
Abstract
This review synthesized the literature for barriers to HCV antiviral treatment in persons with HIV/HCV co-infection. Searches of PubMed, Embase, CINAHL, and Web of Science were conducted to identify relevant articles. Articles were excluded based on the following criteria: study conducted outside of the United States, not original research, pediatric study population, experimental study design, non-HIV or non-HCV study population, and article published in a language other than English. Sixteen studies met criteria and varied widely in terms of study setting and design. Hepatic decompensation was the most commonly documented absolute/nonmodifiable medical barrier. Substance use was widely reported as a relative/modifiable medical barrier. Patient-level barriers included nonadherence to medical care, refusal of therapy, and social circumstances. Provider-level barriers included provider inexperience with antiviral treatment and/or reluctance of providers to refer patients for treatment. There are many ongoing challenges that are unique to managing this patient population effectively. Documenting and evaluating these obstacles are critical steps to managing and caring for these individuals in the future. In order to improve uptake of HCV therapy in persons with HIV/HCV co-infection, it is essential that barriers, both new and ongoing, are addressed, otherwise, treatment is of little benefit.
Introduction
U
Current guidelines recommend that both HIV antiretroviral therapy and HCV antiviral therapy be considered for all co-infected patients to slow progression of liver disease and to achieve sustained virologic response (SVR). 9,10 Combination antiviral therapy of pegylated interferon and ribavirin (PegIFN+RBV) has been the mainstay of HCV therapy for many years, based on clinical efficacy in reducing SVR in persons with co-infection. 11 However, effectiveness in clinical practice is limited and is typically attributed to high rates of treatment ineligibility, poor patient involvement in medical care, and waning adherence to prescribed regimens over time. 12 –14 These factors are compounded by the fact that attaining optimal SVR is more difficult in those with co-infection as compared to those with HCV monoinfection. 15 Other challenges that are unique to HIV co-infection include the concern for drug–drug interactions and excess toxicities with concomitant antiretroviral medications. 9,10
Fortunately, the field of HCV care is rapidly evolving, given the arrival of two direct-acting antiviral agents (DAAs), telaprevir and boceprevir. In addition to these medications, both simeprevir and sofosbuvir have just recently been approved by the FDA and give promise for more therapeutic options for patients with HCV. 9,16 Presently, telaprevir and boceprevir, both NS3/4A protease inhibitors, are only FDA-approved for the management of persons with HCV monoinfection. Based on emerging results from clinical trials, guidelines now endorse the use of DAAS, in combination with PegIFN+RBV, giving rise to an effective, triple-drug regimen for patients with co-infection. 9,17,18
Despite the clinical promise of newer agents, some of the historical challenges to treating co-infected patients are still obstacles to treatment. We sought to survey the current landscape for barriers to treatment uptake in co-infected patients. The objectives of this review were to synthesize the literature pertaining to HCV antiviral treatment barriers and to compile and classify documented barriers in persons with HIV/HCV co-infection. This knowledge is useful to better address and overcome existing barriers in the context of rising DAA use, with the ultimate intent of improving access and uptake of HCV treatment for these patients.
Methods
Search strategy
A series of searches of the PubMed (1950–2012), Embase (1974–2012), and CINAHL (1984–2012) databases were conducted in September 2012 to identify articles that examined barriers to HCV therapy in HIV/HCV co-infected patients. A series of initial searches were conducted using key words and MeSH terms in various combinations in order to yield the maximum number of articles that were deemed relevant to the review. An overview of the final search strategies for each of the three databases is outlined in Table 1. A subsequent query of the Web of Science database was conducted to broaden the search net in an attempt to capture articles that may have been otherwise overlooked. This process involved extensive hand searches for closely matched citations, beginning with the references of two index articles that addressed the theme of barriers to antiviral therapy in co-infected populations. 19,20 An overview of the article selection process is illustrated in Fig. 1.
