
Abstract
In the United States, rates of HIV infection are highest among black men who have sex with men (BMSM). Pre-exposure prophylaxis (PrEP) is a highly effective form of HIV prevention, but the uptake of this strategy has been slow since FDA approval in 2012, and it is unknown whether information about PrEP is reaching BMSM. Four hundred and thirty-six BMSM in Atlanta, GA were surveyed from January 2012 (6 months prior to PrEP approval) to March 2014 (20 months after approval). Analyses revealed no association between date of survey assessment and awareness of PrEP (20.5% were aware of PrEP before approval and 23.4% were aware after approval; OR=0.99 [0.98–1.02], p=0.952). In a multivariate model, BMSM unaware of PrEP reported lower rates of HIV testing knowledge, fewer experiences with HIV testing, and higher rates of transactional sex than BMSM who were aware of PrEP. Our findings suggest that there is limited understanding of PrEP and that there is considerable groundwork that needs to be achieved in order to reap the full benefits of PrEP. The current findings call attention to the need to both prioritize and better understand how to strengthen the bridge between medical advances and community uptake.
Introduction
I
In the state of Georgia, the location of the current study, the prevalence of HIV is twice the national average. 7 Sixty-three percent of new HIV diagnoses are attributed to male-to-male sexual contact according to data on HIV infection rates in Georgia. Further, a recent longitudinal study in Atlanta documented a 43.4% HIV prevalence rate and a 6.6% annual HIV incidence rate among BMSM. 8 The HIV epidemiology in the state of Georgia suggests a public health crisis among BMSM that demands for urgent attention.
Given the impact of HIV among BMSM, there is a considerable need to implement the most effective HIV prevention strategies available for this population. More recently, substantial emphasis has been placed on the use of anti-retrovirals (specifically, a combination pill of tenofovir and emtricitabine) as a form of HIV prevention for HIV negative men, also known as pre-exposure prophylaxis (PrEP). 9 This strategy holds tremendous promise, yet our ability to implement a wide-spread, scale-up of PrEP for those at-risk for exposure to HIV in the US has been slow. 10 –14 Namely, PrEP was approved by the US Food and Drug Administration (FDA) in July 2012, and as of March 2013, an estimate of 1774 people in the US have been prescribed the drug, with 48% of those prescriptions being written for women. 15,16 FDA approval is, of course, a critical step in promoting PrEP awareness and uptake, and past work suggests that FDA approval directly shapes PrEP acceptability. 17 However, with 50,000 annual HIV infections, scale-up of PrEP will necessitate greater population uptake than what we currently observe. 18,19
In order to increase uptake of PrEP, it is critical that we focus attention on how PrEP is being embraced by populations at-risk for HIV. Our understanding of community perspectives of PrEP suggests that there are multiple limitations to accessing it, 10,11,20 –24 and that populations in need might not be receiving information about PrEP. 25 We must also acknowledge that those who are at greatest risk for HIV may be least likely to be aware of its availability or have the means to access it. Prior research has identified experiencing syndemics, or numerous interrelated health problems, among MSM as being associated with poorer health outcomes and access to care. 26 –29 From this perspective, it is possible that the a lack of awareness of PrEP co-occurs with other factors known to be related to negative health outcomes such as substance use, risky sex behavior, and HIV testing histories. However, little is understood about syndemics among BMSM 30 or how syndemics might be related to awareness of biomedical prevention.
It is critical that we better understand BMSM's awareness, use, and perspectives of PrEP. There exist limited data on how risk factors for HIV transmission among BMSM, such as sexual risk taking or substance use, are related to awareness or use of PrEP. In order to implement PrEP effectively, we must better gauge community response to this prevention strategy. Without effective, action-oriented efforts, PrEP could run the same course as post-exposure prophylaxis (PEP); PEP is also an effective anti-retroviral based form of prevention, but it has been slow to be promoted and received among BMSM. 31,32 It would be detrimental to HIV prevention if PrEP were to follow the same course of stagnation in uptake.
Study objectives
The focus of the current study was to gain an understanding of the extent to which BMSM were aware of the availability of PrEP and factors related to PrEP awareness. We enrolled BMSM throughout the time period of January 2012 (6 months prior to PrEP approval) through March 2014 (20 months after approval). The specific objectives of the study were to assess: (1) the longitudinal relationship between date (January 2012 through March 2014) and awareness of PrEP availability, (2) the extent to which men were currently taking PrEP or interested in obtaining it, and (3) factors relating to awareness of PrEP with a specific focus on socio-economic status, substance use, HIV testing history, condom use self-efficacy, and sexual risk taking behaviors.
