
Abstract
Metabolic syndrome (MS), a group of interrelated risk factors for cardiovascular diseases (CVD) and type 2 diabetes, has been increasingly reported among HIV-infected patients. Data on the prevalence and risk factors for MS among HIV-1 infected Thai adults are limited. The study collected cross-sectional data from 580 HIV-1 infected adults—46.2% were men and 71% were antiretroviral therapy (ART)-experienced. The majority (78.8%) of them used non-nucleoside reverse transcriptase inhibitor-based regimens. Data on lipid profiles, fasting blood glucose, CD4 count, HIV RNA, antiretroviral therapy (ART), anthropometry, food intake, and exercise were recorded. MS was defined using American Heart Association/National Heart Lung and Blood Institute criteria. Overall prevalence of MS was 22.2%; 15.9% in ART-naïve group vs. 24.9% in ART-experienced group, p = 0.018. Significant risk factors for MS in multivariate analyses included age ≥35 years (odds ratio, OR, 4.2, 95%CI 1.6–11.0, p = 0.004), high cholesterol (OR 4.7, 95%CI 1.7–12.9, p = 0.002), and living outside Bangkok (OR 4.2, 95%CI 1.6–10.8, p = 0.003) in the ART-naïve group, and female gender (OR 1.7, 95%CI 1.0–2.8, p = 0.05), lipodystrophy (OR 1.8, 95%CI 1.0–3.0, p = 0.032), high cholesterol (OR 1.9, 95%CI 1.1–3.1, p = 0.015), and food insecurity (OR 1.8, 95%CI 1.0–3.3, p = 0.05) in the ART-experienced group. All variables, except for female gender in the ART-experienced group, remained significantly associated with MS in a model where lipodystrophy was excluded. We concluded that MS was common among HIV-1–infected Thai adults. As HIV-infected patients get older, early screening and intervention, such as ART modification to avoid lipodystrophy, may reduce MS and CVD-related morbidities and mortalities in long-term care.
Introduction
A
Metabolic syndrome (MS) is a set of clinical and laboratory parameters known to be highly related to the development of CVD and type 2 diabetes. Several factors such as socio-economic status, 8 dietary intake, 9 food insecurity, 10,11 ART, 6,7 lipodystrophy, 12,13 and physical activity level 14 –16 have been described as contributing to MS in HIV infection. There are several definitions of MS such as that of the International Diabetes Federation (IDF), 17 the National Cholesterol Education Program's Adult Treatment Panel III (NCEP ATP III), 18 the World Health Organization (WHO), 19 and the National Heart Lung and Blood Institute and American Heart Association (NHLBI and AHA). 20
Data on the prevalence and risk factors of MS in Asian HIV-infected patients are very limited. We examined the prevalence of MS and its related factors among ART-naïve and ART-experienced HIV-1 infected adult patients in Thailand. We used the NHLBI and AHA MS definitions as they have waist-circumference criteria which are adjusted by ethnic groups. MS is defined as having ≥3 of the following 5 components: abdominal obesity, hypertriglyceridemia, low HDL, high blood pressure, and high fasting plasma glucose. 20
Methods
Enrollment of study participants
The study was conducted in six HIV clinics located in five different regions of Thailand; the Thai Red Cross Anonymous Clinic in Bangkok (Central Thailand), Bamrasnaradura Infectious Disease Institute in Nonthaburi (Central Thailand), Queen Savang Vadhana Memorial Hospital in Chonburi (Eastern Thailand), Sanpatong Hospital in Chiang Mai (Northern Thailand), Khonkaen Provincial Hospital in Khonkaen (Northeastern Thailand), and Surat Thani Provincial Hospital (Southern Thailand) between August 2009 and December 2011.
All HIV-1-infected patients, aged >18 years, who were attending the services at these clinics, were consecutively invited to participate in this study. Patients were excluded from the study if they had an active, AIDS-related illness within 3 months before participating in the study or if they were pregnant. Informed consent was obtained from all study participants. The study was approved by the Institutional Review Boards (IRBs) of each participating hospital as well as the IRBs of the Faculty of Medicine, Chulalongkorn University, and the Ministry of Public Health of Thailand.
