
Abstract

Dear Editor:
A
HIV-infected patients in Taiwan have been provided with free antiretroviral therapy and medical care at AIDS-designated hospitals since the early 1990s. An estimated 70% of individuals living with HIV infection in Taiwan have sought HIV care, and 40% of individuals who have sought HIV care received HAART after the diagnosis of HIV infection with CD4 cell counts <350 cells/mm. 3,4 In 2005, the Taiwan Center for Disease Control (Taiwan CDC) initiated an HIV case management (CM) program in AIDS-designated hospitals to provide integrative services and risk reduction counseling for HIV-infected individuals. The current study provides a unique opportunity to observe the impact of HIV case management on achieving the optimal therapeutic effect of HAART among HIV-infected persons.
A longitudinal prospective cohort study was conducted at an AIDS-designated hospital, National Cheng Kung University Hospital (NCKUH), with over 15 years of experience caring for HIV-infected patients in southern Taiwan. A total of 549 patients who were newly diagnosed during 2008–2012 provided data for analysis. Of the 549 patients, 427 (77.8%) ever enrolled in the hospital-based HIV case management program. Retention in care was defined as having two or more HIV clinical visits separated by ≥90 days during a calendar year over the 5-year observation period. 5 Achievement of viral suppression was defined as the first HIV RNA level of <400 copies per milliliter, and time to viral suppression was defined as the number of days between the initial diagnosis of HIV and the first viral load (VL) of <400 copies per milliliter. 6 Patients who never had a VL >1000 copies per milliliter after viral suppression (VL <400 copies per milliliter) by the time of death or at the end of the analysis period were considered to have maintained suppression.
Of the 549 patients, the mean age was 31.6 years (SD 9.7, range: 16–77 years), 95.3% were male, and 69.2% reported men having sex with men (MSM) as a primary risk factor for HIV transmission. Median initial CD4 count during the year rose from 55.2 to 185.9 cells/mm3. Applying the pre-2013 HAART initiation threshold of CD4 <350 cells per cubic millimeter, 52–60% would have been eligible to begin HAART based on the first CD4 after the initial diagnosis. Almost two-thirds (n=335, 72.2%) of the patients were retained in care until the end of the 5-year study period. The adjusted multivariate logistic regression indicated that persons retained in HIV care were significantly more likely to be female [adjusted odds ratio (aOR) 0.25, 95% confidence interval (CI): 0.75–0.84], to have initiated HAART (aOR 4.91, 95% CI: 2.81–8.60), and to be enrolled in the case management program (aOR 2.15, 95% CI: 1.11–4.16) than persons not retained in care during years 2008–2012.
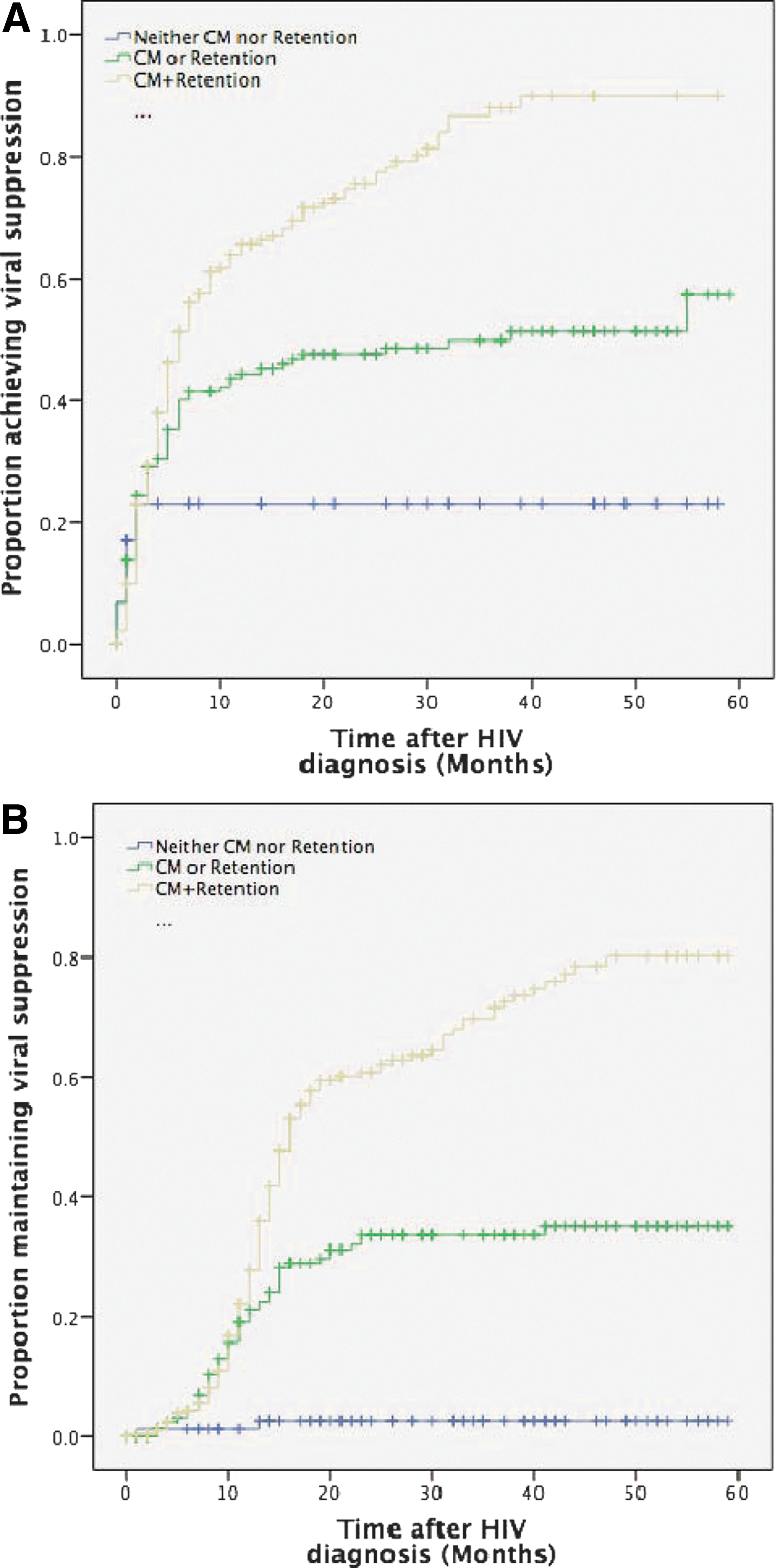
Overall, 257 (61.8%) of the patients newly diagnosed with HIV during 2008–2012 ever achieved viral suppression by the end of 2012; 26.6% achieved suppression within 6 months of diagnosis, and 39.8% within 12 months. Overall, 57.6% of the 257 persons who ever achieved viral suppression maintained their suppression for 12 months. Cox proportional hazards models showed significant interaction effects between retention in care and enrollment in CMP on viral suppression (Table 1).
Excluding death and transfer cases
95% CI, 95% confidence interval; CMP, case management program; LL, lower limit; UL, upper limit.
