
Abstract
Poor adherence to combination antiretroviral therapy (ART) is a major global challenge. In this study we examined the efficacy of a smartphone application incorporating personalized health-related visual imagery that provided real-time information about the level of medication and the patient's level of immunoprotection, in order to improve adherence to ART. We randomized 28 people on ART to either a standard or augmented version of the smartphone application. The augmented version contained components that illustrated participants' current estimated plasma concentrations of antiretroviral drugs and the immune protection provided by ART. Adherence to ART was assessed at baseline and at 3 months using self-reported adherence, pharmacy dispensing records, and HIV viral load. Information was also collected on illness and medication beliefs and use of the application. Participants who received the augmented application showed a significantly higher level of self-reported adherence to ART at 3 months (p=0.03) and decreased viral load (p=0.023) as compared to individuals using the standard version. Greater usage of the extra components of the augmented application was associated with greater perceived understanding of HIV infection and increased perceived necessity for ART. Smartphone applications that incorporate personalized health-related visual imagery may have potential to improve adherence to ART.
Introduction
C
Many existing psychological interventions have been shown to produce only modest improvements in adherence to ART and have often required considerable resource investment, which compromises feasibility in the clinical setting. 11,12 Recent studies in other chronic illnesses suggest patients' perceptions of their illness and medication present researchers with a valuable target for adherence-promoting interventions. 13,14 In particular, visual representation of the mode of action and the physiological effects of treatment have been shown to modify maladaptive illness perceptions and medication beliefs to be more conducive to optimal adherence. 14,15 Illness-related imagery can make a health condition more concrete or real to the individual, improving their understanding of the implications of non-adherence, and consequently, motivating and maintaining positive behaviour change. 16,17
The recent development of Internet-enabled smartphones has enabled the delivery of personalized health-related information as a method of improving adherence to treatment. 18 Smartphones have been shown to be an acceptable method of delivering HIV interventions 19,20 and for assessing adherence to ART and other relevant health behaviors. 21 New interventions using smartphone technology can be tailored to the individual patient, incorporate visual imagery, include multimedia information, and provide real-time feedback on adherence behavior. 22 Further, such interventions also have the potential to be cost-effective and scalable to the large numbers of people living with HIV worldwide. 23
The current study aimed to examine the efficacy of a smartphone application incorporating personalized health-related visual imagery that provided real-time information about the level of medication and the current level of immunoprotection in the patient's body, in order to facilitate adherence to ART. It was hypothesized that use of this intervention would enhance adherence to the ART regimen, as measured by the Medication Adherence Report Scale (MARS) and pharmacy dispensings, and this would also result in beneficial effects on the patient's viral load. A secondary hypothesis was that such an intervention would improve perceived understanding of HIV infection, elicit stronger perceptions of treatment control, and increase the perceived necessity for ART.
Methods
Participants
Participants were recruited from the Auckland City Hospital Infectious Diseases outpatient clinic and from Body Positive Incorporated (a local HIV support organization). Individuals were eligible to participate if they had been on ART for at least 6 months and used an Android smartphone (Android version 3.1 or later).
Procedure
Participants were randomized into either the active control group or the intervention group (Fig. 1). Individuals in the active control group were provided with a standard version of the smartphone application which comprised a 24-h medication clock displaying the participant's daily ART dosing schedule. This function allowed the participant to record when they had taken their medications each day.
