
Abstract
HIV stigma is rooted in culture and, therefore, it is essential to investigate it within the context of culture. The objective of this study was to examine the interrelationships among individualism–collectivism, HIV stigma, and social network support. A social network study was conducted among 118 people living with HIVAIDS in China, who were infected by commercial plasma donation, a nonstigmatized behavior. The Individualism–Collectivism Interpersonal Assessment Inventory (ICIAI) was used to measure cultural norms and values in the context of three social groups, family members, friends, and neighbors. Path analyses revealed (1) a higher level of family ICIAI was significantly associated with a higher level of HIV self-stigma (β=0.32); (2) a higher level of friend ICIAI was associated with a lower level of self-stigma (β=−035); (3) neighbor ICIAI was associated with public stigma (β=−0.61); (4) self-stigman was associated with social support from neighbors (β=−0.27); and (5) public stigma was associated with social support from neighbors (β=−0.24). This study documents that HIV stigma may mediate the relationship between collectivist culture and social network support, providing an empirical basis for interventions to include aspects of culture into HIV intervention strategies.
Introduction
S
Stigmatization is a cultural construct and its experiences differ across countries and communities and thereby needs to be understood in this context. 8,10 Triandis distinguished between two types of cultures: individualist and collectivist cultures. 11,12 These opposing perspectives help to explain the differences of beliefs, attitudes, and behaviors across cultures. Individualistic cultural ideals dominate North American and Western European thoughts and emphasize the importance of the autonomous individual's needs and goals above all others. Individualistic cultures tend to be more heterogeneous and emphasize self-reliance and competition with others.
Conversely, collectivist cultures value interdependence and homogeneity within groups. While Asian cultures are predominantly collectivist, all cultures have varying levels of individualism and collectivism at multiple levels throughout society, including at the individual, interpersonal, and broader societal levels. 13,14 The extent to which a culture is more individualistic or collectivist is rooted within the norms of society. A systematic review of individualism–collectivism found that people from China have consistently endorsed strong collectivistic values compared to Americans. 15 China's collectivist culture stems from Confucianism, where interdependent group values are emphasized and individualistic self-guiding principles (e.g., individualistic tendencies) are negated. Focus on blending within the group to create a sole identity is supported by societal norms; however, if the identity of one person changes, the whole group's identity changes, leading to stigmatization of groups. Studies examining the relationships between culture and HIV stigma reveal that PLWHAs in collectivistic societies are more likely to experience stigma than individualistic societies. 16 In China, negative attitudes toward PLWHAs persist. HIV is viewed as an ignominy in Chinese culture, leading to marginalization, shame, and disgrace of the whole group due to one members' HIV status. 17
There is a plethora of research that has focused on the relationship between HIV stigma and social network support; most of these studies suggest that HIV stigma is a barrier to social network support. 18 –21 A systematic review among PLWHAs in the United States indicated that more perceived HIV stigma was associated with less social network support. 4 In China, our previous study showed that homosexual men who experienced a higher degree of stigma perceived more social network support from their sexual partners compared to non-sexual-partner peers. 22 This difference may be due to distinctions of cultural constructs because homosexuality in Chinese collectivist culture is harshly stigmatized. Homosexual men may turn to their homosexual partners for social network support because they are from the same marginalized group and share relatable experiences.