Clinical and laboratory assessments
Anthropometry measurement was done by centrally trained healthcare workers (nurses and nutritionists) at each clinic. The measurements included weight, height, umbilical waist circumference, waist/hip ratio, and mid-upper arm circumference. Data on fasting plasma glucose, triglyceride, total cholesterol, HDL, calculated low-density lipoprotein cholesterol (LDL), CD4 count, HIV RNA, and complete blood count (CBC) performed at the enrollment or within 3 months prior to enrollment were collected.
The term lipodystrophy used in this study included lipoatrophy and/or lipohypertrophy. Lipoatrophy was defined as subcutaneous fat loss of face, arms, and legs. Lipohypertrophy was defined as fat accumulation at dorso-cervical spine, abdomen, and breast. Lipodystrophy was documented by participant self-recognition and/or observation made by healthcare workers. The degree of lipodystrophy at each body compartment was graded according to the lipodystrophy severity grading scale (LSGS), proposed by Lichtenstein et al., 21 as absent (score of 0), mild (noticeable on close inspection, score of (1), moderate (readily noticeable by patient/physician, score of (2), or severe (readily noticeable to a casual observer, score of (3). The Lipodystrophy scores were categorized as absent (score <0), grade 1 (0–9.9), grade 2 (10–14.9), grade 3 (15–22.9), and grade 4 (≥23). 21
Dietary intakes were assessed in terms of total energy from macro and micro nutrients using 24-h recall. The questionnaire consists of questions on demographics, health status, ART, food budget, food insecurity and accessibility, food hygiene, dietary intakes (Usual Food Intakes: UFI), HIV nutritional knowledge, smoking, drug and alcohol use was modified from the Health and Lifestyle Survey in Australia, based on the results from the pilot testing and focus group discussions among Thai HIV-infected patients. 22,23
Participants were asked to rate their physical activity as low, moderate, or high using the International Physical Activity Questionnaire (IPAQ) short form (Thai version, 2005) published by Division of Physical Activity and Health, Department of Health, Ministry of Public Health of Thailand). 24,25 Information regarding family history of chronic diseases and family support was also collected through an interview.
MS was defined, using the AHA and NHLBI criteria, as having three or more of the following five components: abdominal obesity (waist circumference ≥90 cm for men, ≥80 cm for women), hypertriglyceridemia (≥150 mg/dL), low HDL (men <40 mg/dL, women <50 mg/dL), high blood pressure (≥130/85 mmHg), and high fasting plasma glucose (FPG ≥100 mg/dL). 20
Statistical analysis
Prevalence rates of MS and each MS component were calculated along with 95% confidence intervals (CI) for ART-naïve and ART-experienced participants. Student t-test or Mann Whitney U-test was performed to compare continuous variables for normally and non-normally distributed variables, respectively. Associations of MS with demographic characteristics, HIV parameters, lipodystrophy, fat accumulation, and the presence of metabolic abnormalities were analyzed using a univariate analysis by logistic regression. Factors associated with MS in univariate analysis with p values<0.1 were included in the multivariate model by backward stepwise selection method. Likelihood ratio test statistic was used to assess overall model fit. As lipodystrophy might include lipohypertrophy, which may be the same phenotype with metabolic syndrome, a model excluding lipodystrophy was also analyzed. All statistical analyses were performed using Stata version 11 (StataCorp LP, College Station, TX, USA).
Results
A total of 584 HIV-infected patients were enrolled into the study. Two participants were excluded because their HIV status was later found to be negative, and another two participants withdrew after the enrollment resulting in 580 HIV-infected participants in the analysis.