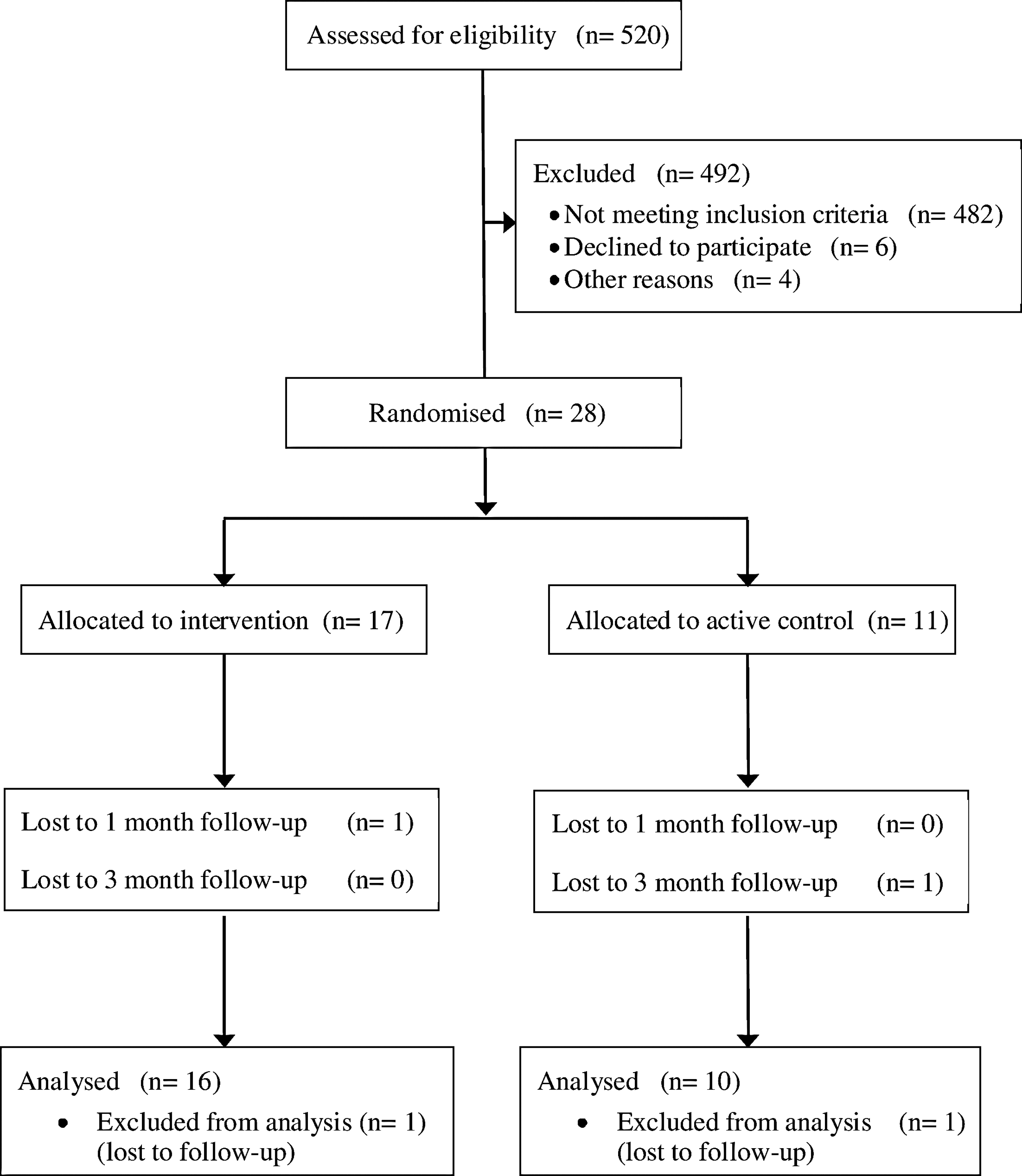
CONSORT diagram detailing participant progression through the study.
Participants in the intervention group received an augmented version of the application which, in addition to the 24-h medication clock, contained: (1) graphical representations of the estimated plasma concentrations of each of their antiretroviral medications, and (2) a personalized disease-state simulation of immune activity that comprised a moving pictorial representation of the patient's CD4 count and HIV viral load (based on their most recent blood tests). Protective barriers around the CD4 lymphocytes are made up of each of the ART medications the patient is taking. When any medication is not taken and the concentration drops below the recommended level, the protective barrier corresponding to that medication breaks down and virus begins attacking the CD4 lymphocytes (Figs. 2 and 3). Both the plasma level of the drugs and immune activity representation change in response to participants entering their medication dose taking into the application. This allows the participant to visualize, in real-time, the physiological effects of his or her adherence to ART. It was intended that these functions would facilitate and improve adherence by enhancing participants' understanding of their HIV infection and the benefits of their ART regimen.
