
Abstract
Few studies in China have focused on advanced human immunodeficiency virus (HIV) disease (AHD) and late entry to HIV care, which are associated with increased morbidity and mortality. A population-based retrospective study was conducted using 980 national HIV surveillance reports from 1994 to February 2012 in Wuhan, China. AHD was defined as presence of a first-reported CD4 count <200 cells/μL or an acquired immune deficiency syndrome (AIDS)-defining event within 1 month of HIV diagnosis. Late entry to HIV care was defined as patients with a first-reported CD4 cell count >6 months after diagnosis. Non-conditional logistic regression analysis was used to identify factors associated with AHD, late entry to HIV care, and AIDS within 1 year of HIV diagnosis. The proportions of AHD, AIDS within 1 year of HIV diagnosis, and late entry to HIV care were 29.49%, 39.39%, and 20.84%, respectively. Most of the deaths (74.27%, 127/171) occurred within 1 year of diagnosis. Short-term mortality, proportion of AHD, and late entry to HIV care showed a similar downward trend from pre-2003 to 2011 (p<0.001). Age, transmission category, sample source, and occupation were associated with AHD, late entry to HIV care, and AIDS within 1 year of HIV diagnosis in the multivariate logistic regression analysis. These findings indicate that AHD and late entry to HIV care were associated with an increased incidence of AIDS or death, particularly within 1 year of diagnosis. More effort should be made to assure early diagnosis and timely entry to care.
Introduction
S
A late diagnosis of HIV infection typically occurs when the patients develop HIV-related symptoms, or their immune systems are permanently damaged with a low CD4 cell count. Furthermore, many will inadvertently infect their partners without the knowledge of positive HIV serostatus. 7,8 Due to the advanced stage of disease, late diagnosis of HIV increases the risk of short-term mortality (death within 1 year of diagnosis) and mortality in general. 9,10 On the contrary, early diagnosis of HIV infection and subsequent timely initiation of ART can ensure maximum benefit by strengthening the impact of therapy and thus reducing AIDS incidence.
This may also reduce HIV transmission risk behaviors and HIV transmission. 11,12 Early diagnosis of HIV infection and timely treatment might increase lifetime costs, but ultimately prove to be cost-effective. 11,13 In addition, early diagnosis and timely treatment increase life expectancy 14 –16 and improve quality of life. 15 However, many factors could be associated with late diagnosis of HIV infection, and understanding the related factors is critical to the development of effective programs and treatment strategies. 17
According to the China AIDS response progress report in 2012, the estimated number of PLWHIV in China stood at 780,000 people by the end of 2011. Although China has made progress in HIV prevention and control, the epidemic remains serious and complex. 18
However, the issue of late diagnosis of HIV infection and entry to HIV care in China remains unclear. One cross-sectional study conducted from 2009 to 2010 indicated that 72.02% of the HIV infectors from 10 provinces in China were diagnosed late (CD4 count ≤200 cells/μL). 19 Given the current situation, we used HIV surveillance data in Wuhan, China, to explore the related factors and obtain a better understanding of late diagnosis of HIV infection and entry to HIV care. We hope to provide scientific evidence for HIV prevention and control, thereby highlighting the importance of this issue in China.
Methods
Data source
Data from 1994 to February 2012 were derived from the national HIV surveillance system. All PLWHA in China are reported to the Center for Disease Control and Prevention (CDC) through the national HIV surveillance system, which was upgraded to the China Information System for Disease Control and Prevention (CISDCP) in 2003. 20 Wuhan, the capital city in the Hubei province in central China, has a population of 10.22 million people and developed the web-based reporting system for conventional infectious diseases in September 2003 and then upgraded the system to a special reporting system for AIDS and tuberculosis in 2005.
Before 2003, the information for cases with HIV was sent to the Wuhan CDC via email. The information was then manually entered into the system after the reporting system was developed. 21 Demographic characteristics, HIV diagnosis, AIDS diagnosis, and CD4 cell count were extracted from the database, as described in our previous study. 21 Subjects who were (1) reported by the Wuhan CDC, (2) Wuhan residents, (3) aged older than 13 years at diagnosis, and (4) confirmed to be HIV-infected by a positive Western blot were included in our study. A total of 980 cases with HIV met the inclusion criteria.