Characteristics of study participants
Of 580 HIV-infected participants included for data analyses, 46.2% were men and 53.8% were women. Mean age was 37 years (interquartile range, IQR, 32–43) and mean duration of HIV infection was 5.0 years (IQR 2.0–9.0). Thymidine analogues and non-nucleoside reverse transcriptase inhibitor (NNRTI) were generally used by the majority of HIV-infected patients in Thailand during the time period of the study. Among 410 (71%) ART-experienced participants, 92.4% had past or current use of the following nucleoside/nucleotide reverse transcriptase inhibitors (NRTI): lamivudine (89.8%), stavudine (68.0%), zidovudine (52.7%), tenofovir (24.6%), didanosine (7.3%), and abacavir (0.2%). NNRTIs were ever used in 78.8% (72.2% ever used nevirapine and 34.9% ever used efavirenz). Past or current protease inhibitor (PI) use was reported by 14.9% (8.3% ever used indinavir/ritonavir, 6.8% ever used lopinavir/ritonavir, and 1.5% ever used atazanavir/ritonavir). Median duration on ART was 2.6 years (IQR 1.8–5.0) for NNRTI-based regimens and 2.0 years (IQR 0.6–5.2) for PI-based regimens. Mean CD4 count was 394 cells/mm3 (IQR 267–535). HIV RNA was <400 copies/mL in 68.3% of participants; 10.6% in ART-naïve group and 92.2% in ART-experienced group.
Compared to ART-naïve participants, ART-experienced participants were significantly more likely to be male, at older age, infected with HIV for a longer duration, more clinically advanced, having lower HIV RNA, and having lipodystrophy (Table 1). In addition, significantly higher proportion of ART-experienced participants had a high waist to hip ratio (>0.9 for men, >0.8 for women) although lower proportion of them had obesity defined by body mass index (BMI) >25 kg/m2 and large mid-upper arm circumference (Table 2).
Chi-square test was performed for test of homogeneity for categorical variables, p value of<0.05 was considered to be statistically significance.
ART, antiretroviral therapy; CDC, Center for Disease Control and Prevention; CVD, cardiovascular disease; IQR, interquartile range; NNRTI, non-nucleoside/nucleotide reverse transcriptase inhibitor; PI, protease inhibitor; USD, United States Dollar.
Chi-square test was performed for test of homogeneity for categorical variables, p value of≤0.05 denotes level of significance.
ART, antiretroviral therapy; BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein cholesterol; IQR, interquartile range; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
Prevalence of hypertriglyceridemia, hypercholesterolemia, high LDL, and hyperglycemia was also significantly higher in ART-experienced participants compared to ART-naive participants, although HDL was higher in ART-experienced participants (Table 2). Dietary intake was not significantly different between ART-experienced and ART-naive groups (data not shown).
Participants from Eastern Thailand demonstrated lower nutrition knowledge (38.6% with adequate knowledge vs. 55.9% in other regions) and engaged in significantly less exercise (33.4% with moderate to high exercise levels vs. 50.3% in other regions) when compared with participants from the other regions. Food insecurity and level of stress did not differ among regions (data not shown). There was no differences in any of these factors comparing ART-naïve group and ART–experienced group.
Prevalence of metabolic syndrome
The overall prevalence of MS among all participants was 22.2%. MS prevalence was significantly higher in ART-experienced group than ART-naïve group (24.9% vs. 15.9%, p=0.018). HIV-infected women had higher MS prevalence than HIV-infected men (17.9% vs. 26.0%, p=0.02). MS prevalence was increasing by age among both HIV-infected women and men (Fig. 1).
