
Abstract
The HIV epidemic is experiencing a rapid shift in transmission profile in China. This study aims to examine the changes in magnitude, transmission pattern, and trend of the HIV epidemic in a typical Southwest Chinese prefecture over the period of 1995–2012. HIV surveillance data from the web-based reporting system were analyzed during this period. We investigated the temporal trends in the changing characteristics of HIV transmission, the HIV disease burden in key affected populations, and assessed the impacts on HIV disease progression due to scale-up of antiretroviral treatment. A total of 3556 HIV/AIDS cases were reported in Yuxi prefecture, Yunnan, over the study period. The number of HIV tests conducted has dramatically increased from 1041 in 1995 to 247,859 in 2012, resulting in a substantial increase in HIV diagnoses from 11 cases to 327 cases over the same period. Since 2005, cumulatively 1250 eligible people living with HIV (PLHIV) have received combination antiretroviral therapy which reduced AIDS disease progression from 9.0% (95% CI: 6.7–11.4%) in 1995 to 0.1% (0–0.3%) in 2012 (ptrend =0.0002). The primary mode of HIV transmission has been shifted from injection sharing (71.9% diagnoses in 1995–2004) to unsafe sexual contacts (82.6% diagnoses in 2012). Yuxi prefecture is experiencing a concentrated but shifting HIV epidemic. Scale-up of HIV testing is essential to effective sentinel surveillance and enhancing early diagnosis and treatment in PLHIV.
Introduction
Y
Yuxi prefecture is a predominantly rural area located at the centre of Yunnan and in the proximity of its provincial capital, Kunming City. It has approximately 2.3 million residents and about 62% are living in rural area of Yuxi. 7 HIV sentinel surveillance (HSS) in Yuxi was first established in 1994 and specifically targeted injecting drug users (IDUs) and female sex workers (FSWs). The system was later expanded to include men who have sex with men (MSM) and other at-risk populations, including pregnant women, blood donors, and sero-discordant couples. Under the HSS system, Yuxi Center for Disease Control and Prevention (CDC) conducted annual cross-sectional epidemiological surveys and provided free HIV sero-testing to the at-risk individuals. 2 Confirmed cases identified from the HSS were reported to China CDC through the web-based national HIV/AIDS information system. 8,9 Diagnosed HIV patients were referred to further CD4 count tests and eligible patients (CD4 count ≤350 cells/mm3) were recommended to initiate ART within 3 months of CD4 count tests. The HIV epidemic in Yuxi is a concentrated one typically driven by injecting drug users. It shares many similarities and is generally representative of the HIV epidemic in Yunnan province and Southwest China. 10 Understanding the epidemic trend in Yuxi adds important insights to inform public health policies and HIV programs in this Chinese region.
Yuxi prefectural HSS has collected rich information on the HIV epidemic over the years. This study investigates the changes in magnitude, transmission pattern, and trend of the HIV epidemic in Yuxi prefecture and evaluates the impacts of scale-up of VCT and ART over the period of 1995–2012.
Methods
HIV sentinel surveillance
As of 2012, 93 HSS sites have been established in Yuxi to provide routine HIV surveillance among IDUs (nine community-based sites and one detention center; sample size 400–2000 per site), FSWs (nine sites; sample size 200–500 per site), MSM (nine sites; sample size 20–300 per site), prisoners (eleven sites, including nine detention centers and two jails; sample size 100–500 per site), male sexually transmitted disease (STD) clinic attendees (nine sites; sample size 20–100 per site), pregnant women (nine sites; sample size 3000–5000 per site), blood donors (one site; sample size 6000–20,000), HIV sero-discordant couple (nine sites; sample size 40–300 per site). In addition, 25 HIV VCT sites were established to provide free HIV screening program, and pre-martial screening in 10 maternity and children's health care centers.
Each subject was asked to provide a 2–3 mL blood sample for HIV testing and complete a standardized questionnaire on demographic characteristics and HIV-related risk behaviours. HIV infection was determined by enzyme-linked immunesorbent assay (ELISA) and confirmed by Western Blot analysis. All serological tests were performed in the laboratory of prefectural CDC in Yuxi, Yunnan. All surveillance data were unidentified and downloaded from the web-based HIV/AIDS case reporting system under the supervision of Yuxi CDC.