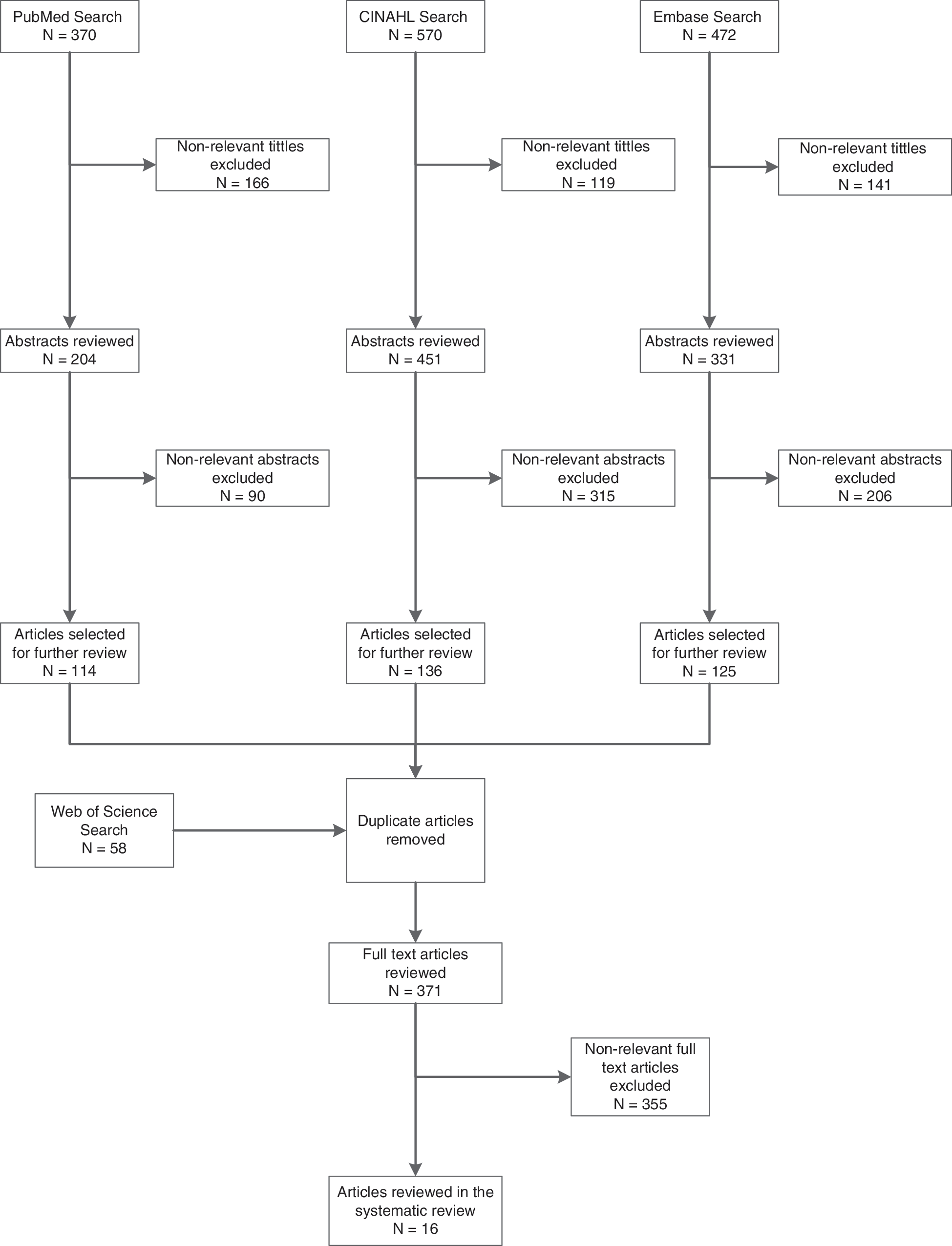
Flow diagram of article selection process.
Inclusion and exclusion criteria
Articles were excluded from the review based on the following criteria: (1) study conducted outside of the United States; (2) not original research (e.g., treatment guidelines, review articles, case studies, case reports, editorials, commentaries, review articles); (3) pediatric study population; (4) experimental study design (e.g., clinical trial designed to determine therapeutic efficacy in a controlled setting); (5) non-HIV and non-HCV study population; and (6) article published in a language other than English.