Outcomes and definitions
AHD and late entry to HIV care were mainly used as the indicators of late presentation of HIV infection. We defined AHD as presence of a first-reported CD4 count <200 cells/μL or an AIDS-defining event within 1 month of HIV diagnosis, referring to European consensus definition. 5,6 The time between the first positive Western blot test and the first-reported CD4 cell count was used to indicate the interval from initial diagnosis of HIV to the first HIV-related medical care visit. 22,23
HIV infectors and AIDS patients were followed up every 6 and 3 months, respectively. Thus, we defined late entry to HIV care as patients with a first-reported CD4 cell count >6 months after diagnosis. Since the CD4 cell count tests were not conducted before 2003 in Wuhan, cases diagnosed before 2003 were excluded in the analysis of late entry to care. Individuals without CD4 cell count were also were categorized as cases with late entry to care. Patients with HIV infection who progressed to AIDS within 1 year of diagnosis and short-term mortality, which was defined as death from any cause within 1 year of HIV diagnosis were also used as references for the timing of HIV diagnosis. 9,10
Statistical analysis
Descriptive results for continuous variables are expressed as medians and interquartile ranges (IQRs). The entire period 1994–2002 (pre-2003) was used due to the small number of cases diagnosed. A contingency table was applied to assess the linear trend by year for the proportions of AHD and late entry to HIV care. Spearman rank correlation coefficients (rs ) were used to evaluate the correlation between the two selected variables.
Univariate and multivariate non-conditional logistic regression analyses were applied to explore the potential factors associated with late presentation and AIDS within 1 year of diagnosis. Variables in the models included age, sex, marital status, education, transmission category, sample source, occupation, and district. The adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were computed in the multivariate non-conditional logistic regression analyses after adjusting for variables that were statistically significant in the univariate analyses (plus sex). All hypothesis tests were two-tailed with α=0.05. A contingency table was applied to assess the linear trend in the proportion of late presentation among the strata of selected variables. Data analyses were performed using SPSS (version 12.0; SPSS Inc., Chicago, IL).
Ethical considerations
The study was approved by the institutional review board of Tongji Medical College of Huazhong University of Science and Technology. Written consent was obtained from the Wuhan CDC, which approved the use of data for this study.
Results
A total of 980 cases with HIV were diagnosed between 1994 and February 2012 in residents of Wuhan, China. Men were diagnosed more frequently than women (sex ratio: 4.54). The median age at HIV diagnosis was 36 years, ranging from 17 to 85 years (IQR: 27–47 years old). The majority of patients had attained a secondary education (61.53%) and lived in the central districts of the city (87.96%). Single, married, and widowed/divorced individuals accounted for 41.43%, 32.14%, and 26.43%, respectively.
Sexual contact was the main route of HIV transmission: 40.71% of cases involved men who had sex with men (MSM), and 41.12% involved heterosexual contact (HC). Over half (57.14%) of the patients were diagnosed at medical institutions, and only 16.02% were diagnosed because of Voluntary Counseling and Testing (VCT). About one-fifth (20.82%) of the patients were farmers/workers, and 39.39% were business/service employees (Table 1).
Adjusting for factors statistically significant in the univariate analysis.
Primary: illiterate or primary school, Secondary: middle school, high school or technical secondary school.
Blood, blood transfusion or blood products; HC, heterosexual contact with a high-risk individual or person with HIV infection or AIDS; IDU, injection drug user; MSM, men who had sex with men.
Medical institutions, hospitals, STD clinics, et al. Special project, MSM project, China-Gates foundation AIDS project, and other special survey; VCT, Voluntary Counseling and Testing.
Advanced HIV disease
Of the 980 cases with HIV, 289 (29.49%) were diagnosed as AHD. Among 289 cases presenting with AHD, 194 cases presented with a first-reported CD4 count <200 cells/μL and the other 95 cases presented with AIDS-defining event (including 51 cases without CD4 cell count). The percentage of patients diagnosed with AHD increased with age (χ2 for trend=17.167, p<0.001) and decreased with educational attainment (χ2 for trend=16.722, p<0.001) (unknown excluded).
Results of the univariate logistic analyses showed that sex, age, marital status, education, transmission category, sample source, and occupation had a significant influence on the diagnosis of AHD. The multivariate analysis showed that older individuals were more likely to be diagnosed with AHD (30- vs. <30 years: OR=1.76, 95% CI, 1.11–2.79; 50- vs. <30 years: OR=2.03, 95% CI, 1.14–3.62). HC presented higher risk of diagnosis with AHD compared with MSM (OR=1.82, 95% CI: 1.18–2.81). Blood transfusion or blood products (blood) presented a 2.99-fold higher risk of diagnosis with AHD compared with MSM (OR=3.99, 95% CI: 2.05–7.75). Patients diagnosed because of special projects (MSM project, China-Gates foundation AIDS project, and other special surveys) were less likely to be diagnosed with AHD compared with those diagnosed because of VCT (OR=0.23, 95% CI: 0.11–0.47) (Table 1).
