
Abstract
Condomless commercial sex work is a common mode of HIV transmission in China. This study systematically reviews the impacts of behavioral interventions on condom use and HIV testing uptake among female sex workers (FSW) in China. Chinese and English language peer-reviewed articles published between January 2000 and December 2013 were searched in five electronic databases. Odds ratios (OR) were calculated by comparing the levels of improvements in condom use and HIV testing uptake by various intervention strategies. Study quality was assessed for included studies. This review followed the PRISMA guidelines and was registered in PROSPERO. One hundred and twenty-eight studies met inclusion criteria. Meta-analyses indicated that FSW in the post-intervention period were 2.3–5.0 times more likely to use condoms with male clients in their last sexual act and 2.3–3.4 times more likely to use condoms consistently in the last month than in the pre-intervention period. In particular, multiple session intervention were more effective in improving condom use among FSW with male clients (OR=5.6, [4.0–7.8]) than a single session intervention (OR=3.3, [2.8–3.8]). Behavioral interventions also improved past-12-month HIV testing uptake 4.6-fold (95% CI, 2.9–7.4). Comprehensive intervention programs were more effective (OR=8.1, [4.0–16.7]) in improving HIV testing uptake compared with health education only programs (OR=2.7, [1.6–4.5]). Longer intervention duration (>12 months) did not increase effectiveness in improving condom use or HIV testing rate among Chinese FSWs. Behavioral interventions are effective in improving condom use and HIV testing uptake among Chinese FSW. This review highlights both the potentials and limitations of condom promotion interventions targeting female sex workers.
Introduction
I
Studies among Chinese FSW generally report low education level and HIV knowledge. 2 –4 Behavioral interventions, such as promotion of condom use and voluntary HIV counselling and testing (VCT), form the core of HIV prevention activities among FSW in China. HIV interventions for Chinese FSW mostly include two types: (1) health education programs, which mainly involve distribution of HIV information leaflets and condoms, health education to improve HIV awareness and knowledge of symptoms, and promotion of timely healthcare-seeking and treatment; 5 and (2) comprehensive intervention programs, which include health education plus additional sexual health care services, testing for HIV infection. and counselling service. 5 Both types of interventions are primarily delivered by peer-educators through the sentinel surveillance network of the Chinese Centers for Disease Control and Prevention (China CDC). 6 Other international donors, such as the Global Fund, the Bill and Melinda Gates Foundation, and the Joint United Nations Programme on HIV/AIDS (UNAIDS), also contribute substantially at the regional level. 7,8
Encouragingly, the Chinese HIV sentinel surveillance system reported a decline in HIV prevalence among FSW from 0.46% in 2000 to 0.36% in 2010. 9 Widespread implementation of behavior change interventions may have contributed to this decline. Several recent reviews specifically examined the effectiveness of HIV/AIDS-related behavioral interventions among other high-risk populations in China, including men who have sex with men (MSM) 10,11 and domestic migrants (i.e., ‘floating population’ in the Chinese context). 12 These studies investigated changes in the number of sexual partners, condom use, HIV knowledge and HIV testing uptake rate and identified important nuances across interventions, such as differential effects of interventions on condom use with male versus female partners 11 and variation by intervention approach and study design. 10
Although numerous studies have reported reduced risk behaviors among Chinese FSW due to behavioral interventions, a systematic review and meta-analysis of the effects of these interventions has not yet been conducted. Thus variation in the design and duration of the intervention strategies, and how these variations may affect the intervention outcomes remains largely unchecked. A comprehensive data synthesis is therefore valuable in examining the differences in the effectiveness of these intervention strategies. This meta-analysis is specifically designed to assess and compare the impacts of various intervention strategies on condom use and HIV testing uptake among Chinese FSWs.
Methods
Protocol and registration
This review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Statement issued in 2009 (Checklist S1). 13 The protocol for this review was prospectively registered (CRD42014013466) with the International Prospective Register of Systematic Reviews (PROSPERO).