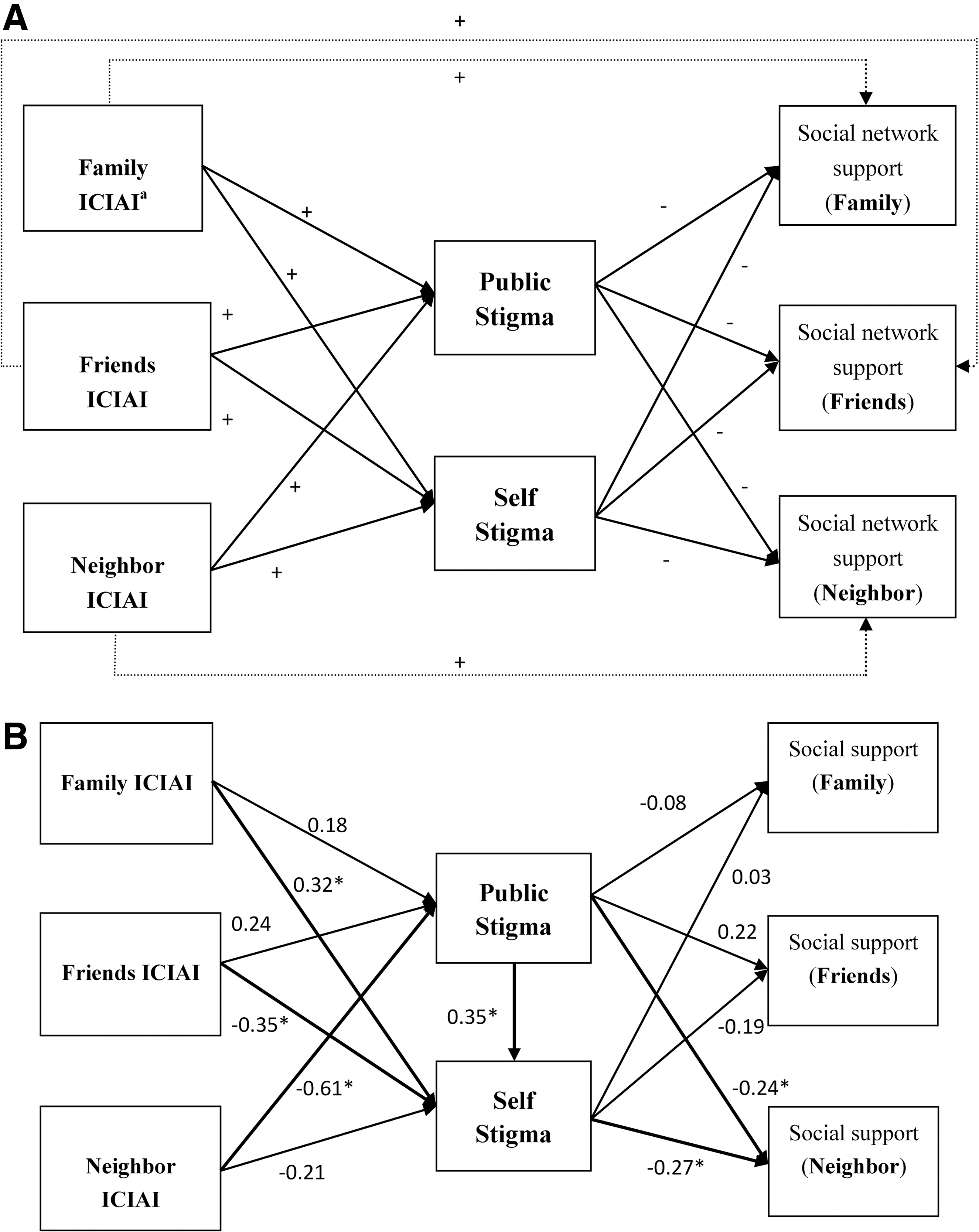
However, social network support may be directly influenced by both stigma and collectivism culture. Collectivist cultures embrace conformity and within group homogeneity, 12 thereby passing stigmatization to social network members and diminishing social network support. These inter-relationships have not been well studied. We thus conducted a study among PLWHAs in China and used path-analytic modeling to assess the interrelationships among individualism–collectivism, stigma, and social network support. We hypothesized that (1) PLWHAs who had higher levels of collectivism among family members, friends, and neighbors would perceived higher levels of public and self-stigma; (2) higher levels of public and self-stigma would be associated with lower levels of social network support from family members, friends, and neighbors; and (3) the individualism–collectivism culture is directly associated with social network support. The hypothesized relationships between collectivism culture, HIV stigma, and social network support are shown in Fig. 1A.