AIDS within 1 year of HIV diagnosis
Among all patients, 386 (39.39%; including 289 diagnosed with AHD) progressed to AIDS within 1 year of HIV diagnosis. The percentage that progressed to AIDS within 1 year of HIV diagnosis increased with age (χ2 for trend=17.233, p<0.001) and decreased with educational attainment (χ2 for trend=20.904, p<0.001) (unknown excluded). Univariate logistic analyses showed that sex, age, marital status, education, transmission category, sample source, occupation, and district had a significant influence on progression to AIDS within 1 year of HIV diagnosis.
After adjusting for factors statistically significant in the univariate analyses, the multivariate analysis showed that older individuals had a higher risk of progression to AIDS within 1 year of HIV diagnosis than younger individuals (30- vs. <30 years: OR=2.04, 95% CI, 1.34–3.11; 40- vs. <30 years: OR=2.00, 95% CI, 1.22–3.29; 50- vs. <30 years: OR=1.76, 95% CI, 1.02–3.05). HC and blood presented a greater risk of developing AIDS within 1 year of HIV diagnosis compared with MSM (HC vs. MSM: OR=1.50, 95% CI, 1.00–2.23; blood vs. MSM: OR=2.91, 95% CI, 1.50–5.65).
Injection drug users (IDU) were less likely to develop AIDS within 1 year of HIV diagnosis than MSM cases (OR=0.42, 95% CI: 0.22–0.81). Patients diagnosed because of special projects were less likely to develop AIDS within 1 year of HIV diagnosis compared with those diagnosed due to VCT (OR=0.42, 95% CI: 0.24–0.74). Business/service employees presented a lower risk of developing AIDS within 1 year of HIV diagnosis compared with farmers/workers (OR=0.57, 95% CI: 0.38–0.85) (Table 2).
Adjusting for factors statistically significant in the univariate analysis.
Primary, illiterate or primary school; Secondary, middle school, high school or technical secondary school.
Blood, blood transfusion or blood products; HC, heterosexual contact with a high-risk individual or person with HIV infection or AIDS; IDU, injection drug user; MSM, men who had sex with men.
Medical institutions, hospitals, STD clinics, et al. Special project, MSM project, China-Gates foundation AIDS project, and other special survey; VCT: Voluntary Counseling and Testing.
Late entry to HIV care
As shown in Table 3, the overall proportion of late entry to HIV care was 20.84% (199/955), since 25 cases diagnosed before 2003 were excluded. Among 199 cases with late entry to care, 93 cases were with a first-reported CD4 cell count >6 months after diagnosis, and the other 106 cases without CD4 cell count. The median CD4 cell count of patients with prompt entry to HIV care (first-reported CD4 cell count within 6 months of diagnosis) was 303.50 cells/μL (IQR: 153.75–450.25) from 2003 to 2011.
Adjusting for factors statistically significant in the univariate analysis (plus sex).
Primary: illiterate or primary school, Secondary: middle school, high school or technical secondary school.
Blood, blood transfusion or blood products; HC, heterosexual contact with a high-risk individual or person with HIV infection or AIDS; IDU, injection drug user; MSM, men who had sex with men.
Medical institutions, hospitals, STD clinics, et al. Special project, MSM project, China-Gates foundation AIDS project, and other special survey; VCT, Voluntary Counseling and Testing.
As shown in Fig. 1a, the median CD4 cell count of patients with prompt entry to HIV care ranged from 65.00 cells/μL in 2004 to 373.00 cells/μL in 2008. The median CD4 cell count of patients with prompt entry to HIV care was negatively correlated with the proportion of late entry to HIV care (rs =−0.118, p<0.01) (Fig. 1a and b). The percentage of late entry to HIV care increased with age (χ2 for trend=6.008, p=0.014) and decreased with educational attainment (χ2 for trend=28.790, p<0.001) (unknown excluded). Univariate logistic analyses showed that age, marital status, education, transmission category, sample source, and occupation had a significant influence on late entry to HIV care.