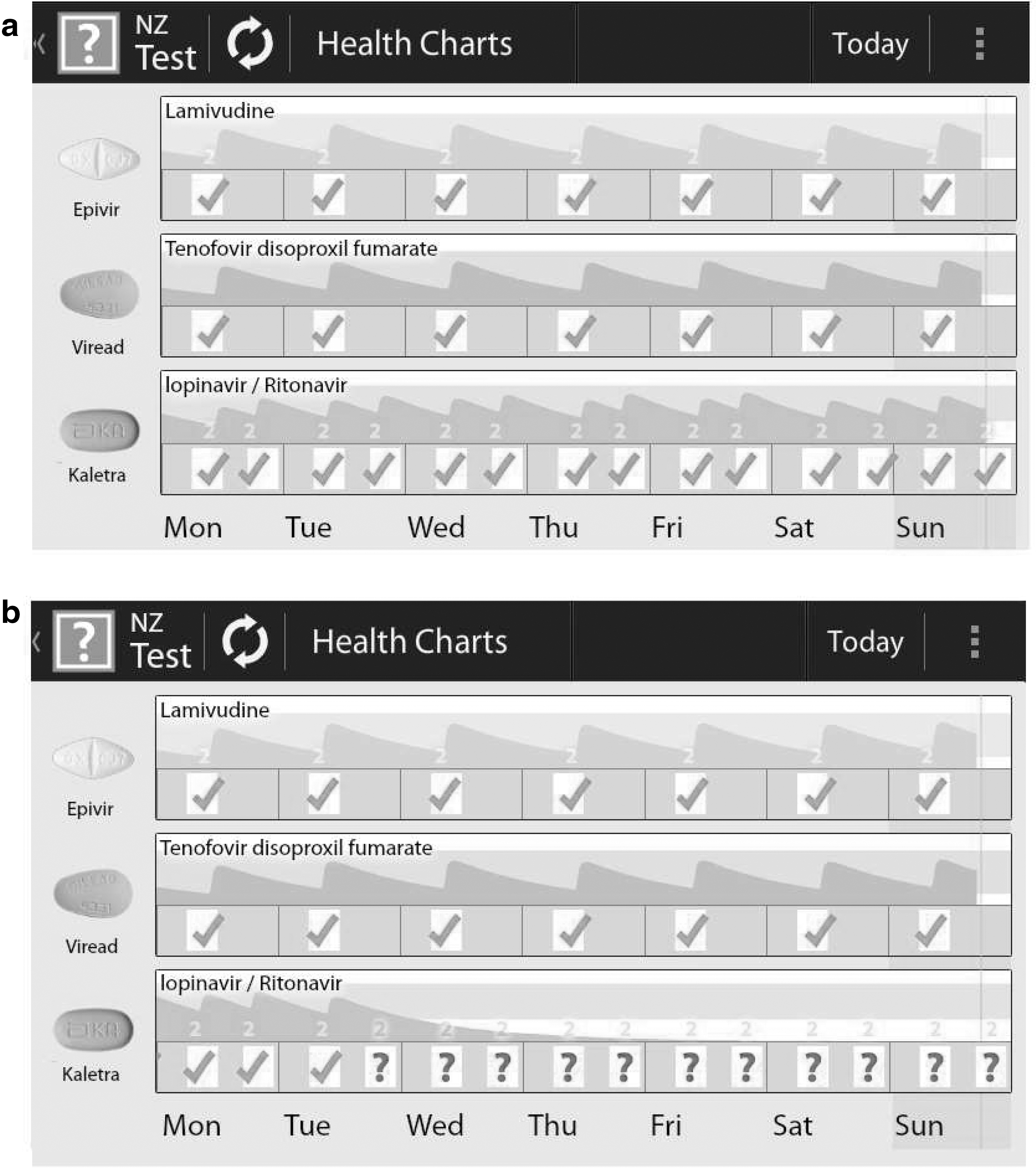
Graphical representations of predicted plasma concentrations of ART medications for
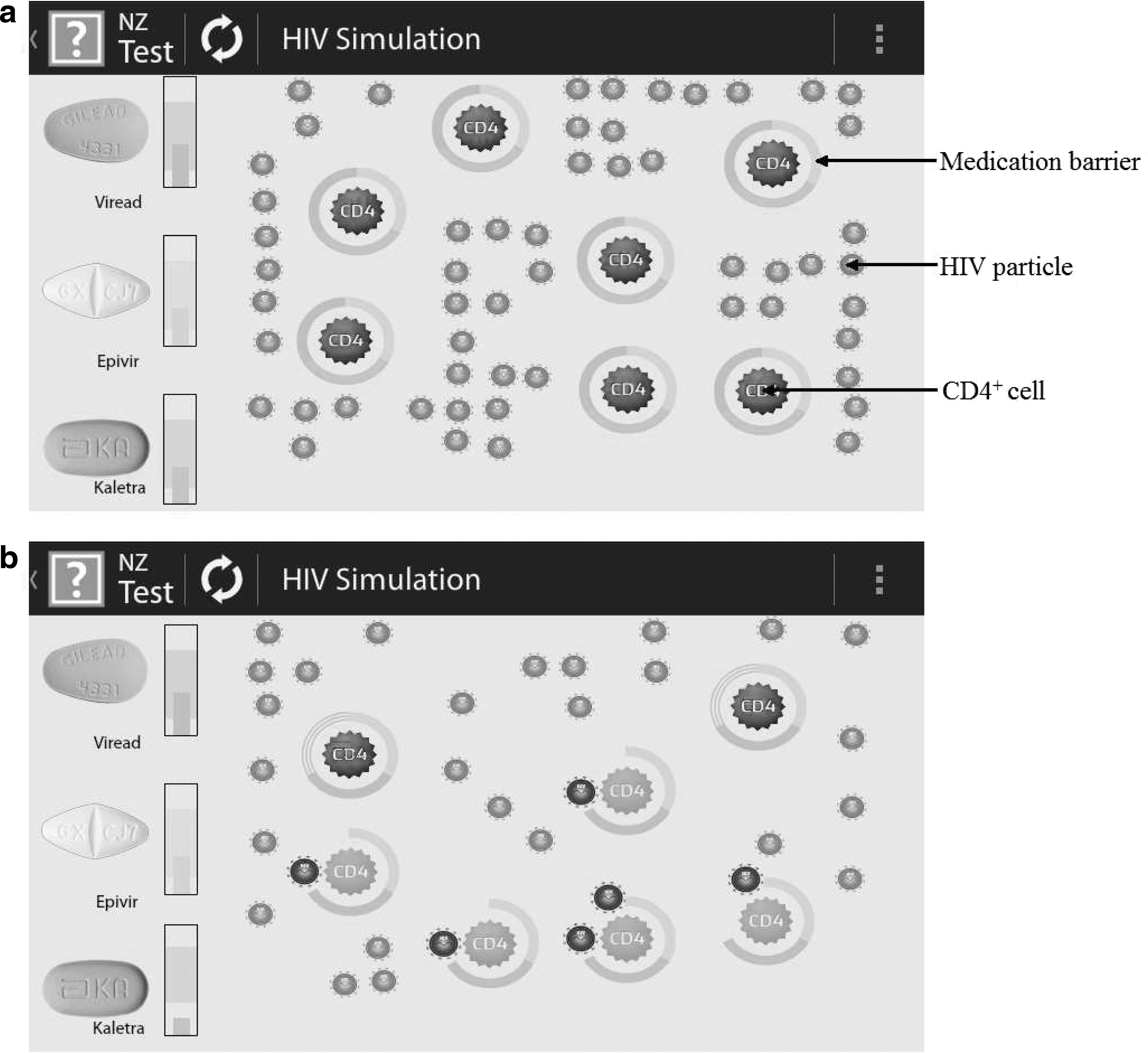
Simulation of the level of protection against HIV replication for
Each participant had their application loaded onto their smartphone during a 1 h appointment with the researcher at Auckland City Hospital. All participants were asked to use their respective application for 3 months. Data were collected at baseline, 1-month, and 3-month follow-up. The study protocol was granted approval by the University of Auckland Human Participants Ethics Committee, the Auckland District Health Board (ADHB) Research Review Committee, and the Massachusetts Institute of Technology Committee on the Use of Humans as Experimental Subjects. The research was also registered with the Australia New Zealand Clinical Trials Registry (Trial ID: ACTRN12613000265774).
Demographic and clinical data
Demographic information (age, gender, ethnicity, sexual orientation, partnership status, education, and income) and relevant clinical data were collected at baseline. Clinical information (year and month of HIV diagnosis, year and month of ART commencement, most recent CD4+ cell count, mode of HIV transmission, and any patient co-morbidities) was obtained for each participant from Auckland City Hospital patient records.
Adherence to antiretroviral therapy
Participant adherence to ART was assessed through the use of objective and subjective methods, namely, self-reported adherence, pharmacy dispensing records, and HIV viral load.
