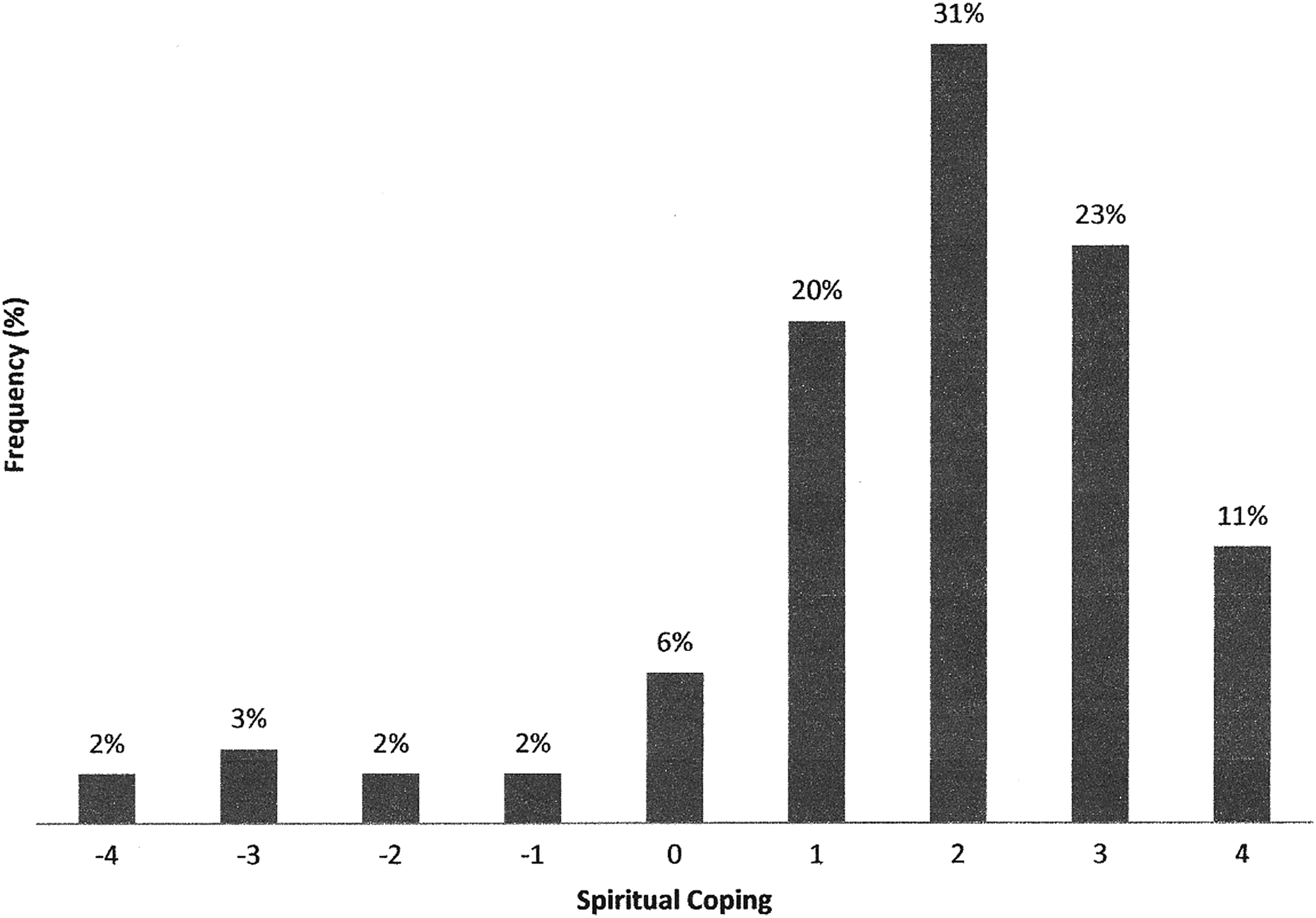
Longitudinal rating of spiritual coping (frequencies in %). Spiritual coping is coded on a 9-point scale (see Table 2). The longitudinal use and effect of spiritual coping can be grouped into three categories: Use with negative effects (from −4 to −2), no significant use/effect (from −1 to +1), and use with positive effects (from +2 to +4).
Socio-demographics
The sample was diverse with respect to gender (30% female), ethnicity (36% African American, 31% White (non-Latino), 28% Latino), sexual orientation (45% heterosexual), and education (77% high-school or less, 19% college graduates). Most participants were relatively poor (modal annual income $10,000), which is consistent with high unemployment (15%) and disability (42%). About half (52%) did not attend religious services, 23% less than weekly, and 25% at least weekly.