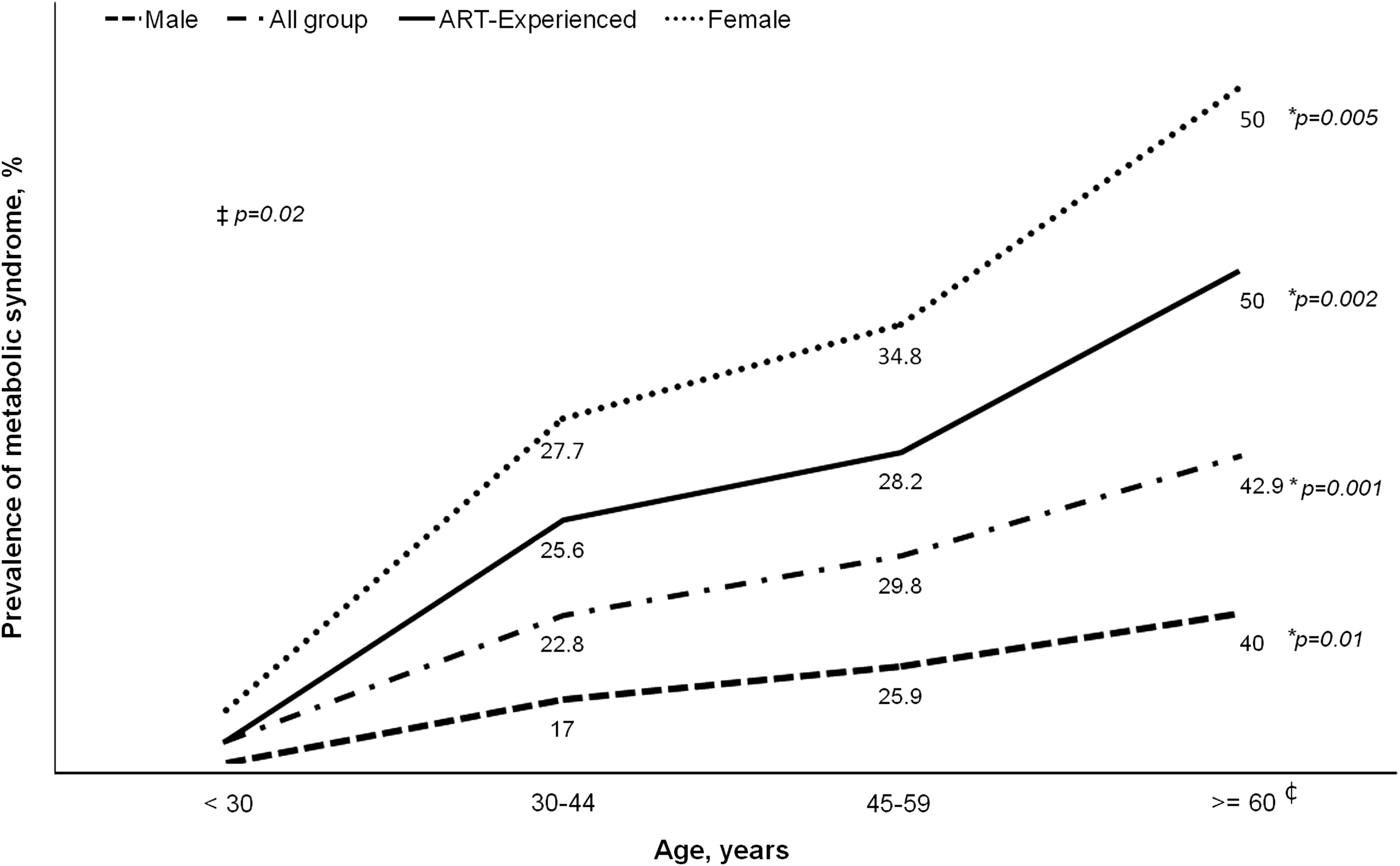
Prevalence of metabolic syndrome among 580 HIV-infected participants in Thailand by gender, age, gender, ART status, and age group. *p value for trend for each group; ‡p value comparing female and male groups; ¢Only 7 participants were in this group.
Over half of the study population was found to have at least two components of MS, 58.8% among ART-experienced group and 47.1% among ART-naïve group (p=0.010). For each component of MS, high waist circumference was found in 15.3% of men and 42.9% of women, low HDL in 48.9%, hypertriglyceridemia in 41.2%, high blood pressure in 26.2%, and hyperglycemia in 20.7% of all participants (Table 2).
Hyperglycemia and hypertriglyceridemia were the two components of MS that were significantly more common in ART-experienced than ART-naïve group, while low HDL was more common among ART-naïve group (Table 2 and Fig. 2).