Monitoring of PLHIV on treatment
Medical records of PLHIV on ART were obtained from the web-based HIV/AIDS case reporting system and reviewed retrospectively. Data collected included demographic characteristics (i.e., age, sex, marital status, residency, and educational level), information of HIV diagnosis (i.e., date of HIV diagnosis, mode of transmission, and date of clinical confirmation of AIDS), and treatment information (i.e., date of ART initiation). Modes of HIV infection was categorized as blood transfusion/donation, sexual contacts (homosexual or heterosexual), injecting drug use, mother-to-child transmission, and unspecified transmission route. The current threshold for ART was CD4 count ≤350 cells/mm3. 11 The dates of HIV diagnosis, CD4 count test, and ART initiation were also recorded. The annual AIDS progression rate was calculated by dividing the number of patients who have progressed to from chronic HIV infection to AIDS stage each year by the total number of HIV-diagnosed individuals.
Statistical analysis
All statistical analyses were conducted in the Statistical Package for the Social Sciences (SPSS) software for Windows (version 21.0; SPSS Inc., Chicago, IL). Descriptive statistics and frequency distribution of the sample were calculated. Chi-square statistics was used for the analysis of categorical variables, while time trend for continuous variables were evaluated by Kruskal-Wallis test. Significance level of 0.05 was used for all statistical tests. The estimated progression rate was calculated as the ratio of number of cases converted from chronic HIV stage to AIDS and the cumulative number of reported HIV cases. The 95% confidence intervals (CI) of AIDS progression rate were calculated based on the ‘exact’ binomial distribution. 12 This study was approved by the Institutional Review Board of the Tsinghua University (TH00131217YX).
Results
Sentinel surveillance in key populations
A total of 1,150,604 subjects from 10 different at-risk populations were tested for HIV infection through routine surveillance during study period. About 41.0% were inpatients, 21.9% pregnant women, 16.3% clients tested for martial purposes, 10.1% voluntary blood donors, 1.9% FSW, 1.3% IDUs, 1.3% prisoners, 0.3% male STD clinic attendees, 0.2% HIV discordant couples, 0.1% MSM, and 5.6% was unclassified. A sharp increase was reported in the number of testing samples (from 9662 in 2003 to 30,274 in 2004, Fig. 1) as a result of the launch of the national campaign for VCT among high-risk populations in China in 2004. By the end of 2012, the case reporting system recorded a cumulative total of 3556 HIV/AIDS cases (551 cases of AIDS), and 512 reported HIV-related deaths.

Annual reported HIV positives and AIDS cases in Yuxi prefecture, 1995–2012.
HIV prevalence among IDU had an early onset of 3.1% (10/319) in 1995 and peaked at 20.6% (44/214) in 2000. It then fluctuated between 10–15% during 2002–2008 and gradually declined to 3.3% (66/1971) in 2012 (Fig. 2). Similarly, HIV prevalence among FSW initiated at close to zero level (0/329) at 1995 but varied between 0.7% and 1.4% over the period 1999–2009. It then experienced a recent decline to 0.7% (13/1836) in 2011 and 0.2% (3/1617) in 2012. The first HIV case in MSM was reported in 2006, although the first HSS site for MSM in Yuxi was not established until 2008. Available surveillance indicated a fluctuating prevalence in MSM, varying from 8.6% (6/70) in 2009 to 12.4% (13/105) in 2010 and then to 4.2% (33/779) in 2012. The temporal variation was not significant (ptrend =0.750). HIV prevalence among male STD clinic attendees was low in early 1990s (0–2.5%), it reached the peak of 9.5% (8/84) in 2002 and fell at the level of 5–6% in late 2000s. It remained higher than that of FSW in most years. The prefectural average HIV prevalence among pregnant women remained low and stable at approximately 0.1% from year 2000 onwards (ptrend =0.823).