Search protocol
First, two independent reviewers (HNM and JCT) screened all of the titles from each of the databases based on the above criteria to exclude nonrelevant articles. A third reviewer (CUO) adjudicated any discordant title exclusions. A similar process was employed to screen abstracts of remaining articles. At this point, all remaining articles were entered into an electronic database, consolidated, and screened for duplicates. Two reviewers (HNM and JCT) then evaluated the full text of these articles for the above exclusion criteria. The third reviewer (CUO) adjudicated any discordant full-text exclusion determinations. We categorized barriers as one of the following: absolute/nonmodifiable medical barriers, relative/modifiable medical barriers, or nonmedical barriers. These classifications were based on categories that have been previously used in the HCV literature. 2,9,21,22
Results
Characteristics of included studies
This systematic review presents a summary of the 16 studies that met study criteria. A detailed overview from the findings of each of these studies is located in Table 2. The articles varied widely in both study setting and study design. The earliest year of study observation was in 1996, 23 and the most recent data were from 2006. 24 Most patients in these studies were managed in specialty clinics. The four studies with the largest sample sizes used nationally representative data from the Veteran Affairs (VA) system. 24 –27 Three studies were conducted in Boston, MA, 28 –30 and three studies prospectively administered questionnaires or interviews to participants to gather information. 24,31,32 In all studies which reported gender, the majority (54–99%) of participants were male.
B, Black/African American; H, Hispanic/Latino; O, other/unknown; W, white/Caucasian.
HCV treatment rates (prior or current) varied widely. In one study, rates were as low as<1%. 33 Patients were enrolled in this study between 1999 and 2000, soon after clinical evidence became available supporting the use of IFN+RBV for HCV. 34 Even though the data were from individuals with HCV monoinfection, HIV infection was not considered a contraindication to therapy at that time. 35 In a separate study, rates were as high as 62%; however, this represented patients who had already met treatment eligibility criteria and who subsequently initiated therapy. 32 HIV antiretroviral treatment rates (prior or current) were generally higher than HCV treatment rates; more than half of the studies had HIV treatment coverage >50%, when reported.
This review presents the common themes of treatment-related barriers identified in the 16 articles. An overview of the documented barriers and themes are presented in Table 3.
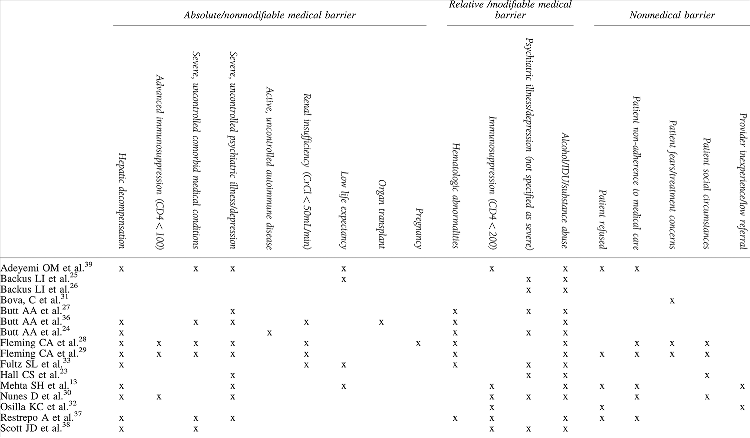
Absolute/nonmodifiable medical barriers
Hepatic decompensation, noted in 10 studies, was the most commonly documented barrier in this category. In one study, 26% of veterans with co-infection were diagnosed with this condition. 36 Diagnoses of decompensated liver diseases in these veterans were defined as elevated INR (>1.3), elevated total bilirubin (>2.0 mg/dL), low albumin (<2.5 g/dL), esophageal varices, ascites, or hepatic encephalopathy. Half of all studies (n=8) cited severe, uncontrolled psychiatric illness, including depression, as an absolute contraindication. Major depression was as high as 57% in one study. 25 Nunes et al. made the distinction for condition severity by classifying depression as either an absolute contraindication or as a relative contraindication. 30 Patients with prior suicidal attempt (35%) and recent suicidal ideation (9%) had an absolute contraindication to antiviral therapy. Patients with significant depressive symptoms (70%), defined as a score ≥16 on the Center for Epidemiologic Studies Depression Scale (CES-D), had a relative contraindication to therapy. Depressive symptoms were deemed to be exceedingly high by the investigators, even though many patients received psychiatric care (over 50%).