The patients were divided into three groups: retained in care plus case management (n=294, 53.6%), either retained in care or enrolled in case management only (n=174, 31.4%), and irregular/lost to follow-up and also without case management (n=81, 14.8%). The Kaplan-Meier survival analysis showed that patients who were retained in care and also enrolled in CMP had the best outcomes of achieving viral suppression (p<0.001) (Fig. 1A) and maintaining viral suppression for 12 months (p<0.001) (Fig. 1B), followed by those either retained in care or enrolled in CMP. Patients who either attended irregularly or were lost to follow-up and were not enrolled in the case management program had worse outcomes.
Proportion of patients
Our study showed that 61.8% of patients newly diagnosed with HIV during 2008–2012 had ever achieved viral suppression. Consistent with previous studies, persons belonging to a more recent diagnostic cohort 6 and those with earlier initiation of HAART since diagnosis held an advantage in entry to care 7 and consistently improved in terms of the proportions who achieved and maintained viral suppression. Poor retention in HIV care as a barrier to achieve and maintain viral suppression, 8 failure to achieve, and sustain viral suppression poses an increased risk of HIV transmissibility. 9 This suggests that persons not retained in care and not virally suppressed may be in need of targeted prevention interventions.
The current study advances earlier research by indicating that case management is an effective strategy to increase retention and, consequently, to achieve and maintain virological suppression in the HAART era. We found that patients receiving HIV CMP were significantly more likely to be retained in care, which is similar to research that found that patients receiving care at medical case management (MCM)-funded facilities were >4 times as likely to be retained in care but equally likely to be virally suppressed when compared with persons at non
During 2008–2012, 72.2% of patients in this study maintained a higher retention rate in HIV care compared with previous studies of other clinic-based cohorts in the US: 67% with 6-year retention at the University of North Carolina Center for AIDS Research 10, 66% in Denver metropolitan area 11 across a 5-year period, and an estimated 59% across the United States from 6 months to 3–5 years. 12 Our study revealed that patients who were retained in care had the best outcomes; they were 5.19 times more likely to achieve viral suppression and 17.16 times more likely to maintain viral suppression than those who were not retained in care. Strategies to retain HIV-infected persons in long-term care must be developed to maximize the benefits of treatment outcomes.
In conclusion, 72.2% of patients newly diagnosed with HIV were retained in HIV care during 2008–2012, 61.8% ever achieved viral suppression and 57.6% of persons who ever achieved viral suppression maintained their suppression for 12 months. Patients who were retained in care and also enrolled in a case management program had the best outcomes for achieving and maintaining viral suppression. The significant interaction between case management and retention in care on viral suppression and survival complements earlier research and provides novel insight into the positive impact of the case management model on retention and long-term treatment outcomes.
Footnotes
Acknowlegments
This study was supported by grants (NSC 102-2314-B-006 -057 -MY2, 2013–2014) from Ministry of Science and Technology, Executive Yuan, Taiwan. The authors would like to thank all participants in the study.
Author Disclosure Statement
All authors report no conflicts of interest relevant to this article.