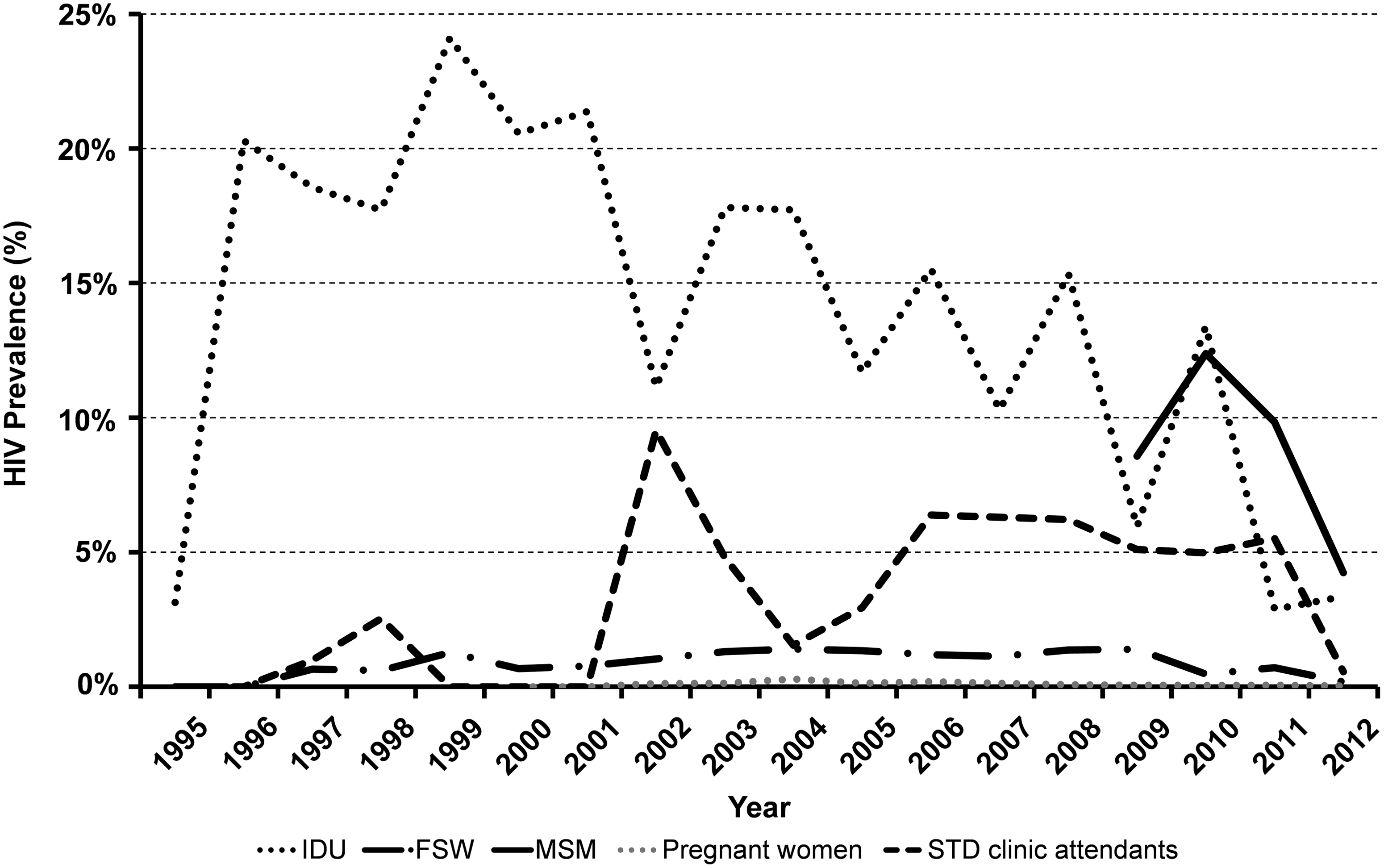
HIV prevalence among IDU, FSW, MSM, pregnant women, and STD clinic attendants from sentinel surveillance in Yuxi prefecture, 1995–2012.