Methods
Study site
A cross-sectional study was conducted among PLWHAs in a rural area in Anhui province. 23 The majority of villagers were infected with HIV through commercial plasma donations that occurred in the early-to-mid 1990s. 24 The prevalence of HIV among commercial donors in this rural area was 10.5%. 25
Participant eligibility
Eligible subjects included PLWHAs who were at least 18 years old. PLWHAs who could not participate in an interview due to poor health conditions were excluded from this study. Based on the local HIV surveillance data (with PLWHAs' names and addresses), 25 we first selected villages with high HIV prevalence, and then listed all HIV-infected families, who were all invited to participate in the study. Because villagers were infected with HIV through a nonstigmatizing practice (commercial blood donation), they disclosed their HIV status to their family members. Nevertheless, rather than identifying the study as one specifically for PLWHA and their families, families were asked to participate in a general health study to protect the status of HIV-infected participants. The Institutional Review Boards of Virginia Commonwealth University and the Anhui Medical University Institute of Biomedicine approved this study protocol.
Interview
Eligible subjects received individual face-to-face anonymous interviews in a private room at each household. After receiving a complete description of the study, all eligible subjects who agreed to participate provided informed consent. Interviewers received training on maintaining participant confidentiality and privacy before conducting interviews. All interviews were conducted in Chinese.
Measurements
Questions in the questionnaire were drafted in English and then translated into Chinese by research members who were fluent in both languages.
Individualism-collectivism (IC)
The Individualism–Collectivism Interpersonal Assessment Inventory (ICIAI) was used to assess the tendencies of individualism and collectivism. 26 ICIAI provides a measure of the tendency toward individualism or collectivism and the perception of IC values with interpersonal orientation in different relationships (e.g., family, friends, and neighbors in this study). It consists of the role and obligations in interpersonal interactions and examines the relative importance of individualism or collectivism across a variety of social contexts. One could have both collectivistic and individualistic tendencies. For example, an individual may have collectivistic tendencies with family members but individualistic tendencies with neighbors. Previous studies have demonstrated that this instrument has high validity and reliability in multiple ethnic populations. 26 –28 The same inventory was used and assessed in our previous study in China and demonstrated good reliability (Cronbach's alpha ranged between 0.85–0.90). 29 The ICIAI has been well validated in different populations in different countries, such as the US, Japan, Russia, and South Korea. 26,30
The current study was adapted from our previous study to the new study population. 29 Social groups were limited to three types of relationships: family members (family ICIAI), friends (friend ICIAI), and neighbors (neighbor ICIAI). The final inventory scale included 54 items (18 items×3 relationship groups). These items were used to measure the level of IC tendencies toward three interaction relationships. Each item has a five-point scale with a response set coded as “not important at all (1), somewhat important (2), important (3), quite important (4), and very important (5).” Participants were asked to rate the importance of each item according to their values. The total score was calculated by summing the item scores in each group, with a higher ICIAI score indicating higher collectivism orientation. The composite score in each group ranged from 18 to 90. Reliability was assessed by the Cronbach's alpha coefficient and was 0.97 for family ICIAI, 0.97 for friend ICIAI, and 0.96 for neighbor ICIAI.
HIV stigma
Based on our previous studies on HIV stigma, 23,31,32 we designed a 13-item measurement scale to measure the level of public stigma (e.g., PLWHAs do not have the same educational or employment opportunities) and a 10-item scale to measure the level of self-stigma (e.g., feelings of self-accusation and shame from HIV status). Participant responses were ranked on a four-point scale ranging from “strongly disagree” to “strongly agree.” The composite score of public stigma and self-stigma ranged from 0–39 and 0–30, respectively. Higher scores indicated greater public or self-stigma. Cronbach's alpha coefficients demonstrated high reliability for public stigma (α=0.94) and self-stigma (α=0.93). Psychometrical properties of those measures have been assessed in our previous studies. 23,31,32
Social network support
The Chinese Social Network Questionnaire (CSNQ) was used to assess social network support at the family, friend, and neighbor levels, the reliability and validation have been assessed in previous studies. 22,33,34 To list social network peers, name-generating questions were used to ask respondents to list, by giving their first names or pseudonyms, peers who could provide social network support. They rated the possibility of social network support that they perceived to be available from each of their network peers (0 to 4; not possible at all, not sure, somewhat possible, quite possible, quite sure that the alter could provide support). Respondents were asked to rate the possibility that each peer would (1) lend the participant 50 Chinese Yuan (equivalent to $8 US dollars), or give immediate help if he/she needed it; (2) take care of the respondent if he/she was sick and confined to bed for 2–3 weeks; (3) provide help or advice if the respondent had problems regarding family or personal issues, or health concerns; (4) agree with or support the respondent's actions or thoughts; (5) make the respondent feel respected or admired; and (6) entrust in the alter to confide intimate details. Cronbach's alpha (α) coefficients showed good reliability with α=0.96 for social network support from family members, α=0.92 for social network support from friends, and α=0.95 for social network support from neighbors. The composite score for each social network member ranged from 0 to 24.