Search strategy
We searched PubMed, Embase, VIP Chinese Journal Database (VIP), Wanfang Data, and China National Knowledge Infrastructure (CNKI) for relevant intervention studies among FSW in China from January 2000 to December 2013. The search was conducted using free-text terms and Medical Subject Headings (MeSH) terms: (‘human immunodeficiency virus’ OR ‘HIV’ OR ‘Acquired immune deficiency syndrome’ OR ‘AIDS’) AND (‘prevention’ OR ‘intervention’ OR ‘control’) AND (‘female sex workers’ OR ‘commercial sex workers’ OR ‘women who sell sex’ OR ‘FSW’ or ‘CSW’) AND (‘China’ OR ‘Chinese’). Hand searching from the reference lists of the retrieved articles in the above databases was also included. Our search strategy was limited to English and Chinese language publications. Two reviewers (EPFC, KT) independently screened all retrieved abstracts from the five aforementioned databases against the selection criteria. Discrepancies were resolved by a third reviewer (LZ).
Selection criteria
Type of studies
We preferentially looked for studies that evaluated the effectiveness of behavioral interventions to reduce risk behaviors. We included randomized controlled trials (RCTs) that compared the effects between intervention and control groups, or nonrandomized before-and-after studies to compare the effect between pre- and post-interventions. Studies conducted in Hong Kong, Macau, and Taiwan were excluded.
Type of participants
We only included studies conducted in China with females who self-reported as sex workers and who were specifically targeted by the intervention. There were no restrictions on demographic characteristics.
Type of interventions
Behavioral or social interventions that were designed to increase condom use and/or HIV test uptake were included. Interventions focused exclusively on pharmaceutical (e.g., post-exposure prophylaxis) or cognitive (e.g., HIV knowledge) outcomes were excluded.
Type of outcome measures
We included studies that reported changes in condom use in the last sex act, consistent condom use in the past one month with various partnerships (i.e., unspecified, regular partner, and commercial clients); and any change in HIV testing uptake (i.e., “ever” and “any” testing within the past 12 months).
Quality assessment
The quality assessment of eligible studies was measured according to the checklist tools for assessing quality in observational studies. 14 Six domains were used to assess the risk of bias: (1) methods for selecting study participants; (2) methods for measuring exposure and outcome variables; (3) design-specific sources of bias; (4) methods to control confounding; (5) statistical methods; and (6) other biases (including conflict of interest and disclosure of funding sources). The quality of each item was categorized as either ‘Low risk (+)’, ‘High risk (−)’ or ‘Unclear (?)’ in accordance with the guidelines recommended by the Cochrane Collaboration. 15
Data extraction and management
Data were extracted and entered into a predesigned electronic data collection form in a Microsoft Access database (Version 2010, Microsoft Corp., Redmond, WA, USA). Each study was given by a unique ID and the data collection form included information on: (1) study design: location, sample size, type of intervention, duration of intervention, and number of follow-up time points; and (2) the reported outcome measures. Each intervention was categorized as a “comprehensive” intervention program or a “health education-only” program (as defined in the Introduction) for each outcome. Duration of the intervention was categorised as less than or equal to 12-month, or more than 12-month intervention period. We also recorded the number of follow-up intervention sessions.
Statistical analysis
Meta-analyses were performed to calculate odds ratios (OR) and 95% confidence intervals (CI) in order to evaluate the impact of each intervention by using the Comprehensive Meta-Analysis software (Version 2.2, Biostat, Englewood, NJ, ISA). Each outcome was stratified by the type of intervention strategy (i.e., comprehensive intervention program, or health education program), duration of intervention period (i.e., ≤12, or >12 months), and number of follow-ups (i.e., one, or more than one intervention session).
Heterogeneity across studies was detected by the chi-square based Cochran Q-test and I 2 statistic. 16 –18 Random-effects model was used if high and significant heterogeneity (I2>75) was detected across studies; 18 otherwise, fixed-effects model was used. Sample sizes of the study were taken into account in both models.