Characteristics and trends of reported HIV/AIDS cases
The number of HIV tests increased dramatically from 9662 in 2003 to 30,274 in 2004, then experienced an eightfold increase in 2012 (247,859 tests). In comparison, the number of HIV/AIDS diagnoses increased from 11 cases in 1995 to 425 cases in 2009, but started to stabilize in recent years (Fig. 1). Of the 3556 HIV/AIDS diagnosed cases, 3212 (90.3%) were local residents, 233 (6.6%) from other prefectures in Yunnan province, and the remaining were migrants from other provinces. The severity of epidemic varied widely across the prefecture. Of 3212 local cases, 28.9% were registered in Hongta District, followed by Chengjiang County (14.6%) and Tonghai County (13.2%). Eshan Yi Autonomous County had the lowest number of reported cases (2.9%) in the prefecture throughout the period.
Age distribution of newly diagnosed HIV cases has changed substantially over time (Fig. 3). Notably, the proportion of 21–30 and >50 age bands increased from 11.5% and 3.9% in 2005 to 25.7% and 17.1% in 2012, respectively, while the proportion of 31–40 decreased from 66.9% to 30.7% over the same period. The proportion of HIV infection through syringe/needle-sharing decreased substantially from 60.6% in 2005 to 15.5% in 2012, while transmission attributed to heterosexual contact increased from 36.4% to 79.1% in the same period. Self-reported homosexual transmission accounts for 3.5% in 2012. In 2012, the male–female ratio of newly diagnosed HIV cases was 1.7:1, more than half (52.7%) were married and about three-quarters were local residents (72.7%). The break-down of reported HIV cases by gender, educational level, marital status, and residency did not change over time.