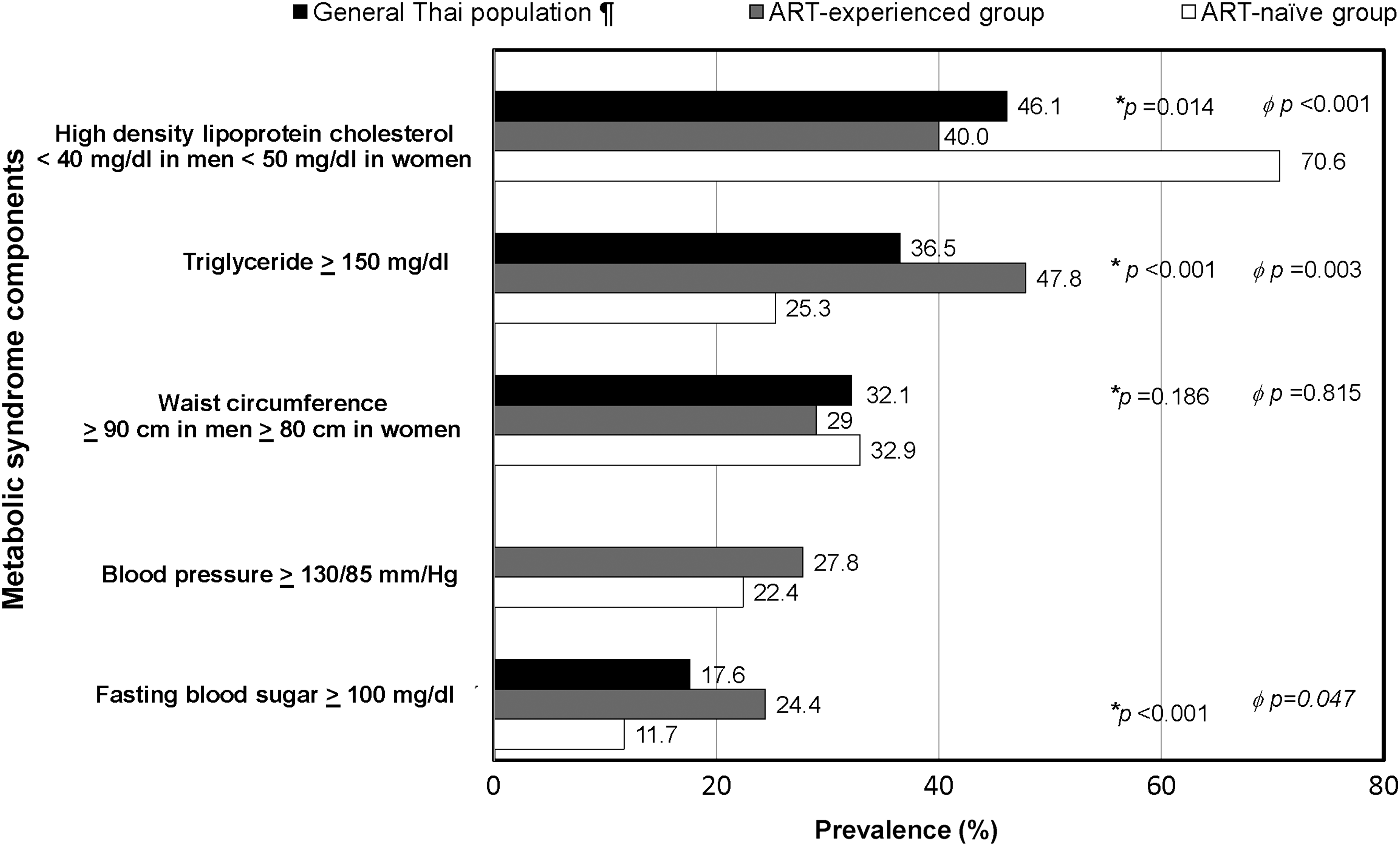
Prevalence of each component of metabolic syndrome by antiretroviral therapy status. ¶Data from general Thai population aged ≥15 years <29>, blood pressure data were not available in the reference study; *Comparing between general Thai population and ART experienced group; øComparing between general Thai population and ART-naive group.