Analysis
Path analytic modeling was performed to assess the interrelationships of IC culture, stigma, and social network support among PLWHAs. Path analytic modeling allows one to test the interrelationships of the ICIAI, stigma, and social network support, indicating possible causal paths from ICIAI to social network support. As the majority of egos did not seek for support from their friends and neighbors, the variables that measured social support from friends or neighbors were coded into binary variables (1: with such support vs. 0: without). Standardized coefficients for all paths were estimated, controlling for gender, marital status, education, and age. Goodness-of-fit of models were assessed by the Bayesian information criterion (BIC). The model with smallest BIC value indicates that the model has better fit. 35,36 These analyses were completed using SAS 9.2 and Mplus 5.
Results
Characteristics of study sample and correlations
Table 1 presents the study participant's demographic characteristics. A total of 118 PLWHAs were invited and agreed to participate in the study. The median age of study subjects was 44 years old (IQR: 8.5) and 59% and 85% of subjects were female and married, respectively. The majority of PLWHAs received primary school education or less (83%) (Table 1). All study subjects were infected with HIV through commercial plasma/blood donation in the early-to-mid 1990s, except one who was infected through sexual contact. PLWHAs received a greater amount of social network support from their family members than from their friends or neighbors. Almost all PLWHAs disclosed their HIV status to network supporting members; only two did not.
PLWHAs, people living with HIV/AIDS.
Individualism–Collectivism Interpersonal Assessment Inventory.
Correlation coefficients of variables that were used in the path analytic model are reported in Table 2. The three ICIAI variables and two stigma variables were positively significantly correlated with each other. Both public stigma and self-stigma were significantly negatively correlated with friend ICIAI [correlation coefficient (r)=−0.20, and r=−0.36] and neighbor ICIAI (r=−0.31, and r=−0.38), but not with family ICIAI. Neighbor social network support was positively significantly correlated with friend ICIAI (r=0.18), and neighbor ICIAI (r=0.21), but negatively with public stigma (r=−0.31) and self-stigma (r=−0.28). Social network support from family members was positively significantly correlated with family ICIAI (r=0.20), and neighbor ICIAI (r=0.23), social network support from friends was not significantly correlated with other variables.
p≤0.05; aIndividualism-Collectivism Interpersonal Assessment Inventory.
Path analytic model analysis
Our hypothesized model included a direct path from family ICIAI, friend ICIAI, and neighbor ICIAI to perceived social network support provided by family members, friends and neighbors (see Fig. 1A). However, based on the value of BIC (BIC=3176.53), the direct path from ICIAI to social support was removed and a path from public stigma to self-stigma was added. The final model had the smallest BIC (BIC=3148.66), indicating better model fit (see Fig. 1B).
The standardized coefficient estimates of each path were statistically significant in the final model (p≤0.05) and the following relationships were observed among PLWHAs and levels of collectivism: (1) a higher level of family ICIAI was significantly associated with higher levels of self-stigma (β=0.32, 95% CI, 0.22 to 0.42); (2) a higher level friend ICIAI was significantly associated with lower levels of self-stigma (β=−0.35, 95% CI, −0.52 to −0.18); and (3) higher levels of neighbor ICIAI were significantly associated with lower levels of public stigma (β=−0.61, 95% CI, −0.80 to −0.42) (Fig. 1A and B).