Self-report
Self-reported adherence to ART was assessed using the 9-item Medication Adherence Report Scale (MARS). 24 –26 The wording of the original scale was modified to ask questions with specific reference to ART. Items on the MARS were rated on a 5-point Likert scale ranging from 1 (always true) to 5 (never true). Scores for each item were summed to give a total score ranging from 10 to 50, with higher scores indicating greater reported adherence. Participants were also asked how many doses of ART they had missed over the past 28 days, and the number of doses missed was converted to a percentage figure.
Pharmacy dispensings
The number and dates of dispensings of ART for each participant from January 1, 2012 to September 1, 2013, and the dates of any missed collections, were obtained from local pharmacy records. The number of dispensings collected at baseline and over the study period was converted into a percentage.
HIV viral load
The COBAS AmpliPrep/Taqman HIV-1 test (Roche Laboratories, California), a reverse transcription polymerase chain reaction test with the capacity to quantitate HIV-1 RNA over the range of 20–10,000,000 copies per mL, was used to determine the amount of virus in each participant's blood plasma.
Composite adherence measure
A dichotomous composite adherence measure, incorporating pharmacy dispensings, self-reported adherence, and measures of HIV viral load was also employed. Participants were classified as non-adherent if they either: (a) reported taking less than 95% of prescribed doses of ART; (b) did not collect all of their HIV medications from his or her pharmacy; or (c) had an HIV viral load of more than 20 (>1.3 log10) copies per mL. While successful treatment of HIV infection can be achieved with more moderate adherence, 9,10 greater than 95% adherence is still considered the goal in clinical guidelines. 27
Illness perceptions
The 9-item Brief Illness Perceptions Questionnaire (BIPQ) 28 was used to assess participants' cognitive and emotional illness representations. Items on the BIPQ measured participants' perceptions regarding the chronicity, consequences, controllability, symptoms, emotional effects, and understanding of their HIV infection. All items were rated using an 11-point (0 to 10) response scale with relevant anchors. Higher scores on an item indicated a greater strength of the belief or dimension for the participant.
Medication beliefs
Two questions related to Horne and Weinman's necessity-concern framework were included to assess participants' personal beliefs about ART. 29 These items quantified participants' attitudes about the necessity of their ART regimen (‘How much do you feel you need the medications prescribed for your HIV infection?’), and their concerns about prescribed ART medications (‘How concerned are you about the long-term use of medications prescribed for your HIV infection?’). Each item was rated on an 11-point scale (0 to 10) with relevant anchors. In order to calculate necessity-concern differentials, each participant's concern score was subtracted from their necessity score. A positive necessity-concerns differential indicated that necessity beliefs outweighed reported concerns.
Smartphone application usage
Google Analytics software was used to acquire objective measures of application use. The number of times that each participant viewed each particular component of their application, and the amount of time spent on each component, was assessed at 1- and 2-week follow-up to determine the initial uptake of application use, and at 3-month follow-up to identify any sustained patterns of application use.
Smartphone application evaluation
A questionnaire to evaluate the utility of the smartphone application was also administered. Questions were based on previous research evaluating patient acceptability and satisfaction with mhealth interventions. 30,31 Participants were asked how satisfied they were with the application and how useful they found each component for reminding them to take their medications. The questionnaire also enquired about specific properties of the application, namely: ease of use, visual appeal, discretion, and information provision. Participants were also asked to give the smartphone application an overall rating. Each item was rated on an 11-point scale (0 to 10) with relevant anchors. Higher scores on an item indicated a more positive response.
Statistical analyses
The data were analyzed using the SPSS version 20.0 software (Chicago, Illinois). Data were assessed for normality, and nonparametric testing was employed for analysis of variables that did not have a normal distribution. One-way analyses of covariance (ANCOVAs), controlling for baseline measures of the outcome variable, were used to examine the effects of the intervention on adherence to treatment, perceptions of HIV infection, and beliefs about ART. McNemar's tests were conducted to ascertain if there were any differences in the proportion of non-adherent participants (as classified using the composite adherence measure) at baseline and 3-month follow-up, in the intervention and active control group. Correlational analyses were used to explore the relationships between application use, changes in illness perceptions and medication beliefs, and changes in adherence to ART. Independent samples t-tests were carried out to assess the effect of group allocation on application usage and evaluations of the smartphone application.