Methods
Sampling, recruitment, and enrollment
Participants were recruited from gay-identified bars, clubs, bathhouses, parks, and street locations; online classifieds; and social media (e.g., Facebook, Black Gay Chat, Jack'd). Participants were screened in-person using electronic handheld devices and over the phone using screening software. For in-person screening, recruiters approached men as they entered targeted venues. Men were eligible to participate if they reported condomless anal sex in the past year with a man, HIV-negative status, were at least 18 years of age or older, and consented to study procedures. Study procedures required participants to attend an in-person appointment at the study research site. The appointment included taking an HIV test and an Audio Computer Assisted Interviewing (ACASI) assessment. All participants tested negative on OraQuick ADVANCE Rapid HIV-1/2 Antibody Test as part of study procedures (participants who tested or disclosed an HIV positive status were referred to other available studies). Participants were compensated $30. Four hundred and seventy-eight participants were recruited and surveyed between January 2012 and March 2014. For the current article, we focused only on MSM who reported being black/African American (N=436). All further analyses involved data from 436 BMSM. All study procedures were approved by <blinded> Institutional Review Board.
Measures
Socio-demographic characteristics
Participants were asked to report their age, years of education, employment status, income, ethnicity, whether they identified as same gender loving/gay, bisexual, or heterosexual, and how “out” they are about their sexual orientation.
Preexposure prophylaxis and postexposure prophylaxis
Participants were given written and verbal descriptions of both PrEP and PEP that described the use and timing of PrEP and PEP (adapted from Eaton et al. 33 ). Participants were asked the following about PrEP and PEP use: “Have you ever heard of PrEP?”, “Have you ever used PrEP?”, “Are you currently taking PrEP?”, “If given the option, would you take PrEP?”, “Have you ever heard of PEP?”, and “Have you ever taken PEP”?
HIV testing history
Participants were asked to report if they had ever been HIV tested prior to their HIV test that day, how many times they had been tested, and the date of their last HIV test (this variable was transformed into months since last HIV test for interpretation purposes).
HIV testing knowledge score
Participants were asked four items regarding their knowledge about HIV testing. 34 Response set included yes/no and the answers were summed. Correct answers were given a point; therefore, higher scores indicated greater HIV testing knowledge. Example items included: “It is possible to test HIV negative but really be HIV positive if someone is recently infected with HIV”, and “I can be certain of my HIV test result even if I am having unprotected sex around the time of the test.”
Condom use self-efficacy
Participants were asked seven questions regarding condom use self-efficacy. 35 Items included a response set of strongly disagree=1 to strongly agree=6. Example items included: “I feel confident in my ability to persuade a partner to accept using a condom”, and “I feel confident that I could stop to put on a condom in the heat of passion.” Responses were averaged and demonstrated acceptable reliability, Cronbach's alpha=0.90.
Substance use
Participants were asked whether they used alcohol, marijuana, crack, party drugs (i.e., cocaine, methamphetamine), sex drugs (i.e., nitrates, sildenafil), and the number of times they used drugs or alcohol during sex in the past 3 months.
Sex behaviors and sex risk taking
Items regarding sex behaviors included number of male sex partners and incidence of condomless receptive or insertive anal sex with a man, separated by perceived HIV status of partner (i.e., HIV negative, HIV positive, or HIV status unknown) in the past 3 months. Participants were asked to report whether they had anal sex during their last sex encounter, and, if yes, did they use a condom during anal sex. Participants were also asked to report on transactional sex; specifically, whether they had exchanged (given or received) money, food, a place to stay or alcohol/drugs for sex.
Data analysis
To begin, we first looked at the longitudinal relationship between date of participant assessment and awareness of PrEP. We used generalized linear modeling with awareness of PrEP, treated as a dichotomous yes or no, as our outcome; therefore, we specified a binary logistic model. For interpretation purposes, Fig. 1 shows seven 4- to 5-month time periods that depict the percentage of participants aware of PrEP by time period.