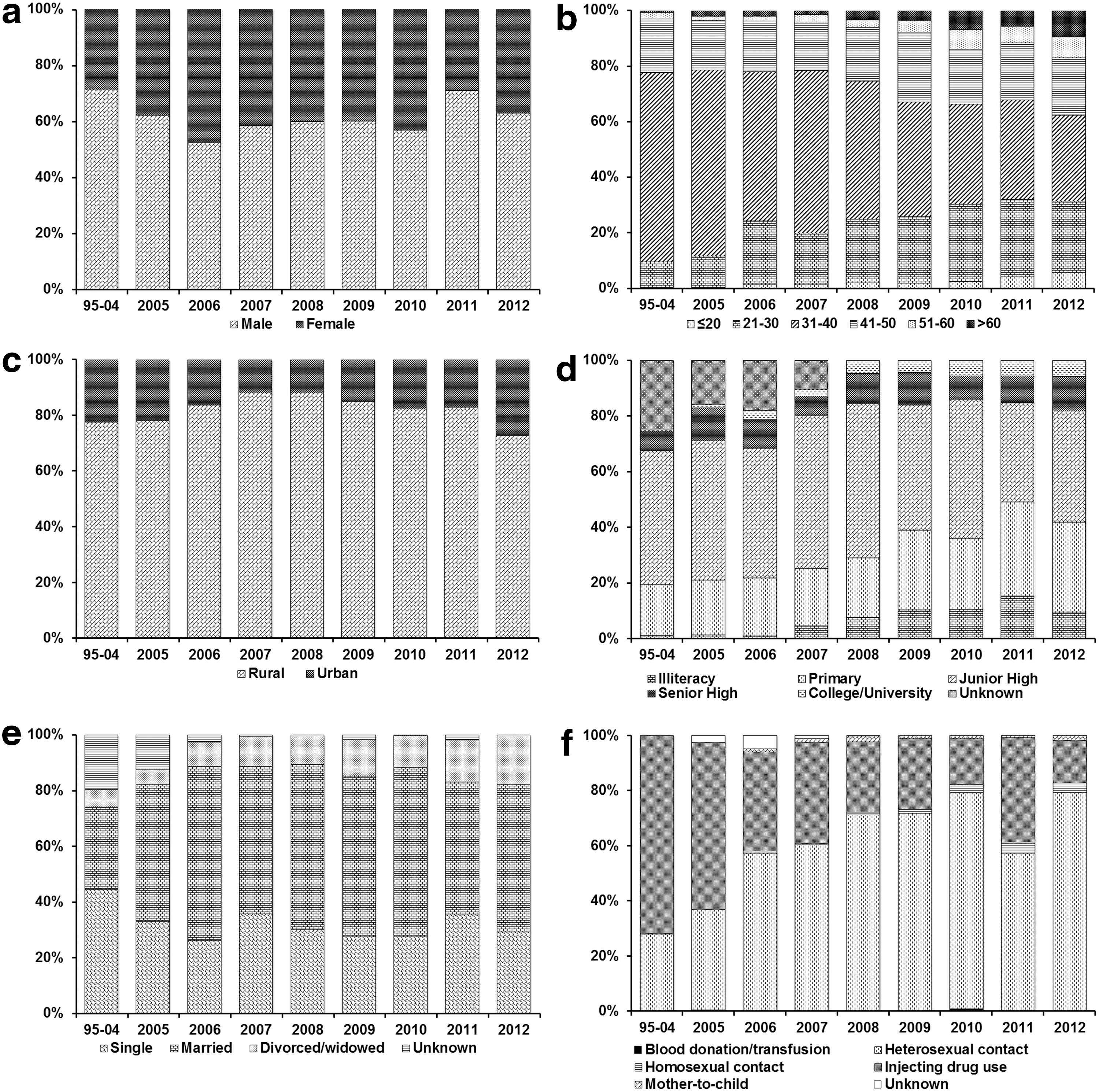
Reported HIV cases in Yuxi prefecture from 1995–2012 stratified by
Characteristics of HIV patients at ART initiation
The progression rate from chronic HIV infection to AIDS among PLHIV decreased significantly from 9.0% (95% CI: 6.7–11.4%) in 2005 to 0.1% (0–0.3%) in 2012 (ptrend =0.0002, Fig. 4). This is aligned with the sharp increase in the number of PLHIV receiving ART from 27 in 2005 to 1250 in 2012. Overall, the majority of ART patients acquired HIV through heterosexual contact (59.5%), about 30.1% through needle-sharing, and only 1.4% through male-to-male sexual contacts (Fig. 5). About 71.0% of the patients had been diagnosed with HIV for 5 years or less. Among eligible patients (CD4 counts ≤350 cells/mm3), the median time from diagnosis to treatment initiation was 1.6 years.

Cumulative number of HIV/AIDS patients receiving ART and progression rate from chronic HIV infection to AIDS, 1996–2012.

HIV/AIDS patients who receiving antiretroviral treatment (ART) from 2005–2012 stratified by
Discussion
This study investigated the trend of the HIV epidemic in Yuxi prefecture over an 18-year period. The epidemic remained concentrated among key affected populations such as IDU, MSM, FSW, and STD clinic attendants, and its prevalence remain low and stable over the last two decades. Consistent with previous findings, 4,13 our study strongly indicates a rapid transition phase of the HIV epidemic in Yuxi, characterized by the shift of transmission mode from unsafe injection sharing to heterosexual contacts, and enlarging PLHIV populations in both young and elderly groups in recent years. The dramatic scale-up of HIV testing and ART programmes had significantly reduced progression to AIDS among PLHIV.