Stressful life events
Within the first 3 years, 118 of 177 participants reported a very stressful event such as death of a loved one and/or divorce, or another comparably stressful life event.
Specific aspects of spiritual coping
According to our coding, most participants were spiritual (92%) and used spiritual practices (73%), whether the connection to a higher presence was found via “praying to God” or “feeling one with a mountain”. Spiritual comfort (51%), empowerment (46%), growth/transformation (45%), and gratitude (40%) were frequent positive aspects of spirituality. However, spirituality was less involved in the many ways of meaning-making (28%), positive reframing (18%), and community support (27%). Surrender (25%) was a double-edged sword, since the belief that “God is in control” could result in both overcoming substance use and not taking HIV medication.
The dynamics of spiritual coping were also illustrated by less common aspects, such as conflict (22%), struggle (15%), guilt (12%), anger (11%), and disengagement (7%). A critical confrontation with spirituality could catalyze both a spiral of negative effects and a positive transformation via an increase in spirituality.
Longitudinal rating of spiritual coping
The longitudinal rating of spiritual coping showed that each spiritual aspect can have both a positive and a negative effect on coping depending on the context. Spiritual practices do not always have positive effects as demonstrated in the introductory example of the gay man praying to God to make him straight and the woman not taking her medication because she felt her prayers had healed her from HIV. The rating of spiritual coping takes into account the overall longitudinal effect of all aspects of spiritual coping. Over time, spiritual coping is a dynamic multidimensional construct that reflects more than the sum of specific aspects and cannot be investigated by looking at one traumatic event only. Table 2 explains our longitudinal rating of spiritual coping with definitions and examples. Although the scale ranks from −4 to +4, indicating the overall negative and positive effects, the rating is not a mere linear function. The multidimensional construct of spiritual coping combines the use, the effect, and the dynamics of spiritual coping. The use of spiritual coping behaves more like a curve, with zero being the nadir (no spiritual connection and no effect) and the maxima (±4) reflecting extreme use of spiritual coping with positive/negative effects.
For example, a continuous spiritual seeker who feels lost in life and attempts suicide is categorized as −4, whereas a spiritual experience triggering a positive transformation is rated as +4. Persistent struggle with unquestioned spiritual beliefs (e.g., karma, hell) (−3) is opposed to post-traumatic spiritual growth/transformation (+3). Ambivalent spiritual coping with fluctuating effects is categorized as −2, whereas finding benefit in consistent spiritual practices is categorized as +2. Feeling guilty about not having a spiritual connection was rated as −1 and the absence of elaborate use or any effect of spiritual coping as +1.
In addition, the longitudinal rating took into account that use and effect of spiritual coping may fluctuate over time. Rating longitudinally captures whether spiritual disengagement at the time of trauma converts into future effective spiritual coping. Intense trauma often triggers dynamics and reexamination of one's spirituality. Static spirituality is more prevalent in those who do not critically reflect or elaborate on their spirituality.
In our study, some participants experienced spirituality as a central driving force that influences the person's life. Participants who rated +4 on the scale of the Longitudinal Rating of Spiritual Coping (Table 2) found ways to use spirituality to benefit them, such as complete surrender to God's will or a higher being. For instance, in one interview, the participant related how she has faced extreme adversity in her life—imprisonment, battling with drug addictions, having a low socioeconomic status, and other numerous family stressors, including death of a loved one to AIDS. However, all these stressors became manageable to her since she had started to use spirituality to cope. She stated that HIV had “opened her eyes” and this transformation had led her to becoming a Christian. The participant displayed spiritual surrender with respect to her HIV infection and believed that God will heal her and she could “live up to 101 years of age.” Furthermore, she admits: “The medicine made me real sick, I lost my hair, weight, and was very depressed. And these are only some of the side effects. So I'm leaving it in the hands of the Lord.” The participant recalled that the death of a friend had profoundly impacted her life. She continued by stating: “It changed my life, the way I was living. The drugs, alcohol, fornication with married men, all that stopped” and it made her grow more religious. She even attributed this event to “saving” her and God blessing her with two more children. She also described spiritual experiences, such as feelings of exaltation—she feels higher, she feels like she's “moving up” and “when the spirit comes upon me, I feel it.” She further relates that she has received HIV from “doing drugs; not as punishment (…), just something I had to go through in this life because we all have to go through something. It led me to God.” This participant, faced with multiple hurdles in her life, has put her life into God's hands.