Severe, uncontrolled co-morbidities were barriers in six articles; co-morbidities were most often due to cardiac disease when a specific condition was listed. 29,36,37 Renal insufficiency and/or renal failure was a treatment barrier in four studies. The highest prevalence was in one of the studies by Butt et al., wherein 19% of veterans had renal failure, defined as elevated serum creatinine (>1.5 mg/dL). 36 Only one study cited active, uncontrolled autoimmune disease as an absolute contraindication. 24 Data were retrieved through patient self-report or via medical chart abstraction and was a contraindication for 12% of veterans. Details on the type of autoimmune disorders were not available.
Relative/modifiable medical barriers
Substance use was the most common of all barriers in this review (n=14 articles). Rates were especially high in one of the studies by Backus et al., which documented 64% of co-infected veterans with alcohol abuse, 68% with substance abuse, and 63% with hard drug abuse. 25 The investigators employed a liberal definition of substance abuse using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes. Codes for substance abuse included drug psychoses, drug dependence, cannabis abuse, hallucinogen abuse, barbiturate and similarly acting sedative or hypnotic abuse, opioid abuse, cocaine abuse, amphetamine or related acting sympathomimetic abuse, antidepressant-type abuse, and other, mixed, or unspecified drug abuse. The investigators were unable to differentiate injection drug use as a form of substance abuse using ICD-9-CM codes, rather they defined hard drug use to include opioid-type dependence, cocaine dependence, amphetamine and other psychostimulant dependence, combinations of opioid-type drug with any other, opioid abuse, cocaine abuse, and amphetamine or related acting sympathomimetic abuse. High rates of substance abuse were reported in two of the studies conducted by Butt et al. 27 Half (56%) of the nationally representative sample of co-infected veterans in their earlier study were diagnosed with drug use based on ICD-9-CM codes. 27 Multivariable logistic regression revealed drug use as a significant predictor for lack of HCV therapy (OR 0.68, 95% CI: 0.53–0.88). 27 In their subsequent study, substance use was documented via self-report, and/or chart abstraction in patients referred for care in specialty clinics. Twenty percent of these patients reported recent alcohol abuse (defined as alcohol use more than once a week) and 60% reported recent injection drug use (definition not provided). 24 Similarly, in the study by Nunes et al., the prevalence of heavy alcohol use was 29% and was noted as the most common reason for not receiving HCV antiviral therapy. 30
For eight articles, psychiatric illness/depression was classified as a relative/modifiable barrier. Depression was the most common contraindication in one of the studies by Butt et al., present in two-thirds (67%) of patients. 24 With exception to the Nunes et al. study, 30 there was often no description of condition severity or control. For example, Scott et al. did not evaluate depression severity; however, diagnosis with a psychiatric illness/depressive condition was one of the reasons providers did not evaluate patients for HCV therapy. 38 Half of participants with co-infection in the Veterans Aging Cohort three-site study (VACS-3) had depression or bipolar disorder as a contraindication to treatment.
Barriers attributed to hematologic abnormalities or immunosuppression (CD4 cell count <200) were documented to a lesser extent. Of the seven studies that reported hematologic abnormalities, anemia was as high as 43% in one study. 36 Diagnosis was based on objective laboratory data (hemoglobin <12 g/dL for men, <11 g/dL for women). Hematologic disorders were grouped along with other co-morbid conditions in some articles, thus, the exact frequencies could not be elucidated in these studies. 28,29,37 Immunosuppression, in six of 16 articles, was the least common relative barrier. CD4 cell count was an indicator of treatment eligibility for patients managed in an urban liver/gastroenterology clinic in New York. Patients with CD4 <200 were less eligible to receive HCV treatment as compared to patients with CD4 >200 (p=0.01). 37 A similar effect was seen in patients seeking care at three Los Angeles area HIV clinics. 32 When controlling for other patient and provider variables, CD4 ≤200 was independently associated with a decreased likelihood of patient acceptance of HCV treatment (OR 0.08, 95% CI: 0.01–0.40).
