
Abstract
Renal disorders are an emerging problem in HIV-infected patients. We performed a cross-sectional study of the first 1000 HIV-infected patients attended at our HIV unit who agreed to participate. We determined the frequency of renal alterations and its related risk factors. Summary statistics and logistic regression were applied. The study sample comprised 970 patients with complete data. Most were white (94%) and men (76%). Median (IQR) age was 48 (42–53) years. Hypertension was diagnosed in 19%, dyslipidemia in 27%, and diabetes mellitus in 3%. According to the Chronic Kidney Disease Epidemiology Collaboration (CKD EPI) equation, 29 patients (3%) had an eGFR<60 ml/min/1.73 m2; 18 of them (62%) presented altered albumin/creatinine and protein/creatinine (UPC or UAC) ratios. Of the patients with eGFR>60 mL/min, it was present in 293 (30%), 38 of whom (7.1%) had UPC>300 mg/g. Increased risk of renal abnormalities was correlated with hypertension (OR, 1.821 [95%CI, 1.292;2.564]; p=0.001), age (OR, 1.015 [95%CI, 1.001;1.030], per one year; p=0.040), and use of tenofovir disoproxil fumarate (TDF) plus protease inhibitor (PI), (OR, 1.401 [95%CI, 1.078;1.821]; p=0.012). Current CD4 cell count was a protective factor (OR, 0.9995 [95%CI, 0.9991;0.9999], per one cell; p=0.035). A considerable proportion of patients presented altered UPC or UAC ratios, despite having an eGFR>60 mL/min. CD4 cell count was a protective factor; age, hypertension, and use of TDF plus PIs were risk factors for renal abnormalities. Based on our results, screen of renal abnormalities should be considered in all HIV-infected patients to detect these alterations early.
Introduction
A
Regarding the HIV-infected population, the chronic and end-stage kidney diseases have diminished due to the improvement of immunological status, although renal alterations still remain as a problem. 7,8 Renal chronic disease is three times more prevalent than in the general population. 9,10 However, the real frequency of renal abnormalities has been reported to range from 1% to 30%, depending on the characteristics of the study population (e.g., race, age, and co-morbidities) 11 –13 and the definition of the abnormality evaluated (e.g., chronic kidney disease or signs of renal damage, that is, presence of proteinuria, albuminuria, or other signs of altered urine markers) in the absence of altered estimated glomerular filtration rate (eGFR).
Some of the factors associated with kidney alterations in HIV-infected patients are common to the general population, including, age, arterial hypertension, diabetes, use of potentially nephrotoxic drugs, and hepatitis co-infection; however, other factors are specific to HIV infection, such as low CD4 cell count, high HIV plasma viral load, or use of some antiretroviral drugs [e.g., tenofovir disoproxil fumarate (TDF)]. 13 –15 As is usual in several co-morbidities, age is a factor at risk to developed or worsened renal disease. 16
Renal disease has several clinical manifestations, from subclinical forms of renal damage, to decreased GFR or renal failure at end stages. 11 On the other hand, the relevance of renal damage in the HIV-infected population can be seen in the independent association between microalbuminuria and AIDS-related death (HR, 2.3; 95%CI, 1.3–4.3). Furthermore, patients with proteinuria are at increased risk for non–AIDS-related death (HR, 2.4; 95%CI, 1.2–4.6). 17,18 Finally, cardiovascular events are a frequent cause of non-AIDS mortality in this population. 19
The principal aim of this study was to determine the real prevalence of kidney abnormalities and related factors in our setting by assessing a large cohort of HIV-infected patients attending a tertiary hospital in Spain for routine clinical control of HIV infection.
Methods
We performed a cross-sectional study of the first 1000 HIV-infected outpatients who attended our HIV Unit and agreed to participate. All the patients signed an informed consent document. The study was approved by the Institutional Ethics Committee of the coordinating center and the local health authorities. The study period was started at January 2011, and the last patient was included in December, 2012.