Results
Characteristics of included studies
We identified 569 records based on our keyword searches; of those 415 were unique records (Fig. 1). After screening the full-text, a total of 128 studies were included in the meta-analysis (Supplementary Table S1; supplementary data are available online at
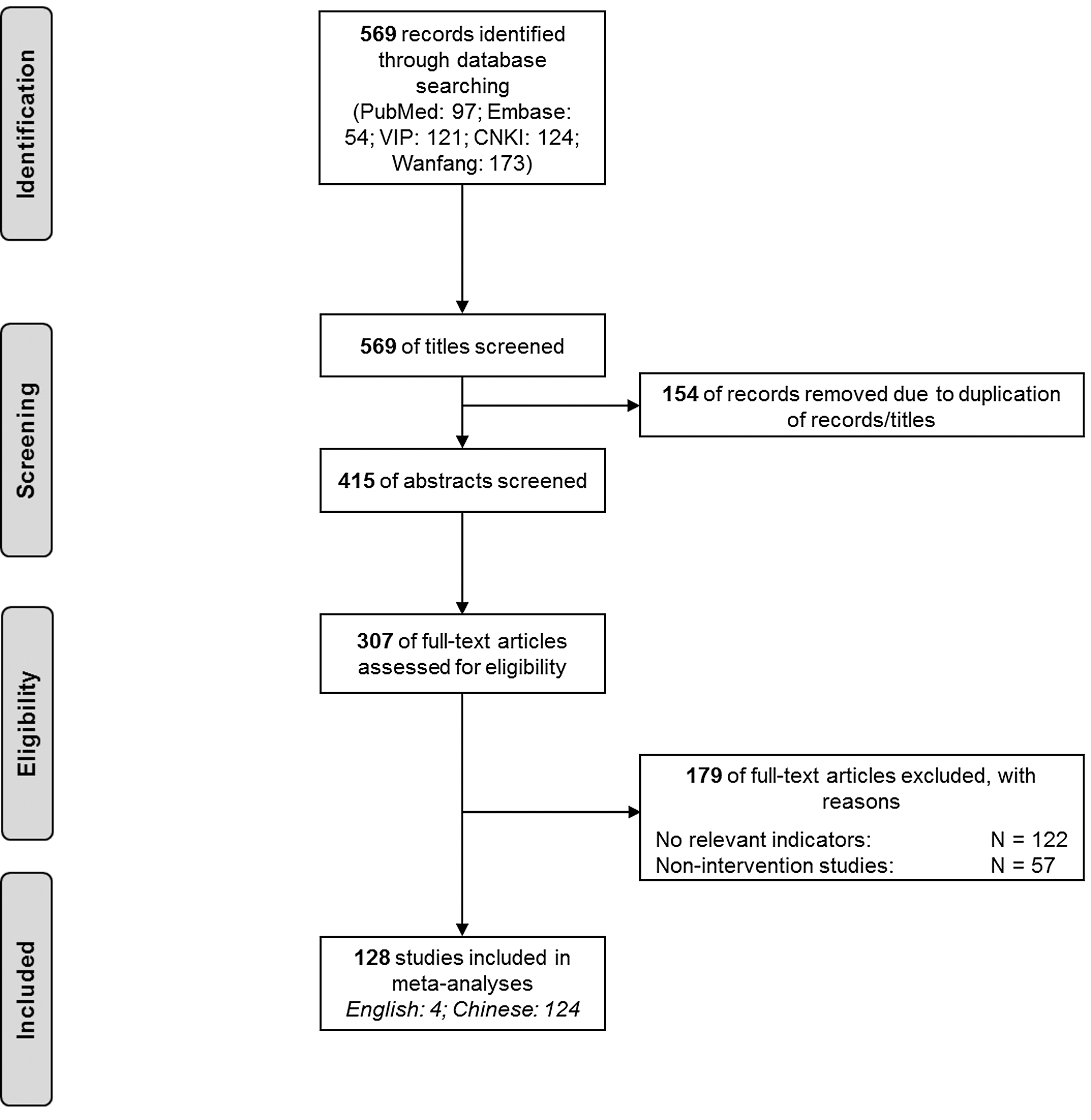
PRISMA flow chart of study selection.