Public stigma and self-stigma were strongly associated with each other (β=0.35, 95% CI, 0.27 to 0.43). The following associations were observed for social network support: (1) higher levels of self-stigma was significantly associated with lower levels of social network support from neighbors (β=−0.27, 95% CI, −0.49 to −0.04); self-stigma was insignificantly associated with social network support from family members (β=0.03, 95% CI, −0.07 to 0.13), and from friends (β=−0.19, 95% CI, −0.43 to 0.06); (2) public stigma was insignificantly associated with social network support from family members (β=−0.08, 95% CI, −0.28 to 0.12) and friends (β=0.22, 95% CI, −0.03 to 0.46), but higher levels of public stigma was significantly associated with lower levels of social network support from neighbors (β=−0.24, 95% CI, −0.47 to −0.02).
From the above statistical associations, we inferred three connected pathways: (1) higher family member ICIAI may increase self-stigma which, in turn, may reduce social network support from neighbors; (2) higher ICIAI among friends may reduce self-stigma which, in turn, may increase social network support from neighbors; and (3) higher ICIAI among neighbors may reduce public stigma which, in turn, may increase social network support from the neighbor.
Discussion
This study documents that HIV public and self-stigma may mediate the relationship between collectivist culture and social network support, providing an empirical basis for interventions to include aspects of culture into HIV intervention and prevention strategies.
We found that higher levels of family collectivism led to higher levels of perceived self-stigma. In traditional Chinese culture, the family is the basic unit of social organization and individuals are seen as embedded within this unit. 37 Thus, when an individual discloses their HIV status, the whole family is stigmatized and considered responsible for the HIV-infected group member. PLWHA with higher levels of family ICIAI may feel personal responsibility for the shame he/she has brought to his/her family, thereby internalizing feelings of guilt and increased sensitivity to negative feedback (self-stigma).
Our findings show that higher levels of collectivism toward friends are significantly associated with lower levels of self-stigma, and that higher levels of neighbor collectivism are significantly associated with lower levels of public stigma. When collectivism-oriented individuals are motivated by the norms of their group, whether that is at the interpersonal or community level, they sacrifice personal duties and goals for group priorities. The more adhering a person is to their group, the more likely they are to be accepted by their friends and community. 11 When a PLWHA keeps harmonious relationships with friends and neighbors, they may be less likely to stigmatize him/her. Additionally, the more supportive and accepting communities are of HIV disease, the less likely an individual is to experience stigmatization socially and internalize such events. PLWHAs in the study area were infected with HIV through commercial blood donation, not through stigmatizing behaviors (i.e., commercial sex contacts or drug use). In the early-to-mid 1990s, commercial blood donation was a common and acceptable practice in those areas. Under these circumstances, it is likely that individuals experience lower levels of self-stigma and public stigma on the friend and community levels, respectively. Also, because they were HIV infected through a nonstigmatizing practice (commercial blood donation, a very common practice in 1990s in the study area), they disclosed their HIV status to their family members and those they looked for social support.
A number of research reports that HIV stigma is negatively associated with social network support. 4,18,38 Our findings show that the relationship between HIV stigma and social network support coincides with each other and are more complicated. Both public and self-stigma were significantly associated with lower social network support from neighbors. Self-stigma hinders the ability of PLWHAs to seek social network support from their neighbors by internalizing feelings of self-hatred. 39 –41 Studies have demonstrated that those individuals who are most ashamed of their HIV infection experience increased worry about spreading their HIV infection to others and are less likely to access and attend support groups. 38 Societal attitudes of HIV-infected individuals include beliefs of isolating HIV-infected persons, immorality, and fear of infection from daily contact with HIV-infected individuals. 17,42 Public stigma impedes acceptance of HIV-infected individuals into mainstream society and hinders the ability to provide and maintain social network support to PLWHAs.