Physicians' lack of awareness of negative spiritual coping
On the other pole, in some cases, spiritual coping had a long-lasting negative effect and became at times even a stressor in itself. Participants who rated −4 on the Longitudinal Rating of Spiritual Coping scale, experienced anger towards spiritual presence, and feelings of punishment. Overall, they have very negative life experiences, yet hold spiritual presence accountable for their life. Surrender may be present, but if so, it is used in a negative way (as an avoidance strategy). For instance, in one case, a participant who grew up as a Baptist identified himself as religious up until he was diagnosed with HIV, but he began to lose his faith afterwards. He testified, “The longer this has happened, the more empty I have become spiritually or religiously, (…) I feel like I don't have a soul right now. My life, my entire world has turned upside down (…) drinking a lot, you know…angry, violent; (…) I just continued an abusive path.” The “worst” for his spiritual turnaround is that his disconnectedness from God had impaired his son from forming a relationship with God. This participant had been struggling to re-engage into the church community. Importantly, participants who experienced negative effects of spiritual coping did not talk to their physicians about their struggle and were not asked by their physicians how they used their spirituality to cope.
Frequency and socio-demographic aspects of longitudinal spiritual coping
As shown in Fig. 2, 65% used spirituality with a positive effect over time to cope with trauma (spiritual coping >1), no effect (between±1) was prevalent in 28%, whereas only 7% had negative effects (<−1). Mean spiritual coping differed by gender (F=9.72, df 1,174, p=0.002), sexual orientation (F=6.98, df 1,172, p=0.009), and ethnicity (F=5.48, df 1,174, p = −0.020) (Fig. 3).Specifically, positive effective spiritual coping (>1) occurred more frequently among female (83% vs. 57%, LR=11.58, p=0.001), heterosexual (77% vs. 55 %, LR=8.94, p<0.003), and African American participants (77% vs. 51%, LR=7.88, p=0.009). No effect of spiritual coping (0) was more prevalent among Whites compared to other ethnicities (12% vs. 3%, LR=4.30, p=0.038).

Socio-demographic differences in longitudinal spiritual coping. Mean scores of longitudinal rating of spiritual coping (scale range −4 to +4) stratified by gender, sexual orientation, and ethnicity.
Discussion
The purpose of this study was to examine longitudinally how effective PLWH use their spirituality to cope with trauma to help guide PLWH so they may recognize how to use spirituality for effectively coping with traumatic events. In our study population, almost all PLWH were spiritual in the sense of feeling connected to a higher presence and used their spirituality to cope with trauma, which is consistent with the findings from Cotton et al. 33 In line with other studies in PLWH, 34 –36 spirituality was particularly beneficial for women, heterosexuals, and African Americans, whereas Non-Latino Whites made less use of spiritual coping. For the majority, spiritual coping was positively effective over time, which is also supported by other studies. 37 –40
In particular, religious stigma often prevented participants from being open about their HIV status, which dovetails the results of another qualitative study on African American gay men, experiencing religious homophobia. 41 Spirituality, as part of the problem, is a known phenomenon in coping research, 25,42 which was found to be associated with negative health outcomes in longitudinal studies in people with HIV. 19,43
What this study identified is that spiritual coping fluctuates over time, and that spiritual coping is more than the sum of single spiritual aspects and needs to be seen in a longitudinal context within the dynamics of the three functional components of coping (stressor, self, reaction). For some participants in our study, the initial reaction to a stressor is spiritual struggle, conflict or anger (which Pargament classifies as “negative spiritual coping”). 44 However, this paved the way for post-traumatic spiritual growth/transformation. Spirituality is mainly helpful as a source of comfort, empowerment, growth/transformation, gratitude, and community support, as described by others. 9,45 Spirituality is an aid on its own for meaning-making and positive reframing, beyond cognitions.