A questionnaire was prospectively completed by all the patients to obtain data on personal and family history of diabetes mellitus, dyslipidemia, hypertension, cardiovascular events, renal or liver disease, previous or current syphilis, use of potentially nephrotoxic drugs (e.g., angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, cyclosporine, nonsteroidal anti-inflammatory drugs, and tacrolimus), physical exercise, and the consumption of tobacco products, alcohol, and drugs of abuse.
Demographic and HIV-related data were collected from the patient's clinical records, as follows: sex, age, risk factors for HIV infection, clinical stage, time since HIV diagnosis, time with suppressed viral load, previous and current antiretroviral treatment, time on antiretroviral treatment, time on tenofovir, time on protease inhibitors, and hepatitis co-infection. Immunologic and virological data were also recorded, including current viral load, CD4 and CD8 T-cell count, peak viral load, and nadir CD4 T-cell count.
Blood and urine samples were collected in fasting conditions. Serum creatinine and phosphate were determined. Estimated GFR was calculated using the Modification of Diet in Renal Disease equation (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD EPI) equations.
Normal local reference values were as follows: eGFR, >60 mL/min/1.73m2; serum creatinine, <1.20 mg/dL; and serum phosphate, 2.5–4.50 mg/dL. Kidney disease was defined as an eGFR<60 ml/min/1.73m2 and graded according to the Kidney Disease Outcomes Quality Initiative (KDOQI) classification. 20 Renal damage was defined as the presence of micro- or macro-albuminuria, or proteinuria, by albumin/creatinine and protein/creatinine ratios (UAC or UPC ratios), or glucosuria, hematuria, or hipophospatemia. The normal values for UPC and UAC ratios were <200 and <30 mg/g, respectively. Subsequently, these ratios was categorized as <30, 30–300, or >300 mg/g.
Body mass index (BMI) was calculated, and arterial blood pressure was measured three times with the patient resting. Arterial hypertension was defined as a systolic blood pressure of ≥140 mmHg, diastolic blood pressure of ≥90 mmHg, or the need for antihypertensive agents. In case of high readings, patients were followed up to confirm or rule out the diagnosis of arterial hypertension. Diabetes was defined as persistent fasting glycemia >100 mg/dL or the need for antidiabetic agents. Dyslipidemia was defined as triglycerides >150 mg/dL, total cholesterol >200 mg/dL, LDL cholesterol >130 mg/dL, or the need for lipid-lowering drugs.
Statistical analyses
Patient characteristics were described using the mean (SD), median (IQR), and frequency (%), as appropriate.
Univariate and multivariate logistic regression analyses were performed to evaluate risk factors that might influence renal abnormalities (alteration in eGFR or signs of renal damage).
The predictor variables used in the regression models were age, smoking, gender, diabetes mellitus, arterial hypertension, BMI, dyslipidemia, time since diagnosis of HIV, use of potentially nephrotoxic drugs, nadir and current CD4 T-cell count, months on antiretroviral treatment, type of antiretroviral agent, use of TDF and of TDF plus protease inhibitors (PIs), time on protease inhibitors, and time on TDF. Variables were included in the multivariate model in such a way as to avoid multicollinearity using a stepwise procedure.
All analyses were performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA). All tests were two-sided, and p values<0.05 were considered statistically significant.
Results
We offered to participate in the study to all the patients visited in our AIDS Care Unit. A total of 37 subjects refused to participate. The main reason to refuse was they did not have enough time to complete the survey. We recruited the first 1000 patients who attended the HIV Unit and accepted to participate. Of these, 30 were subsequently excluded from the analysis because of missing data. Most of the remaining 970 patients were white (94%) and men (76%), with a median (IQR) age of 48 (42–53) years. A history of arterial hypertension was self-reported by 9% (in the questionnaire), but was diagnosed in 19% of patients by means of repetitive measurements and subsequent clinical evaluation. Dyslipidemia was diagnosed in 27% and diabetes mellitus in 3%. Treatment with antihypertensive agents was taken by 87 patients (9%), lipid-lowering agents by 142 (4.3%), and hypoglycemic agents by 26 (2.7%) (Table 1).