Nonmedical barriers
Nonmedical barriers in this review were classified as occurring at either the patient level or at the provider level. In order of frequency within the 16 studies, patient-level barriers included nonadherence to medical care (n=6), 13,28 –30,37,39 refusal of therapy (n=5), 13,29,32,37,39 social circumstances (n=4), 23,28 –30 and fears and treatment-related concerns (n=3). 28,29,31 Provider-level barriers included provider inexperience with antiviral treatment and/or reluctance of providers to refer patients for treatment (n=2). 13,32
Discussion
This review reveals the many challenges and persistent themes in barriers that are unique to patients with HIV/HCV co-infection. A surprising finding was the lack of recent data in this field; the most recent study captured data from 2006. This may be due to the prospect of new and ultimately more efficacious medications to manage HCV. However, if barriers to therapies still exist, the underlying problems regarding low treatment rates will persist. Thus, the concerns of treatment-related challenges in patients with HIV/HCV co-infection are perhaps even more relevant as the field continues to evolve.
HCV treatment should be considered in all patients with HIV/HCV co-infection. 9 In some circumstances, therapy can be deferred or delayed for those with minimal HCV disease, in anticipation of newer therapies on the drug development horizon. 9 Treatment should not be initiated in cases where the risks outweigh the benefits. Examples of such absolute medical contraindications include sarcoidosis and hemoglobinopathies, due to the increased risk of disease flare. 40,41 Likewise, HCV antiviral therapy is not recommended for pregnant women or for individuals trying to conceive, as pregnancy is a contraindication due to teratogenicity concerns. 9 Both telaprevir and boceprevir are pregnancy category B; however, more severe ratings apply since they are to be used in conjunction with PegIFN+RBV (PegIFN is pregnancy category C and RBV is pregnancy category X). For patients with absolute contraindications due to RBV, PegIFN monotherapy is a less efficacious, but viable option for a regimen. 42,43 Nevertheless, these conditions were rarely documented as barriers in the present review. Rather, the most common absolute barriers were hepatic decompensation, severe/uncontrolled co-morbid conditions, and psychiatric illness. One theme noted was frequency of hepatic decompensation that prevented patients from receiving treatment. Individuals with decompensated liver disease should be evaluated for liver transplantation, where feasible. 9 For those with sustained liver damage or poor life expectancy, the efficacy of antiviral therapy is negligible and is therefore of limited efficacy for these patients. 8 The only plausible intervention to improve treatment rates in these individuals is to identify and evaluate them for treatment earlier on in the course of their disease.
Some studies cited conditions as nonmodifiable treatment barriers when they did not necessarily fall into this category. Butt et al. listed the presence of an autoimmune disorder (to include rheumatoid arthritis, systemic lupus erythematosus, or autoimmune hepatitis) as a contraindication, but did not describe level of disease severity. 36 Of note, the guidelines distinguish such conditions on the basis of severity or level of control. The distinction is important because patients can be re-evaluated for HCV therapy if these co-morbidities are clinically managed. For example, uncontrolled conditions such as autoimmune disorders can be treated with monoclonal antibodies such as adalimumab, and hematologic abnormalities can be managed with erythropoiesis-stimulating agents, such as erythropoietin. 9 This clinical distinction is relevant as it is possible that therapy could have been initiated in patients whose conditions were non-severe or were controlled.