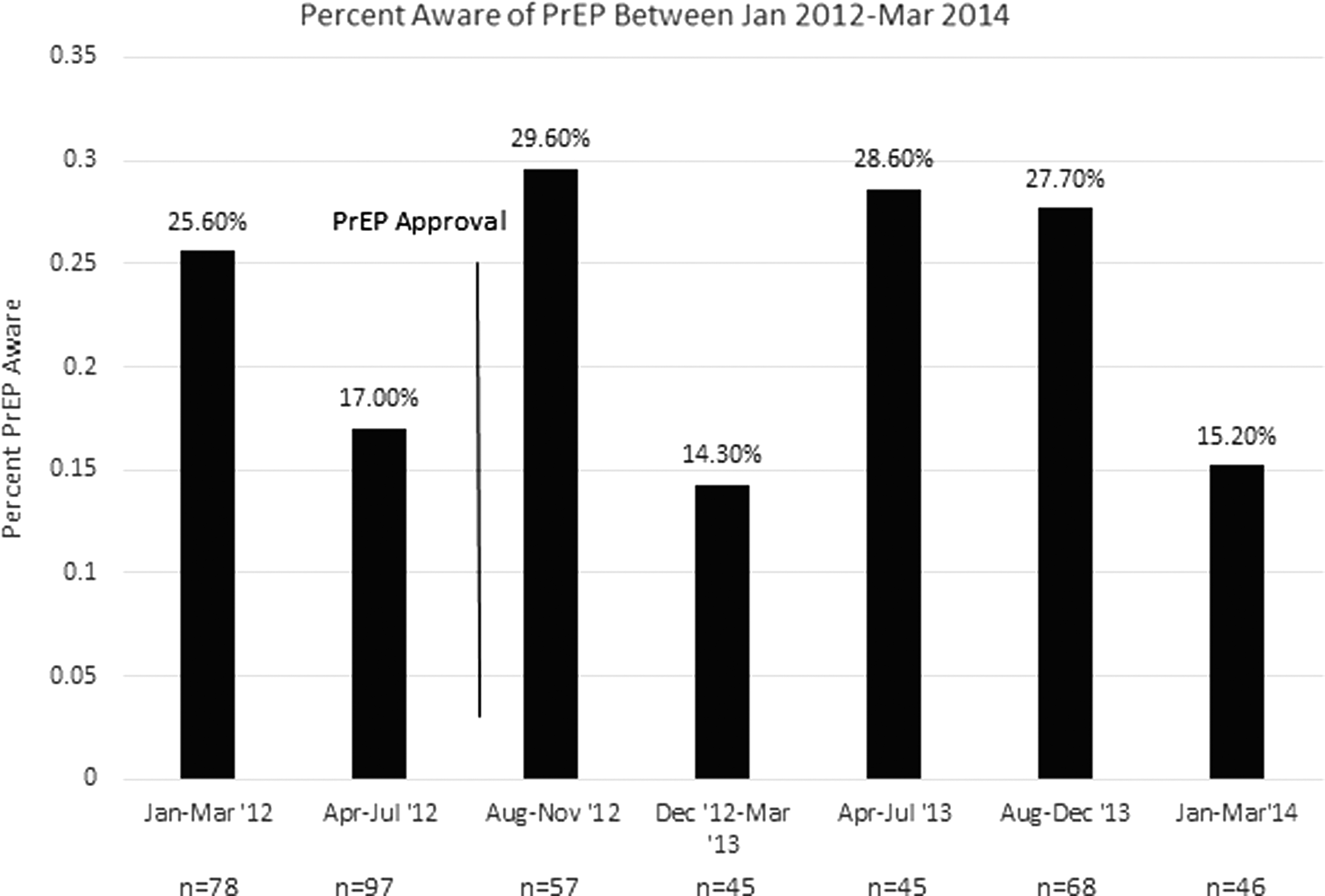
Percentage of BMSM aware of PrEP between January 2012 and March 2014.
Once we established the relationship between time and PrEP awareness, we investigated whether factors such as socio-demographic characteristics, HIV testing history, HIV testing knowledge, condom use self-efficacy, substance use, and sex risk behaviors were associated with being aware or unaware of PrEP. We conducted both bivariate and multivariate analyses of these variables using generalized linear modeling. We provided descriptive data including means and standard deviations, or numbers and percentages for our study variables. Variables were entered into the multivariate model if they were significant (p<0.05) in bivariate analyses. Results are reported as odds ratios (OR). There were less than 5% missing data for any given variable. For all analyses, we used p<0.05 to define statistical significance. PASW Statistics version 18.0 (SPSS Inc., Chicago, IL) was used for all of the analyses.