ARV, antiretroviral; BMI, body mass index; IQR, interquartile range; n, number of patients; PI, protease inhibitors; TDF, tenofovir; UAC ratio, urine albumin creatinine ratio; UPC ratio, urine protein creatinine ratio. Data are expressed as the median (IQR) unless otherwise indicated.
Grade of UAC or UPC are irrespective to the e GFR.
Estimated glomerular filtration rate and classification according to KDIGO criteria
The median (IQR) eGFR according to the CKD EPI equation was 101 (89.5; 108.2) mL/min per 1.73 m2.
According to the 2012 KDIGO criteria, CKD parameters were normal in 507 patients (52.3%) (eGFR>90 mL/min/1.73 m2 with no signs of renal damage). Stage 1 CKD was recorded in 213 patients (22%, eGFR>90 mL/min/1.73 m2 with signs of renal damage), stage 2 in 221 patients (22.8%, eGFR>60–90 mL/min/1.73 m2), and stage 3 in 27 patients (2.8%, eGFR<60 mL/min/1.73 m2). One patient (0.1%) had stage 4 CKD (eGFR between 15–30 mL/min/1.73 m2), and 1 patient (0.1%) had stage 5 disease (eGFR<15 mL/min/1.73 m2) (Fig. 1).
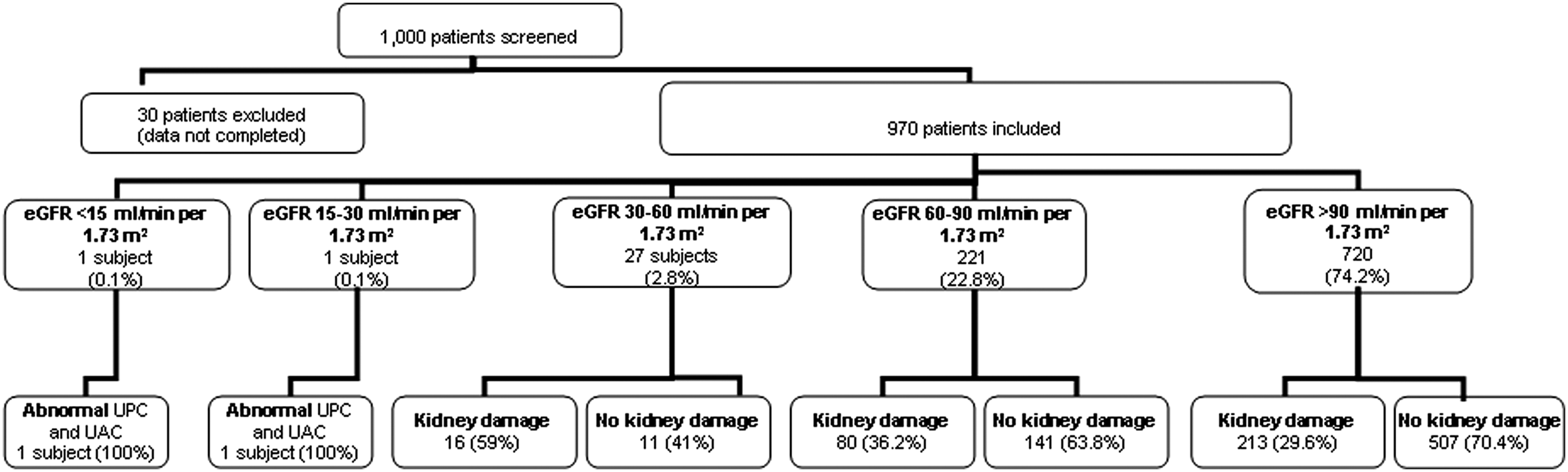
Flow chart. eGFR: estimated glomerular filtration rate; kidney damage: altered albumin/creatinine and protein/creatinine ratios (UPC or UAC ratios), or presence of glucosuria, hematuria or hipophospatemia; UPC or UAC ratios: urinary proteinuria/creatinine or albuminuria/creatinine ratios.