The results of this study have important implications for health care. Although clinicians are often afraid to address the “Gretchen Question” which means to ask directly about spirituality, 46 this question is often already the intervention to help coping with trauma. 47 The spiritual coding and rating in our study is based on brief interview questions that are recommended by Pargament 25 and King and Koenig 8 to tap into the topic of spirituality and coping. Taking the 2–5 min to ask these questions may be an effective way to signal genuine care about illness, stigma, and trauma. 47
Taking the time to assess spirituality in PLWH may save time and life in the long run and may have far-reaching clinical implications. Most PLWH do not share with their clinicians when they do not take the prescribed HIV treatment as required if they did not feel comfortable to talk about spirituality with their clinicians, which negatively impacts their life expectancy. 48 –50 For example, if spiritual struggle is present, taking a spiritual assessment may help with resolution. 42,47,51 Opening the dialog about spiritual struggle, conflict, guilt, anger, and disengagement may prevent PLWH from a negative spiral of spiritual reactions or even initiate an individual's critical confrontation with negative religious beliefs such as karma or hell. Conversely, when spirituality is a source of meaning and growth and important in medical decision making, PLWH are often comforted by sharing beliefs with their clinician. 15 –18,48 –50,52 This is why clinicians should not defer the spiritual assessment to others, although providing spiritual interventions is best left to experts in spiritual care. 47 Koenig et al. 47 dovetails our own experience that we as clinicians benefit too from bringing spirituality back to medicine by experiencing both greater work and patient satisfaction. 4,53
In US surveys, 54,55 about 90% of the patients but only one-third of the clinicians agreed that clinicians should ask about spirituality, whereas fewer than 10% of clinicians actually do so. 56 The present study and our prior research in PLWH provide evidence that overcoming the barrier to address spirituality is beneficial for several reasons. First, as shown in this study, most PLWH use their spirituality to cope with trauma. Second, an increase in spirituality after diagnosis 20 and a positive view of God 19 predict slower disease progression and spiritual transformation is associated with longer survival. 18 Third, spirituality plays a role in medical decision-making, adherence, quality of life, and clinician–patient relationship. 12,15,16,18,48 –50,52 Finally, it is important to assess the spiritual needs in order to identify people who may benefit from spiritual intervention. Potentially, spirituality-based interventions may aid in trauma treatment, as some experimental studies suggest. 57 –59
As Pargament 60 points out, the critical question is not if but how spirituality should be assessed in the clinical setting. Before addressing the topic of spirituality, clinicians need to establish a relationship in which people feel comfortable to open up about their spirituality. 53 If someone indicates that spirituality is not important to her/him, there is probably no need for further questions. 61 However, it might be that this individual has problems with spirituality that may not be uncovered, when not asked for. Nevertheless, tackling spirituality in those who do not feel spiritually connected, which is more common in White gay men, may negatively affect the relationship to the individual. Vigilance is required not to offend one's spiritual belief system. 25,61,62
In PLWH who are spiritually engaged, the dynamics of spiritual coping deserve special attention. In coping with trauma, spirituality may change over time from being a useful resource to being ineffective or even harmful. 63 Clinicians can encourage the process of formative evaluation of the effectiveness of the individual's coping style. This study further corroborates our prior findings: those who are more spiritually engaged are more likely to reap the positive benefits of spirituality but are also at higher risk of negative effects of spirituality.
The three major limitations of this study include a cohort effect, sample bias, and interviewer bias. The cohort effect occurred through PLWH who died or did not feel well enough to visit our study site, which may have produced a bias towards positive spiritual coping, although participants would have received a rating based on initial participation in the study. In addition, this study initially excluded people with substance use dependence, dementia, active psychosis, and people who could not speak English. Thus, frequencies in this study are not representative for the population of PLWH in South Florida and may not be generalizable to other cultural contexts.
Spiritual coping can be reliably assessed in the clinical setting following the questions recommended by King and Koenig 8 and Pargament 25 and by using our rating scale. It is hoped that this longitudinal examination of spiritual coping in PLWH will provide useful information to guide people dealing with traumatic events based on spiritual coping. For the majority of our participants, spirituality is an effective and useful tool to cope with trauma. Even initial spiritual struggle can catalyze effective spiritual coping long-term. However, those who are engaged in spiritual struggle are at particular risk for experiencing harmful effects. Therefore, it is important for clinicians to know how to integrate spirituality constructively into trauma-treatment. Clinicians can encourage the critical evaluation of adaptive use of spiritual coping.
Our future longitudinal analysis will examine whether spiritual coping is associated with healthier behavior, better health, and longer survival with HIV [Kremer H, Ironson G, Kaplan L, et al. (under submission) Spiritual Coping Predicts HIV Disease Progression and Transmission over Four Years. AIDS Care].
Footnotes
Acknowledgments
We thank the Templeton Foundation for the 2-year funding of this secondary data analysis and the NIH (R01MH53791 and R01MH066697, PI: Gail Ironson) and the Metanexus Foundation for financing the longitudinal study. Further, we thank all people living with HIV for sharing their personal experiences with us. Finally, we thank the positive survivors research team for running the longitudinal study, in particular, Annie George for conducting most of the interviews, the research assistants Tony Guerra and Marietta Suarez, Franz Lutz for his suggestion to create a Wiki for the coding agenda, and all the students for their enormous help in transcribing and coding of the interviews and essays.
Author Disclosure Statement
No competing financial interests exist.