Results
Awareness of preexposure prophylaxis
In our longitudinal analysis, we found no relationship between date of assessment and being aware of PrEP (OR=0.99 [0.98–1.02], p=0.952). In the 6-month period prior to PrEP approval (inclusive of the month of approval), 20.5% (36/175) of the sample was aware of PrEP, and in the 20 months after PrEP approval, 23.4% (61/261) of the sample was aware of PrEP. In the most recent time interval (January–March 2014), 15.2% of the sample was aware of PrEP. We then ran a multivariate analysis that controlled for demographic data in order to determine whether this data would have an effect on the relationship between time period and PrEP awareness. For this analysis, we included PrEP awareness, time period, age, income, education, and employment status; PrEP awareness remained unassociated with time (OR=0.99 [0.97–1.01], p=0.341). Given that we did not identify differences in PrEP awareness by study enrollment period, all further analyses focus on factors relating to PrEP awareness irrespective of time period.
Socio-demographic characteristics
Twenty-two percent of the entire sample had heard of PrEP (N=97 were PrEP aware, N=339 were not PrEP aware). BMSM who were aware of PrEP were more likely to be older in age, to report more education, to have higher annual incomes, to identify as same gender loving/gay, to be “out” about their sexual orientation, and to have ever heard of PEP than BMSM who had not heard of PrEP (Table 1). We observed no differences in current employment status between groups. With respect to PrEP-specific items, we found that six participants had ever taken PrEP, and three were currently taking PrEP. If given the option, however, most men (81%) would be interested in taking PrEP. On the whole, 25% (N=109) of the sample had heard of PEP and 2% (N=8) had ever used it.
Corresponds to high school diploma.
p<0.05, ** p<0.01, *** p<0.001.
HIV testing history
Men who were aware of PrEP were more likely to have ever been tested for HIV, to have been tested more times for HIV, and to have reported a shorter duration of time since last HIV test (Table 2) compared to BMSM who were unaware of PrEP.
Additional instruction was provided to specify that the question referred to the time period prior to the day of the assessment as that day included an HIV test; buse of Viagra/Cialis/Levitra without a prescription.
p<0.05, ** p<0.01, *** p<0.001.
HIV testing knowledge and condom use self-efficacy
With respect to psychosocial factors, participants aware of PrEP were more likely to score higher on measures of HIV testing knowledge and condom use self-efficacy than participants unaware of PrEP (Table 2).
Substance use
A majority of men reported using alcohol and marijuana in the past 3 months. One-fifth of men reported using crack, one-quarter of men reported using party drugs, and one-sixth of men reported using sex drugs. Results were not significantly different by PrEP awareness (Table 2). Likewise, men reported equal rates of mixing substance use with sex in the past 3 months.
Sex behaviors and sex risk taking
BMSM aware of PrEP reported fewer episodes of condomless, receptive anal sex with partners of unknown HIV status, and were more likely to report condom use during last anal sex than BMSM not aware of PrEP (Table 3). Differences between other sex acts were nonsignificant. BMSM aware and unaware of PrEP reported similar numbers of male sex partners in the past 3 months. BMSM aware of PrEP reported fewer instances of transactional sex than BMSM unaware of PrEP, including both receiving and giving goods for sex in the past 3 months.
p<0.05, ** p<0.01.
Multivariate model of PrEP awareness
In our multivariate model, we included variables found to be significantly related to awareness of PrEP in bivariate analyses (Table 4). For this model, we found that HIV testing knowledge, number of times tested for HIV, and transactional sex were all significant predictors of PrEP awareness when all variables were included; specifically, BMSM with greater HIV knowledge scores, more prior HIV testing experiences, and who reported fewer incidents of transactional sex more likely to be aware of PrEP.
The variables received goods for sex and gave goods for sex were combined to prevent multicollinearity.
p<0.05.