Substance abuse, inclusive of either injection drug or alcohol use, was a common barrier in this review. The high prevalence is partially explained by composite definitions of substance abuse. For example, the highest occurrence was in a study by Backus et al.; the broad definition of substance abuse including diagnoses that do not constitute barriers to HCV therapy. 25 Some studies explicitly cited alcohol, injection drug use, and/or substance abuse as a reason for excluding patients from receiving HCV antiviral therapy altogether. 24,28 –30,33,36,37 However, histories of substance abuse or injection drug use should not preclude a patient from receiving antiviral therapy. 44 Treatment has successfully been delivered to injection drug users. 45 –48 Findings from two recent meta-analyses examining antiviral treatment in HCV-infected injection drug users demonstrate acceptable outcomes in this patient population. 49,50 Based on the 36 studies that met inclusion criteria, the treatment completion rate was high at 83.4% (95% CI: 77.1–88.9%). 50 Pooled SVR was similar in both meta-analyses, reaching a rate of 55.5% (95% CI: 50.6–60.3%) in the meta-analysis by Dimova et al. 50 and 56% (95% CI: 50–61%) in the meta-analysis by Aspinall et al. 49 These response rates are comparable to SVRs that have been achieved in clinical trials evaluating the efficacy of HCV antiviral therapy, which further supports the ability to treat injection drug users successfully. 51,52 Per recommendations to manage HCV infection among injection drug users by Robaeys et al., patients should undergo a comprehensive pre-therapeutic assessment to educate patients regarding the risks and benefits of treatment and to link patients to necessary support services. 44 Treatment should be considered on a case-by-case basis using a multidisciplinary team approach to care management. 44
Adherence encompasses both adherence to medication use and adherence to medical care, both of which are critical to treatment success. 53 Patient adherence is often perceived by the provider as an indicator of treatment readiness and is based on characteristics such as mental health, clinic attendance, substance use, and the patient's attitudes and beliefs towards therapy. 53 A suggested mechanism to improve adherence is that counseling efforts should be tailored to the patient, to include routine inquiry and monitoring for barriers to adherence and identifying potential solutions to overcome patient-reported barriers when they arise. 14 While the risk for reinfection following successful treatment is generally low, 54 patients should receive harm reduction education and be monitored annually for reinfection. 44
Psychiatric illness/depression was documented as a barrier in many studies. Interferon can cause depressive-like symptoms in patients taking antiviral therapy, which is of concern as underlying mood instability and other neuropsychiatric symptoms can worsen in the setting of interferon. 59,60 It is recommended to distinguish between severe, active psychiatric illness with suicidal ideation as an absolute contraindication, versus nonactive illness as a modifiable or relative contraindication. 9 This distinction is important, given that HCV treatment should be considered for patients who have undergone successful psychiatric care and/or treatment for depression. 61 Similar to broad definitions used for substance abuse, some studies employed broad definitions for psychiatric disorders and/or depression using ICD-9-CM codes. 25 Presence of a psychiatric co-morbidity is not indicative of adherence, treatment completion, or SVR; rather, patients with psychiatric disorder or major depressive disorder have successfully undergone antiviral treatment. 62,63 However, it is imperative to document active, uncontrolled neuropsychiatric disorders and to encourage psychiatric consultation where appropriate prior to initiating treatment to assess the need for pharmacological interventions. 61 During the first 3 months of treatment, patients should be monitored for mood changes every 4 weeks, followed by every 12 weeks thereafter. 61 Patients with psychiatric co-morbidities should be monitored every 2–4 weeks during the first 3 months of treatment, followed by every 4–6 weeks thereafter. 61 Pharmacological interventions may also be used during treatment to manage psychiatric symptoms.
Other barriers that were documented to a lesser extent included hematologic abnormalities and immunosuppression. As with other relative contraindications, HCV therapy should be reconsidered in cases where abnormalities are corrected. One issue regarding hematologic abnormalities is treatment-induced cytopenia from both RBV (anemia) and PegIFN (anemia, neutropenia, lymphopenia, and thrombocytopenia). 9 Such abnormalities are deemed to be severe and uncontrolled based on laboratory values such as hemoglobin <10 g/dL, absolute neutrophil count <1000/μL, and platelet count <50,000/μL. One strategy to address these abnormalities is dose reduction of antivirals. 64 Alternatively, adjuvant therapy, such as hematopoietic growth factors, can be initiated in some patients to address neutropenia (filgrastim) or anemia (erythropoietin alfa or darbepoetin alfa). 65,66 Immunosuppression is considered to be a barrier to treatment due to the possibility of lymphocyte reduction from PegIFN. 9 However, this can be modified, given that antiretroviral therapy is recommended to increase CD4. 10 Achieving immune reconstitution may be more attainable for more patients with co-infection as current guidelines now recommend antiretroviral therapy for all individuals with HIV infection. 10
There were fewer nonmedical barriers than either absolute or relative medical barriers. These generally encompassed those perceived at the patient level and most often involved the inability for patients to adhere with medical care. In one article, failure to attend office visits regularly or loss to follow-up during the evaluation process prevented 40% of patients from receiving treatment. 37
Other nonmedical barriers included a combination of treatment refusal, fear, treatment concerns at the patient level, and inexperience and low referral for treatment at the provider level. These obstacles can be addressed through improved patient pretreatment education and provider education. 2 Various models of care can be employed to improve HCV antiviral treatment uptake; examples of such models include integrating HCV care with substance abuse services, opioid substitution clinics, and primary care clinics. 67 Part of the action plan of the U.S. Department of Health and Human Services' Action Plan for the Prevention, Care & Treatment of Viral Hepatitis explicitly entails educating and training the multidisciplinary health care workforce of professionals, as well as communities, to be aware of the benefits of hepatitis prevention, care, and treatment. 68 The present focus for managing co-infection is to “seek, test, treat, and prevent.” 2 Improved HCV education and training can enhance disease assessment, engagement in care, and universal treatment, all of which are critical to ultimately eradicating HCV in persons living with HIV.