Dietary intake and exercise
Among 473 participants (81.5%) with available dietary data, median energy intake was 1301 kcal (range 1003–1783 kcal). Median percent carbohydrate, protein, and fat intakes were 58.6% (range 49.1–66.8), 16.0% (range 13.5–19.5), and 24.0% (range 17.6–32.0), respectively. Across the country only 15.3% were categorized as having high energy intake (defined by dietary intake >2250 calories in men and >1800 calories in women), 34.7% had high carbohydrate intake (>60% of total energy), 28.8% had low protein intake (<15% of total energy), and 13.3% had high fat intake (>35% of total energy). 26,27 When dietary intake was compared among regions, there was a trend of higher energy intake in the North (38.6%), higher carbohydrate intake (54.3%) and lower protein intake (45.7%) in the South, and higher fat intake in the Central region (19%).
Exercise data were available in 555 participants (95.6%). Low exercise level, defined by engaging in moderate exercise <5 times per week or walking <30 min per day, was reported by 47.1% of these participants. Higher proportions of participants in the South (55.7%) and the North (54.3%) had moderate to high exercise levels than the other regions (p=0.001). Low exercise levels were found in 68.6% and 60.0% in patients from the East and Northeast regions, respectively.
Factors associated with metabolic syndrome
By univariate analysis, female gender, high cholesterol, and high LDL were common factors associated with MS in both ART-naïve and ART-experienced groups. In addition, being age >35 years, living outside Bangkok in ART-naïve group, and smoking and food insecurity in ART-experienced group were found to be associated with MS. Being age ≥35 years (odds ratio, OR, 4.2, 95%CI 1.6–11.0, p=0.004), high cholesterol (OR 4.7, 95%CI 1.7–12.9, p=0.002) and living outside Bangkok (OR 4.2, 95%CI 1.6–10.8, p=0.003) in ART-naïve group and female gender (OR 1.7, 95%CI 1.0–2.8, p=0.05), lipodystrophy (OR 1.8, 95%CI 1.0–3.0, p=0.032) high cholesterol (OR 1.9, 95%CI 1.1–3.1, p=0.015), and food insecurity (OR 1.8, 95%CI 1.0–3.3, p=0.05) in ART-experienced group were found to be significant risk factors for MS after the adjustment (Table 3). All variables, except for female gender in ART-experienced group, remained significantly associated with MS in a model where lipodystrophy was excluded (Table 4).
p value of≤0.05 was considered to be statistically significance.
ART, antiretroviral therapy; OR, odds ratio; PI, protease inhibitor.
p value of≤0.05 was considered to be statistically significant.
ART, antiretroviral therapy; OR, odds ratio; PI, protease inhibitor.
Factors associated with components of metabolic syndrome
By multivariate analysis, age >35 years (OR 3.2, 95%CI 1.6–6.4, p<0.001) and female (OR 3.0, 95%CI 1.5–5.7, p<0.001) were significantly associated with having at least two components of MS in ART-naïve group. In ART-experienced group, female (OR 2.3, 95%CI 1.4–3.7, p<0.001), lipodystrophy (OR 2.2, 95%CI 1.3–3.5, p=0.002), PI use (OR 2.8, 95%CI 1.3–6.0, p=0.007), hypercholesterolemia (OR 3.0, 95%CI 1.5–5.9, p=0.001), and high BMI (OR 1.1, 95%CI 0.6–1.8, p=0.023) were independently associated with having two components of MS after the adjustment of other variables (data not shown).
Discussion
We found a higher prevalence of MS among ART-experienced (24.9%) than ART-naïve (15.9%) HIV-infected Thai adults. These prevalence rates tended to be higher than the 13.2% MS prevalence among general Thai population of the same age (mean age of 38 years) to our study participants. 28 Compared to MS prevalence among 20,450 general Thais who participated in the fourth Thai National Health Examination Survey (NHES IV) in 2008–2009, HIV-infected women aged younger than 45 years in our study seemed to have a higher prevalence of MS than general Thai women (27.7% vs. 13.3% in women aged 30–44 years, 8.5% vs. 3.0% in women aged 15–29 years). 29
MS prevalence in our study was also higher than those in Italy (9.1%), 30 Spain (16–17.0%), 31,32 and Australia (18.0%), 33 but was in the same range as those in the US (22.9–25.5%) 34,35 and Taiwan (26.2%). 36 It is also important to note that 55.3% of our patients had at least two components of the MS criteria which might also contribute to the risk of CVD and type 2 diabetes. 37
Definition of MS is based on five components, namely, abdominal obesity, hypertriglyceridemia, low HDL, high blood pressure, and high fasting plasma glucose. Although abdominal obesity and insulin resistance were suggested to be more predictive of CVD and type 2 diabetes than other MS components, 20 this issue remains controversial. ART-naïve patients had a higher prevalence of low HDL, while ART-experienced patients had higher prevalence of hypertriglyceridemia and hyperglycemia, than general Thai population in the NHES IV 29 (Fig. 2). Unfortunately, the prevalence of high blood pressure was not recorded in that large general population study.