The implementation of the national “Four Frees, One Care” policy in 2004 is a key milestone of HIV prevention in China. It has directly contributed to the expansion of the VCT program, which is reflected by the large number of HIV diagnoses reported in our study. This policy also enables timely initiation of life-saving ART, which prevents progression from chronic HIV infection to AIDS and also subsequent deaths. The preventive effects of ART have also been well documented. 14,15 Patients on ART have not only a reduced risk of HIV transmission to their sero-discordant partners, 16,17 but also a reduced risk of acquiring other STDs. 18 A recent study has indicated that home-based interventions can significantly improve the adherence of ART patients. Sustaining a matching scale-up of ART and adherence interventions is necessary in reducing disease burden of HIV infection in the affected populations. 19 Although VCT has been an effective strategy in HIV prevention, the marginal cost required to identify one extra undiagnosed PLHIV could substantially increase when the program coverage reaches a saturation level. 20 Targeted testing among high-risk groups should be prioritized. However, rooted in social and cultural values, 21,22 stigma and discrimination are commonly experienced by the high-risk populations (e.g., MSM, FSW, and IDU) and PLHIV in China. 21 –26 Scale-up of multilevel interventions is necessary to reduce stigma and improve access to HIV testing, care and treatment. 21
The HIV epidemic in Yuxi has been IDU-driven, and its recent epidemic shift to homosexual transmission indicates an effective channel of HIV transmission across the most at-risk populations. Previous studies have reported overlapping risk behaviors in these populations in Southwest China, particularly in Yunnan province, 27,28 such as male IDUs soliciting commercial sex from FSWs, 29 FSWs selling sex for drugs, 30 and MSM engaged in commercial sex trade and injecting drug use. 31,32 Addressing the overlapping behaviors in these populations remains a major challenge for HIV prevention and control in the region. Integration of existing HIV prevention programs is important in targeting multiple risk behavior that associated with a particular population.
The proportion of HIV diagnoses in the elderly population (>50 years old) has been significantly increased over time, and this is consistent with findings in other parts of China; 33 however, the cause of rise remains unclear. Elderly had reportedly poorer knowledge and awareness of HIV/AIDS, 34 and Chinese doctors avoid discussing sexual life and HIV risk with their elderly patients. 35 Recent studies have reported that elderly may be often willing to engage in high risk sexual activities and less concerned of being infected with HIV because of their self-perceived limited years of living. 36 Among infected elderly, early symptoms such as fever, dementia, and weight loss may be masked and overlapped with other age-associated diseases, 37,38 resulting in delay of HIV diagnosis. 39,40 In contrast, young people (≤30 years old), being substantially more risk-taking in unprotected sex, multiple sexual partnerships, and noncommercial casual sex, 41 are also found to be increasing in the number of diagnoses. Being more technology savvy and soliciting sex through Internet or the smartphone applications 36,42 enable the younger generation, especially among MSM, to expand their sexual networks and hence increases their risk of acquiring HIV. 43,44
This study has several limitations. First, the trends of HIV diagnoses may not be representative of the undiagnosed individuals. HIV undiagnosed rate are high in China, particularly among MSM (∼87%). 45,46 MSM are reluctant to access HIV services due to stigma and discrimination. 22,36 At diagnosis, MSM are often not willing to disclose their sexual orientation, leading to substantial underestimation of the proportion of HIV cases attributed homosexual transmission. Second, sentinel surveillance of at-risk populations in early days was subject to potential sampling bias. Establishing sentinel sites at hotspots often leads to overestimates of the actual disease burden. The hidden nature of specific at-risk group may result in small effective sample size and high uncertainties in HIV prevalence estimates. 9 Third, the estimated AIDS progression rate may be subjected to the lead-time bias after the introduction of ART. Besides, improved diagnosis of HIV due to scale-up of testing services alone may lead to an extended duration for AIDS progression. Furthermore, previous studies have shown that several factors such as age, 47,48 opportunistic diseases, 49 and the mode of transmission 50,51 are the co-factors that affecting the disease progression but are not examined in this study.
Our study has important implications for HIV prevention in China. Given that the HIV epidemic is disproportionally affected in youth and elderly, it is important to promote regular sexual health check in these two populations, particularly those who are sexually active. Health education programs should specifically target elderly to improve their HIV knowledge and awareness, the associated risk factors, and reduce misconceptions about HIV. Educational interventions may be integrated into primary care to provide relevant information to the elderly. Multi-strategy interventions should be designed to target overlapping risk behaviors in the target groups. Components of safer sex intervention (e.g., condom and lubricant distribution) could be added and enhanced while implementing drug-related programs such as needle and syringe program and methadone maintenance treatment (MMT) for drug users. 52 Further scale-up of VCT plays an essential role in HIV surveillance and prevention and should be prioritized to the most at-risk populations.
Footnotes
Acknowledgment
We thank all the Endeavour Research Fellowship (Award ID: 2744_2012) for its support in EPFC's study in China.
Author Disclosure Statement
No conflicting financial interests exist.