Discussion
Increases in HIV incidence among BMSM underscore the importance of considering new biomedical prevention technologies like PrEP when compiling comprehensive HIV prevention approaches. Our findings and other's, 36 however, suggest that there is considerable groundwork that needs to be achieved in order to implement this approach. We expected that PrEP awareness would increase in the months after approval, but this information is largely limited to a minority of BMSM and, based on the current data, there is no evidence to suggest that awareness is even slowly increasing. The current findings call attention to the need to prioritize and better understand how to strengthen the bridge between medical advances and community uptake. 37,38 Although improvements have been made in biomedical HIV prevention tools, these advances do not help improve the lives of those at-risk for HIV if they are not disseminated and readily accessible. Richardson et al. 39 caution against the over-reliance of biomedical HIV prevention technologies without concurrent changes in the environment where HIV transmission is elevated. Public health agencies must evaluate their current approaches to PrEP, as without considerable changes in the current status quo, PrEP may remain largely underutilized.
Strategies that provide direction on PrEP uptake have been defined and are well-articulated, 38,40 –43 however, public health agencies and primary care providers need to develop stronger ties in order to identify and link to ongoing care individuals who are at elevated risk for HIV. Although historically much of the HIV prevention and treatment efforts in the US have been carried out by community-based HIV/AIDS organizations, many of these agencies are likely unequipped within their currently existing infrastructure to not only raise awareness of PrEP, but seek out, engage, and provide ongoing care for individuals who are on PrEP or candidates for PrEP. This scenario leaves open the need to either enhance and improve services provided by HIV/AIDS medical providers, 44 –46 or to train primary care providers in sexual health assessments and CDC guidelines on PrEP use, and invigorate efforts to promote PrEP. Further, our study focused primarily on challenges relating to awareness of PrEP. Awareness, however, is only one barrier to using PrEP; research among other populations at-risk for HIV has identified multiple factors of important consideration in regards to PrEP use, including adherence 47 and comprehensive health care, 48 which will need to addressed in order to make this strategy work.
In the current study, in our multivariate model, the number of times an individual tested for HIV and HIV testing knowledge were both significantly associated with awareness of PrEP after controlling for multiple relevant factors (other significant bivariate associations). Based on these findings, it appears that having an awareness of PrEP is also linked to greater connection with and understanding of HIV prevention services. These findings underscore the importance of integrating conversations about PrEP within HIV test counseling. These interactions provide opportunities for BMSM to learn about advances in HIV prevention and care, and to discuss whether PrEP would be suitable and appropriate based on their sex behaviors. 49 The relationship between being connected to HIV testing and being aware of PrEP perhaps reflects a broader dichotomy representing men who are either largely informed of prevention services and those who are not aware. From this standpoint, engaging men who are unaware of PrEP will likely require using channels outside of those typically employed by community based HIV/AIDS organizations.
In addition to HIV testing, engaging in transactional sex was associated with being unaware of PrEP in our multivariate model. Given the power imbalance that exists for negotiating safer sex practices during transactional sex, it is likely that these men are at elevated risk for HIV transmission compared with men not engaging in these behaviors. 50 –52 However, there exists a dearth of research on transactional sex among BMSM. Prior work has been largely focused on commercial sex work among MSM in developing countries. We have very little understanding of the extent to which BMSM in the US are at an elevated risk of HIV due to a lack of basic resources (e.g., food, shelter, money) and therefore need to exchange sex for those resources. Focusing on PrEP awareness for BMSM engaging in transactional sex should be prioritized.
Limitations
Data were collected from BMSM in a southern US city and cannot be generalized to the larger population of BMSM. Data are self-report and, therefore, are prone to biases in responses. Participants were asked to report on potentially stigmatizing factors which may be under-reported. In addition, psycho-social measures used in this study have not been validated with this specific population and caution is suggested when interpreting the responses.
It is important to note that more than 80% of our sample reported interest in taking PrEP if given the option; this finding is promising for product uptake. 53 Strategies to increase PrEP awareness through health promotion in community venues, discussions within BMSM's social networks, and provider education may be the first steps toward increasing BMSM's awareness and understanding of PrEP. 54 –56 Beyond community awareness, however, it will be of critical importance to acknowledge the gap between public health advances and community awareness of these advances. We must now prioritize working towards reducing barriers to accessing care for HIV negative men and developing novel ways to reach and engage men who are unaware of prevention services.
Footnotes
Acknowledgments
This project was supported by National Institute of Mental Health Grant R01MH094230 and by National Institute of Nursing Research Grant R01NR013865.
Author Disclosure Statement
The authors declare no conflicts of interest.