Condom use in last sex act
Overall, behavioral interventions significantly increased condom use at last sex act among FSW regardless of partnership type: any male partners (OR=5.0, 95% CI: 3.4–7.2), regular partners (OR=2.3, [1.8–2.9]), or commercial clients (OR=3.5, [3.1–4.1]) (Table 1). In particular, interventions with multiple session interventions were more effective than those with a single session intervention for increasing condom use with any partner (OR=20.3, [5.2–78.8] versus OR=4.0, [2.8–5.7]) and commercial clients (OR=5.6, [4.0–7.8] versus OR=3.3, [2.8–3.8]). However, intervention approach and duration of intervention did not lead to significant differences in the extent of improvement of condom use.
p<0.05; ** p<0.01; *** p<0.001.
Consistent condom use in the past 1 month
Post-intervention, there were substantial increases in the odds of women reporting consistent condom use in the past 1 month with any partners (OR=3.1, [2.0–4.7]), regular partners (OR=2.3, [1.7–3.1]), and commercial clients (OR=3.4, [2.8–4.0]) (Table 2). However, using a comprehensive approach, longer duration and multiple sessions did not appear to add to the effectiveness of the interventions.
p<0.05; ** p<0.01; *** p<0.001.
HIV testing
The median proportion of FSW who were ever-tested for HIV increased from 10.4% (7.4–22.8%) prior to intervention to 44.2% (25.9–63.1%) after intervention, whereas past-12-month testing rate increased from 17.0% (14.1–40.9%) to 58.0% (45.0–75.4%). These correspond to 5.0 (2.7–9.6) and 4.6 (2.9–7.4) times higher odds of HIV testing, respectively (Table 3). Comprehensive intervention programs demonstrated a greater effect on improving past-12-month HIV testing rate than health education programs alone (OR=8.1, [4.0–16.7], versus OR=2.7, [1.6–4.5]; p=0.015).
p<0.05; ** p<0.01; *** p<0.001.
Risk of bias within and across studies
Among the 128 included studies, only one study had low risk of bias for all six methodological quality items. The remaining 127 studies had high or unclear risk for at least one of the bias items. No studies had high risk for all six items (Supplementary Fig. S1). Overall, most studies had low risk of bias in methods for selecting study participants (63%), measuring exposure and outcome variables (77%), and statistical measures (91%) (Supplementary Fig. S2).
Discussion
This review summarized 128 behavioral intervention studies conducted among FSW in China, demonstrating the effectiveness of these interventions for improving condom use and HIV testing uptake. Our analysis fills an important gap in the literature on both the Chinese and the international HIV epidemics, as past reviews of FSW interventions conducted in resource-limited settings have included only one China-based FSW intervention. 19 Notably, we find that increased condom use is more likely in programs with multiple session interventions. Additionally, comprehensive intervention programs are more effective in increasing HIV testing updates than health education alone. However, interventions with extended duration of implementation (over 12 months) do not further improve the already significantly elevated condom usage and HIV testing uptake.