Interestingly, social network support from families and friends was not associated with public or self-stigma. In other words, no matter the degree of perceived stigma, PLWHA tended to seek support from their family members and friends. As documented in this study, PLWHAs received a larger amount of social network support from their family members than from others. This relationship may be explained by the tradeoff between perception of HIV stigma and obtainment of social network support among PLWHAs. Families may restrain support out of fear of contracting HIV or because of feelings of shame, disgrace, or loss of dignity to their family unit. Conversely, a family's support may be strengthened due to an obligatory culture of collectivism. Triandis, Bontempo, Villareal, et al. theorized that collectivist societies are more cohesive and are more likely to provide social network support when stressful life events occur. 43 The Chinese collectivist family unit is an asset that can provide its members with emotional and tangible support and strength to cope with and fight against HIV-related stigma and discrimination. 17 However, receiving social network support is dependent upon disclosing one's HIV status. A study in Thailand (another collectivism country) found that PLWHAs were more likely to disclose their serostatus to family members compared to other types of relationships. The main reason cited for HIV disclosure was for social network support. 44 Thus, the transaction between social network support and collectivism neutralizes stigmatization through HIV status disclosure. In other words, disclosing ones' HIV status creates balance between receiving social network support from family members and public and self-stigmatization. However, more research on this topic needs to be conducted. Similarly, PLWHA may consider their friends as the “in-group” and their neighbors as the “out-group” in the collectivist society, 12 which may result in their seeking social support from friends despite HIV stigma.
This study found that public and self-stigma are significantly associated. This is consistent with previous research that self-stigma begins with public stigma. 45,46 PLWHAs accept that they are surrounded by discrimination and prejudice from society, resulting in internalized negative attitudes toward themselves. Public stigma exacerbates self-stigma, which in turn prevents self-stigmatized individuals from receiving social network support from network members—that is, self-stigma mediates the relationship between public stigma and social network support.
HIV stigma may mediate the relationship between Individualism–Collectivism culture and social network support. We found that higher levels of family member ICIAI increase self-stigma, which, in turn reduces social network support from neighbors, even with infection from a nonstigmatized behavior, such as commercial blood donation. In the context of the Chinese culture, families are considered an interdependent group and the identity of one person becomes the identity of the group. Therefore, since the family unit's identity adversely changes with a member's HIV diagnosis, the PLWHA may be more likely to internalize feelings of guilt and shame to one's family. 17 Added burden may also be placed on family caregivers of PLWHAs, especially as new infections increase among older populations in China. 5 Moreover, families may experience ‘courtesy stigmatization’ for their association with a PLWHA 47 . Together, these may further intensify feelings of remorse by PLWHA and potentially explain the positive association found between family collectivism and self-stigma.
Higher friend and neighbor ICIAI may lead to increased social network support as potentially mediated by stigma. The findings of mediation effects of stigma on social network support indicate that intervention programs that increase social network support should take unique aspects of the Chinese culture into consideration.
There are a few limitations to this study that should be acknowledged. While the study site embodies traditional Chinese culture, within-culture heterogeneity exists among all cultures and therefore, may not be generalizable outside of this population. This study had a relatively small sample size and was conducted under a cross-sectional study design; thus the findings are limited to interpretations of association and not causality. However, these results are meaningful in the context of the collectivist Chinese culture to reduce stigmatization of PLWHA and increase social network support. Larger, more robust studies are needed among other collectivist cultures to verify the results from this study.
The relationships between culture, stigma, and social network support are complicated and are context specific. Our study documents that HIV public and self-stigma is driven by Individualism–Collectivism culture. Further, HIV public and self-stigma mediates the relationship between collectivism culture and social network support. These findings illustrate the need for culturally independent multilevel interventions that address education on HIV transmission to the public and access to support services for PLWHA to decrease stigmatization and increase access to care. Understanding social beliefs, values, and norms in the context of individualism and collectivism cultures may facilitate the development of effective HIV prevention and intervention policy strategies to reduce cultural stigmatization.
Footnotes
Acknowledgments
We are grateful to the staff from Anhui Medical University for participation in the study and to all the participants who gave so willingly of their time to provide the study data.
Funding: This work was supported by a research grant from the Virginia Commonwealth University School of Medicine and Anhui Medical University. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
No competing financial interests exist.