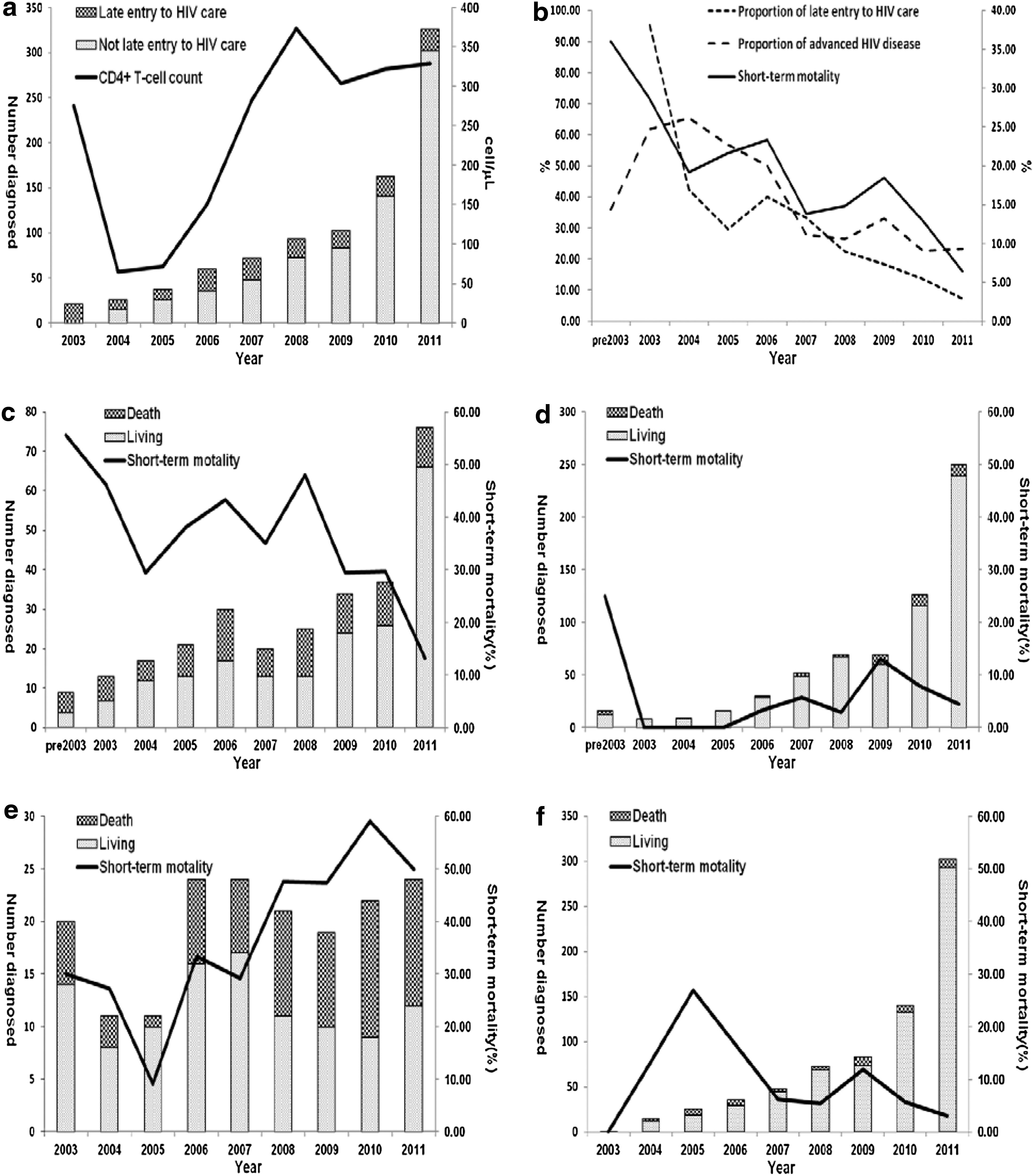
Temporal trend for number, proportion of advanced HIV disease and late entry to HIV care and short-term mortality among HIV infectors diagnosed from pre2003 to 2011 in Wuhan, China.