Results
A total of 28 adults with HIV infection (26 men, 2 women) took part in the trial. The average age of participants was 46, with ages ranging from 30 to 65 years. The sample was predominantly male (93%) and homosexual (86%), with the majority of participants identifying as New Zealand European (54%). The average length of time since diagnosis of HIV infection was 11 years, and the average time since initiation of ART was 8 years. The majority of participants (54%) were prescribed a antiretroviral treatment regimen composed of two nucleoside analogue reverse transcriptase inhibitors and one non-nucleoside reverse transcriptase inhibitor. There were no significant differences between the active control and intervention groups at baseline with regard to demographic (ps>0.14) and clinical characteristics (ps>0.49), illness perceptions (ps>0.16), medication beliefs (ps>0.30), and psychological distress (ps>0.08). Similarly, there were no significant between-group differences at baseline with respect to any adherence variables (ps>0.60).
Examination of MARS scores to examine self reported adherence revealed that the intervention group had significantly higher self-reported adherence to ART, when compared to the active control group F(1,23)=5.37, p=0.03, ηp 2 =0.19 (Table 1). Similar analyses conducted with the percentage of prescribed doses of ART taken, F(1,23)=1.41, p=0.25, ηp 2 =0.06, and pharmacy dispensing data, F(1,25)=1.88, p=0.18, ηp 2 =0.07, revealed no significant differences between the active control and intervention groups at 3-month follow-up. Examining HIV viral load, we found the intervention group had a significantly lower HIV viral load at 3-month follow-up, compared to individuals in the active control group F(1,23)=5.62, p=0.023, ηp 2 =0.20. In the intervention group, the proportion of participants with a detectable HIV viral load (>20 copies of HIV RNA per mL) decreased from 26% at baseline to 7% at the 3-month follow-up. No such change was evident in the active control group where the proportion of participants with a detectable HIV viral load increased from 18% at baseline to 37% at the 3-month follow-up.
MARS, Medication Adherence Report Scale.
Employment of a dichotomous composite measure of adherence highlighted a significant reduction in the percentage of participants who were classified as non-adherent in the intervention group between baseline (53%) and 3-month follow-up (13%), X 2 (1, n=15)=6.00, p= 0.03. Within the active control group, there was no change from baseline (27%) to 3-month follow-up (27%) in the percentage of participants classified as non-adherent, X 2 (1, n=11)=0.00, p>0.99.
There were no significant differences between the intervention group and the active control group with regard to any illness perceptions or medication beliefs, at either the 1-month or 3-month follow-up. However, greater levels of engagement with the augmented application appeared to drive changes in participants' conceptualizations of their HIV infection and ART regimen. Within the intervention group, greater use of the graphs of predicted medication concentrations was associated with improvements in participants' perceived understanding of HIV infection with regard to both time, rtime =0.58, n=15, p=0.02, and frequency metrics, rfrequency =0.65, n=15, p= 0.01. Similarly, greater use of the simulation of immune activity was significantly associated with improvements in participants' perceived understanding of their HIV infection, rfrequency =0.60, n=15, p=0.02, increases in the perceived necessity for ART, rtime =0.53, n=15, p=0.04, and positive changes in necessity-concern differentials, rtime =0.56, n=15, p=0.03; rfrequency =0.52, n=15, p=0.04. These associations were apparent 1 month after participants started using the application but were not maintained at 3-month follow-up, perhaps indicating that changes in these cognitive factors were driven by participants' initial level of engagement with the augmented application.
At the 1-month follow-up point, individuals in the intervention group rated their augmented application as significantly more informative, more visually appealing, and a more effective source of motivation to take their ART medications, when compared to ratings of the standard application reported by the active control group (Table 1) Participants in the intervention group were also significantly more satisfied with their smartphone application and gave it a significantly higher overall rating. Significant differences with regard to satisfaction ratings and information provision were maintained at 3 month follow-up (Table 2).
Significant differences are in
The majority of participants in the intervention group (81%) stated that they would recommend the augmented application to other people on treatment for HIV infection. It was suggested that the application would be particularly useful for individuals who had recently initiated ART and for those with low English literacy. With regard to future improvements, many participants (79%) reported that the addition of an alarm function would be useful for encouraging adherence.