Similar to other studies of MS in Thailand and other countries, we identified older age, 28,35,38 –41 female gender, 38,39 and lipodystrophy 32,41 as associated or risk factors for the development of MS. Of these identified risk factors of MS, lipodystrophy may be prevented or modified by the selection of first-line ART regimens that are lipodystrophy-friendly, early detection of lipodystrophy, and early change of ART once lipodystrophy is detected. 32 As the fear of treatment-induced body changes, rather than MS in general, drives much nonadherence to ART in the resource-poor countries, 42 these early interventions to prevent lipodystrophy may also enhance ART adherence.
In this study, 45.2% of Thai HIV-infected adults had lipodystrophy as identified by patient's self-recognition and by the observation of the healthcare providers. Although subjective diagnosis of lipodystrophy may not be as accurate as dual energy x-ray absorptiometry scan, it is a real life practice in resource-limited settings. 43 Similar to finding from previous studies, 44 –46 our patients who were on ART, with a median duration of only 2.0 years for PI-based regimens and 2.6 years for NNRTI-based regimens, had a higher prevalence of lipodystrophy than ART-naïve patients. Considering that lipodystrophy is often associated with peripheral fat wasting and increased waist-to-hip ratio, it was not unexpected to also see a higher prevalence of increased waist-to-hip ratio in ART-experienced group. Therefore, monitoring waist-to-hip ratio may also be helpful as part of lipodystrophy screening in this population.
Due to the cross-sectional nature of this study, we could not assess the temporal relationship between MS or its components and the development of CVD. Association between lipodystrophy or MS and ART regimens also could not be assessed due to the complexity of ART history as a result of multiple changes of treatment regimens overtime. Longer term follow-up of these patients will be essential to assess clinical consequences of MS or its component overtime in HIV-infected population, with and without the effect of ART. Although recent data emphasized the possible role of suboptimal vitamin D levels in the development of metabolic disorders in HIV infection, 47,48 we did not have a chance to study this factor among our patients. Our data, however, are likely to be generalizable as it came from a large number of HIV-infected patients with various dietary intakes and exercise levels from different regions of Thailand. Specific MS prevalence and risk factors by ART status is also another strength of this study. These data could guide clinical practices in clinics that serve HIV-infected patients with similar characteristics to participants in this study.
At present, HIV-infected individuals with appropriate treatment are expected to have a near normal life expectancy. 49,50 Diseases associated with aging such as CVD and type 2 diabetes are expected to be seen more in aging HIV-infected population. Careful selection of ART regimens that do not cause lipodystrophy can help lower the risk of MS which can result in CVD and diabetes. To further reduce the risk of MS, diet and lifestyle modification such as exercise and smoking cessation should also be included as a standard component of long-term care for HIV-infected individuals.
Footnotes
Acknowledgments
The study team would like to thank all the study participants for providing their time and information and staff at the Thai Red Cross Anonymous Clinic, Bamrasnaradura Infectious Disease Institute, Queen Savang Vadhana Memorial Hospital, Sanpatong Hospital, Khonkaen Provincial Hospital, and Surat Thani Provincial Hospital for their works. We would like to thank Rita Bhatia for proofreading our article. Funding for the study was provided by the World Health Organization, South-East Asia Regional Office, and the intramural fund from the Thai Red Cross AIDS Research Centre.
Author Disclosure Statement
None of the authors have any relevant financial relationships that would present a conflict of interest with the material reported in this article.