Data were very similar for the MDRD equation: 39 patients (4%) had an eGFR<60 mL/min/1.73 m2, 1 patient (0.1%) had <15 mL/min/1.73 m2, 1 patient (0.1%) had 15–30 mL/min/1.73 m2, and 37 patients (2.8%) had 30–60 mL/min/1.73 m2.
Signs of renal damage according to eGFR
Overall, signs of renal damage (abnormal UPC, UAC, hypophosphatemia, glucosuria, hematuria, or all), was present in 311 of the patients (32%). With regard to the eGFR, of the 29 patients with eGFR (CKD-EPI)<60 mL/min/1.73 m2, 18 (62%) presented any sign of renal damage. Of those with eGFR>60 mL/min/1.73 m2, renal damage was present in 297 (30%). Indeed in the case of a normal function (eGFR>90 mL/min/1.73 m2), signs of renal damage are present in 213 patients from 720 (29.6%). Specifically, abnormal UPC or UAC ratios (UPC>200 mg/g and/or UAC>30 mg/g) was detected in 75 (7.8%) and 58 (6%) patients, respectively.
Considering only those patients with abnormal UPC or UAC ratios, median values for the albumin/creatinine and protein/creatinine ratios were 54.8 (38.7;91.05) mg/g and 309 (246;470) mg/g, respectively.
Seventy seven patients (8%) had UAC ratio <30 (median [IQR], 0.9 [0.07;10]) mg/g, and 38 patients (4%) had UPC or UAC ratios >300 (467 [351;887.75]) mg/g.
Related factors
Logistic regression was performed in two cases: altered eGFR and/or abnormal UPC or UAC ratios and normal eGFR and in case of proteinuria >300 mg/g. The results from the univariate and multivariate analyses are summarized in Table 2.
BMI, body mass index; eGFR, estimated glomerular filtration rate; PI, protease inhibitor; NRTIs, nucleoside reverse transcriptase inhibitors; TDF, tenofovir; UPC, urine protein/creatinine ratio; UAC, urine albumin/creatinine ratio.
Multivariate regression from the first model showed associations between an increased risk of abnormal UPC or UAC ratios and: hypertension [OR 1.821, (95%IC: 1.292; 2.564), p=0.001], age [per 1 year, OR 1.015, (95%IC 1.001;1.030), p=0.040], BMI bellow 18 or above 30 kg/m2 [OR 2.1277, (95%IC:1.335; 3.39), p=0.001] and use of TDF plus PI, [OR 1.401, (95%IC:1.078;1.8215), p=0.012)]. Current CD4 cells count [per one cell of increase, OR 0.9995, (95%IC 0.9991;0.9999), p=0.035] was a protector factor.
In the multivariate analysis of the second model, the only variables associated with proteinuria >300 mg/g were diabetes mellitus (p=0.018) and arterial hypertension (p=0.007).
Logistic regression analysis based on the MDRD equation revealed similar risk factors to the analysis based on the CKD-EPI equation (data not shown).
Discussion
The main findings of our cross-sectional study were a low percentage of patients with renal disease (eGFR<60 mL/min/1.73 m2) but, importantly, the high prevalence of signs of kidney damage, in patients with an eGFR>60 mL/min/1.73 m2 and even with normal eGFR (>90 mL/min/1.73 m2). This finding has important clinical implications for the management and control of the HIV population and led these patients as an at risk population. In addition, we also detected that arterial hypertension was an underdiagnosed risk factor in our cohort.
Consistent with findings of other HIV-infected populations in the same geographical area, advanced renal disease was infrequent in our study (0.2%). Results from European cohorts show a prevalence of kidney disease (eGFR<60 mL/min/1.73 m2) to be 2–5%. 21 –23 The relatively low median age (48 years) of our patients likely explains this finding. However, the high prevalence of patients with signs of renal damage, most of whom had an eGFR>60 mL/min/1.73 m2 is similar to other results recently reported elsewhere, 21 and, contrary, is lower than others regarding the proportion of proteinuria detected. 23 Interestingly, these others signs of renal damage (no only AUC or UPC altered) could appear earlier than proteinuria in the case of renal alteration, and this is a possible explanation of the differences in the results regarding the distinct parameters evaluated. it should be take in consideration in order to early detect and manage this alterations, even when a normal eGFR is present.