Discussion
The study found that an augmented smartphone application that provided real time information about the level of medication in the patient's body and a personalized pictorial representation of the current level of immunoprotection improved adherence to ART compared to a control smartphone application. Participants who received the augmented application displayed a significantly higher level of self-reported adherence to ART and lower HIV viral load at 3-month follow-up, in comparison to individuals who received the standard version. Further, there was a significant decrease from baseline to 3-month follow-up in the proportion of participants classified as non-adherent in the group who used the augmented version. Greater use of the extra components of the augmented application was associated with improvements in the perceived understanding of HIV infection and perceived necessity for ART. Compared to the standard version, the augmented application was rated as a significantly more effective source of motivation to take ART and was given a higher overall rating.
While this is a novel area of research, the results of this study support the growing body of literature that endorses the use of mHealth interventions for self-management of chronic illnesses. 23,32 Specifically, the improvements in self-reported adherence and HIV viral load, as well as the significant reduction in non-adherent participants within the intervention group, indicate that the application tested in the current study can be used to enhance adherence to ART among people living with HIV. These findings are consistent with the results of a few recent studies which have successfully utilized mobile-based interventions to facilitate adherence to ART. 33 –35
The current research highlights that a smartphone intervention based on the Common Sense Model of self-regulation 17 and incorporating personalized health-related visual imagery can modify patients' conceptualisations of their HIV infection and improve adherence to ART. Thus, in addition to highlighting that illness perceptions and medication beliefs can be used to understand patient adherence, the findings of this study provide empirical evidence that an adherence-promoting intervention based on these frameworks can be used to change patient behavior. It is notable that changes in patients' perceived understanding of the illness and perceived necessity for ART appear to be driven by greater engagement with the smartphone application in terms of the greater use of the simulation of immune activity in the augmented version. The results of this study suggest benefits can be obtained through mobile interventions which solely target the cognitive determinants of non-adherence.
Interventions delivered through mobile technologies can be accessed by the patient in their natural environment and in real-time, thus making medication-taking more salient to the individual and encouraging adherent behaviour. 36 The interactive nature of the intervention tested in the current study may also aid in increasing the patient's awareness of their ART regimen and medication-taking routine. 34 The results of the current study also indicate that exposure to the extra visual components of the augmented application resulted in modification of participants' conceptualizations of their HIV infection and ART regimen. Thus, while the interactive nature and real-world integration of the augmented application is conducive to optimal adherence, it appears that the changes in illness perceptions and medication beliefs are especially facilitated by the delivery of personalised health-related visual imagery and the provision of real-time feedback. 15,30,37
The findings of the current study support the dissemination of the augmented application as a tool to help people with HIV infection adhere to their treatment regimens. The high level of acceptance and satisfaction with the augmented application reported by participants demonstrates that this intervention has considerable utility among an HIV-infected population. Given that disclosure of seropositive status is a concern for many people living with HIV infection, it is important that the augmented application was rated by people on ART as being discreet with regard to HIV-related information. Furthermore, the cost-effectiveness of mobile technologies means that the implementation of such an intervention is feasible in the clinical setting.
This study was limited by the characteristics of the sample. Participation was restricted to people on ART who used a smartphone with an Android operating system. The participants were also not new to ART treatment, so it could be argued that the effect of the intervention may have been underestimated in this sample. In an effort to gauge the level of adherence in each group we employed a dichotomous measure of adherence composed of self-reported adherence, pharmacy dispensing, and viral load. It should be acknowledged that occasionally there may be reasons other that non-adherence for detectable viral load. Furthermore, a large proportion of the sample exhibited maximum scores for each adherence variable at baseline and continued to do so at the 3-month follow-up, making it difficult to ascertain any intervention-related differences in adherence between the intervention group and active control group. Even so, the results demonstrate meaningful and significant improvements in adherence to ART in the intervention group with regard to measures of HIV viral load and self-reported adherence. A further randomized controlled trial with a larger sample size, across more operating systems, and conducted over a longer period of time would be useful in ascertaining whether the improvements in adherence to ART observed can be maintained in the long-term. Previous research has identified that in order to have maximal benefit, interventions should fit with the patient's stage of adherence to their medication. 38 It is likely that the application may have most utility in patients who are new to ART therapy or are having particular problems with adherence as these individuals are more likely to have an incomplete understanding of the relationship between medication adherence and control of their HIV infection. 11,39,40
Footnotes
Acknowledgments
The smartphone application used in this study was delivered using the open source CollaboRhythm software platform. The development of this open source platform was supported in part by NIH grant R01DA031081-010A1 (Edward W. Boyer, Principal Investigator).
Author Disclosure Statement
No competing financial interests exist.