Undoubtedly, new therapies will revolutionize HCV care over the next few years. Forthcoming oral IFN-free regimens may improve medication adherence. 70 However, many of the barriers identified in this review may still apply to individuals with co-infection. In fact, it is likely that treatment will become more complex for triple therapy (DAAs+PegIFN+RBV), given the increased risk of drug–drug interactions, side effects, and pill burden. 2,9 These issues will continue to be pertinent until IFN-free and RBV-free regimens are the mainstays of treatment. There is still the need for improved access to care, earlier detection of disease, and adherence to medical care. Access to care is necessary in order to identify patients before they progress to hepatic decompensation or poor life expectancy, when treatment is no longer effective. Even in the approaching era of IFN-free regimens, efforts are still needed to reduce nonmedical barriers such as lack of adherence and patient and provider education. Treatment is of little benefit if measures to improve adherence to care are not instituted. It is imperative that both new and ongoing barriers are addressed in order to improve uptake of HCV therapy in individuals with HIV/HCV co-infection.
Limitations
This article is subject to the inherent limitations of a systematic review. Foremost, this review may have inadvertently excluded articles. Despite a comprehensive search strategy that explored articles in PubMed, EMBASE, CINAHL, and Web of Science, it is possible that some articles were erroneously excluded. This review only included research that was conducted within the United States. Excluding non-U.S. research decreased the number of articles examined. This requirement most likely biased the results by excluding data from countries that have different health care systems. However, this exclusion was intentional as barriers were thought to be unique to a given health care system and, therefore, not directly comparable across countries. Another limitation of this review is that the findings may not represent all barriers to newer anti-HCV medications. As a result of the close proximity between when the literature review was conducted and when the DAAs first became available, it is unlikely that sufficient time was given for challenges unique to these new medications to be published. This limitation is overcome by the standard of care to prescribe DAAs in conjunction with PegIFN+RBV; therefore, many barriers identified in this review are still generalizable to newer regimens. An additional limitation of this article is publication bias leading to over-representation of articles yielding positive results. Reviews can only examine published literature, as currently no way exists to examine unpublished literature. It is likely that our study overstates the results in the positive as a result of this bias.
Conclusions
To our knowledge, this is the first review specifically targeted to examine barriers to HCV antiviral therapy in individuals with HIV/HCV co-infection. The findings of this review reveal the many challenges and persistent themes in barriers that are unique to this patient population. Additionally, this study highlights the lack of recent studies addressing this topic. This is of special importance when considering the innovative changes to HCV management, namely the advent of triple therapy for HCV infection and new anti-HCV agents in the drug pipeline. It is critical that more research is conducted concerning barriers to treatment, to capture the full benefit of these new and unique agents as the treatment landscape continues to change. Documenting and evaluating these obstacles are critical steps to effectively managing and caring for these individuals in the future; it is essential that barriers, both new and ongoing, are addressed, otherwise, treatment is of little benefit. Thus, future research should consider possible solutions to the identified barriers; both medical and nonmedical, to enhance treatment-related outcomes for the HIV/HCV co-infected population.
Footnotes
Acknowledgments
The authors would like to thank Dr. Angela Kashuba for her assistance with this article.
Financial disclosure: This work was funded by a developmental grant awarded to Dr. Oramasionwu from the University of North Carolina at Chapel Hill Center for AIDS Research (CFAR), an NIH funded program P30 AI50410. Dr. Oramasionwu was also supported partially by the NIH Loan Repayment Program (LRP) through the National Institute on Minority Health and Health Disparities (Grant Number: L60MD003770).
Author Disclosure Statement
The authors have no further disclosures relevant to this article, and declare no other conflicts of interest.