The relevance of abnormal UPC or UAC ratios is strongly associated with cardiovascular events and death in the general population, irrespective of the grade of albuminuria or proteinuria. 5 A recent meta-analysis of more than 170,000 patients from 26 cohort studies concluded that patients with abnormal UPC or UAC ratios (even those with <30 mg/g) have a ≥50% greater risk of coronary heart disease than those without proteinuria. 3 In the HIV-infected population, recently published articles report a correlation between microalbuminuria/proteinuria and a two-fold increased risk of both AIDS- and non–AIDS-related mortality. 18,24 Consequently, HIV-infected patients should be considered a risk population and renal damage should be assessed, even in patients without other risk factors (e.g., age >60 years, arterial hypertension, and diabetes mellitus). 25
Also relevant is the considerable number of new diagnoses of arterial hypertension in our patients. Given that hypertension is a well-established risk factor for renal damage, blood pressure should be assessed routinely in the HIV-infected population. Metabolic abnormalities such as diabetes mellitus, dyslipidemia, and arterial hypertension are progressively more frequent, and clinical monitoring of these risk factors is increasingly relevant.
Many of the factors associated with altered eGFR and proteinuria were common to those observed in the general population (such as extreme BMI or older age), supporting data from previous studies. 26,27 We expect an increase of renal disturbances in the next future among HIV-infected people due to their improvement of life expectancy. In fact, aging is related not only with an increased incidence of renal disease but also with an increased incidence of other co-morbidities. 16
However, in contrast with findings reported elsewhere, 13 –15 viral load was not associated with an increase in the risk of kidney disease or proteinuria in our study, probably because of the viral suppression and preserved immune status (a protective factor) recorded in the most of our patients, which reduced the impact of HIV-related factors on renal alterations.
Tenofovir has been associated with tubular injury, 28 and proximal renal tubulopathy is the most common histopathology finding; 29 in contrast, altered GFR and advanced renal disease due to tenofovir seem to be infrequent. 30,31 Our data showed that the use of tenofovir combined with a protease inhibitor increased the risk of kidney disease (abnormal eGFR and abnormal UPC or UAC ratios), as previously described in large cohorts. 15,22,32 Higher tenofovir plasma concentration was associated with alterations in renal markers (both glomerular and tubular), 33,34 and the highest plasma exposure was associated with the concomitant use of protease inhibitors. 35 However, whether co-administered or not with protease inhibitors, tenofovir was not associated with proteinuria >300 mg/g in our cohort. In fact, the most common form of TDF-related toxicity is a low level of proteinuria, 27 that is usually reversible after the interruption of the drug. 36
Our study has several limitations. First, its cross-sectional design could lead us to overestimate the prevalence of renal abnormalities, because of only one determination of blood and urine was collected. Second, the cross-sectional design is unable to evaluate the evolution of the renal alterations detected. Finally, since we included mainly white men, our results cannot be extrapolated to other populations. Nevertheless, our study provides a reasonable picture of renal damage in the HIV-infected population in our setting.
In conclusion, severe kidney disease (eGFR<60 mL/min/1.73m2) was infrequent in our cohort; in contrast, signs of renal damage (mostly altered UPC or UAC ratios) were highly frequent, despite a normal eGFR. These data highlight the susceptibility of this population, and the need for early detection of renal injury, even in patients with normal renal function. In addition to HIV-related factors, factors common to the general population (e.g., age, arterial hypertension, diabetes, and extreme BMI) emerge as potentially major risk factors of renal damage.
Footnotes
Acknowledgments
We are grateful to Thomas O'Boyle for editorial assistance.
Author Disclosure Statement
Conflicts of interest: AB has received fees from VIIV, Jansen Cilag, Abbott, and Roche; PE has received personal fees from VIIV, Jansen Cilag, and Abbott; EN and BC have received personal fees from VIIV, Merck, Jansen Cilag, Abbott, Roche, and Boehringer Ingelheim. The remaining authors report no competing interests.
No financial support was received for this study.