Our reported high effectiveness of behavioral interventions in improving condom use and HIV testing uptake among FSW in China is consistent with the findings from the “100% condom use program” implemented in most Asian countries. 20 In China, more FSW used condoms for contraception purposes, rather than preventing HIV and other sexually transmitted infections (STIs). 21 Only a small proportion of sex workers (∼7%) have access to condoms at their work places, 22 while the majority of women (>75%) have to purchase condoms on their own. 23 Although HIV prevalence among Chinese FSW remains low and stable (0.36%), 9 the prevalence of other STIs is high. 24
Incorrect and low condom use in certain sexual practices is common; only 22.7% of FSW used condoms during oral sex, compared to 57.9% in penile-anal, and 70.1% during penile-vaginal sexual intercourse. 23 About half (48–51%) of Chinese FSW report experiencing condom breakage or slippage during intercourse. 23,25 Incorrect uses of condoms, such as using already damaged or expired condoms, or applying condoms after intercourse begins have also been reported. 26 Willingness for condom use in male clients is also low. 27 Lack of negotiation power and the fear of losing clients are major barriers for consistent condom use among Chinese FSWs. 28
Among Chinese FSW, comprehensive intervention programs have demonstrated greater advantages than health education programs alone, as they not only improve condom use but also link FSW to HIV testing services. HIV testing and counselling service is an integrated component in comprehensive intervention programs but not in health education programs. Outreach efforts to socially stigmatised key affected populations can successfully promote HIV screening play an essential role in HIV prevention and treatment. 29 Regular HIV screening is an essential first step for diagnosis, linkage to care, and subsequent early initiation of antiretroviral treatment. 30
Repetitive enhancement through behavioral interventions is essential for reinforcing positive behavioral patterns. In contrast to single session interventions, which are shown to have limited effectiveness in promoting condom use and HIV testing uptake, 31 multiple session interventions allow the space and time for establishing the necessary trust between FSW and health promotion educators. In this analysis, we found a large difference in effect size between interventions that used multiple sessions as compared to single session interventions (20.3 vs. 4.0). Multiple sessions could reinforce messages for safer sex at each follow-up visit, and also allow more time for the individuals to adopt a new behavior; and therefore, multiple sessions could be more effective in increasing condom use than single session interventions.
Our findings confirmed previous work showing that extended intervention duration without repeated follow up among the same target cohorts does not significantly impact individuals' behaviors changes. 32 It should also be noted that the wide confidence interval for multiple session intervention may be due to small sample size, and two out of three data points reported huge increase of condom use were collected from one small study; therefore, data must be interpreted cautiously.
Several study limitations should be noted. First, about one-third (43/128) of the studies were conducted in Southwest China. This area is known to have a history of higher HIV disease burden and is thus likely a target region of behavioral interventions. 9,33 Second, HIV disease burden and risk behaviors among Chinese FSW may vary in different venue settings. Street-based FSW are likely to have greater risk behaviors than entertainment-based FSW. 33 Observed impacts of interventions may differ across different subgroups of FSW but we are unable to extract relevant information from the original studies in order to assess these relationships. Third, the majority (98.4%) of studies used single-group pre-and-post study design, only two studies utilised a rigorous evaluation methodology (i.e., quasi-experimental design). 34,35 Potential confounders may be associated with differences in study design. Fourth, no biomarkers of disease were measured; outcome data thus relied on self-report, which may result in large uncertainties in outcome measures due to recall bias and social desirability.
This study has several key implications for intervention programs in China. Overall, the condom use rate and HIV testing uptake were improved by the behavioral interventions, but sustaining the level of coverage may require ongoing government investment. High risk subgroups of FSW, characterized by inconsistent condom use, poor working environment, and low literacy rates, remain a high priority for behavioral interventions. While these women may be harder to reach for multi-session interventions, community-based screening efforts—such as those done for syphilis—may provide a model for effectively reaching large numbers of Chinese FSW. 36
Comprehensive intervention programs should not only focus on FSW but also extend to male clients of FSW to prevent “bridging” transmission of HIV to the general population. 37 In order to maximize the effectiveness of the intervention, interventions should focus on the content and delivery through repeat sessions and consistent follow-ups. Effective behavioral intervention strategies should be expanded beyond the current concentration in major urban cities 38,39 to less developed rural regions.
Footnotes
Acknowledgments
EPFC is supported by the Early Career Fellowships from the Australian National Health and Medical Research Council (NHMRC) (No.: 1091226).
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.