After adjusting for factors that were statistically significant in the univariate analyses (plus sex), the multivariate analysis showed that younger individuals had a lower risk of late entry to HIV care compared with older individuals (<30 vs. ≥60 years: OR=0.34, 95% CI, 0.14–0.82; 30- vs. ≥60 years: OR=0.27, 95% CI, 0.12–0.59; 40- vs. ≥60 years: OR=0.37, 95% CI, 0.17–0.81; 50- vs. ≥60 years: OR=0.38, 95% CI, 0.17–0.83). HC, blood, and IDU presented higher risks of late entry to HIV care compared with MSM (HC vs. MSM: OR=2.27, 95% CI, 1.31–3.92; blood vs. MSM: OR=7.40, 95% CI, 3.46–15.83; IDU vs. MSM: OR=5.53, 95% CI, 2.69–11.34). Patients diagnosed from unknown/other sample sources presented higher risk of late entry to HIV care compared with those diagnosed because of VCT (OR=3.48, 95% CI: 1.69–7.16). However, professionals/managers had lower risks of late entry to HIV care compared with farmers/workers (professionals/managers vs. farmers/workers: OR=0.45, 95% CI, 0.66–1.84).
Short-term mortality
A total of 171 patients diagnosed between 1994 and 2011 died, among whom 127 (74.27%) died within 1 year of diagnosis. Subjects diagnosed with AHD were 5.75 times more likely to die within 1 year of diagnosis than were those diagnosed promptly (30.85% vs. 6.20%; OR=6.75, 95% CI: 4.49–10.15) (Fig. 1c and d). Subjects with late entry to HIV care had, on average, a 7.91 times higher risk of dying within 1 year of diagnosis compared to those with prompt entry to HIV care (39.20% vs. 6.75%; OR=8.91, 95% CI: 5.86–13.55) (Fig. 1e and f).
The proportion of subjects with AHD showed a downward trend from pre-2003 to 2011 (χ2 for trend=41.199, p<0.001), as did the proportion of those with late entry to HIV care from 2003 to 2011 (χ2 for trend=120.786, p<0.001) and short-term mortality from pre-2003 to 2011 (χ2 for trend=31.447, p<0.001). Short-term mortality decreased as the proportion of AHD (rs =0.668, p<0.01) and late entry to HIV care decreased (rs =0.817, p=0.007) (Fig. 1b).
Discussion
From 1994 to February 2012, the proportions of HIV patients diagnosed with AHD, who developed AIDS within 1 year of HIV diagnosis, and with late entry to HIV care were 29.49%, 39.39%, and 20.84%, respectively. Of the 171 patients who died between 1994 and 2011, 74.27% died within 1 year of HIV diagnosis. Therefore, although ART has been applied in China since 2003 and has improved the progression of PLWHA, 24 late diagnosis of HIV still remains a public health concern in China 19 and other parts of the world. 17
Previous studies have shown that 22.6–70% among people who present to institutions for the HIV care and treatment already have AHD at the first visit. 4,5 A previous cross-sectional study in China showed that 72.02% of patients newly diagnosed with HIV had a CD4 count ≤200 cells/μL at the time of HIV diagnosis. 19 The much lower proportion of HIV patients diagnosed with AHD in our study might be explained by the difference in socio-economic and demographic characteristics between the two studies. The median CD4 cell count of patients with prompt entry to HIV care (303.50 cells/μL, IQR: 153.75–450.25) between 2003 and 2011 was negatively correlated with the proportion of late entry to HIV care (rs =−0.118, p<0.01), revealing the importance of encouraging prompt entry into care before the late stages that are characterized by lower CD4 cell counts.
Late presentation has been associated with a significantly increased incidence of AIDS or death, 9 particularly in the first year after HIV diagnosis, 25 which is supported by the high proportion (74.27%) of deaths within 1 year of diagnosis in the present study. The decreasing trend in short-term mortality, proportion of AHD from pre-2003 to 2011, and late entry to care from 2003 to 2011 should be regarded as a positive achievement of the considerable efforts and policies aimed at reversing the HIV epidemic in China. 26
Older age has been recognized as an independent factor associated with delayed HIV diagnosis and late entry to care, which was confirmed by our findings. 10,27 –29 It is likely that various factors result in late testing, including a lower perception of risk, missed opportunities in healthcare settings, and limited sexual health information targeting older adults. 27,30 In addition, the more rapid disease progression in older individuals might contribute to greater likelihood of AIDS diagnosis within 1 year. 31
Some studies have indicated that men are more likely to present with AHD and late HIV diagnosis, 32 –34 whereas others have indicated no sex differences, which was supported by our present findings. 35,36 The lack of disparity between men and women in AHD, late entry to care, or AIDS diagnosis within 1 year in the present study might be attributable to the smaller number of women.
In terms of marital status, married patients are more likely to present earlier compared with single, separated, or widowed individuals, particularly among women. 37 However, marital status was not associated with late HIV diagnosis in the present study, which is consistent with a previous study conducted in Thailand. 38
Late HIV diagnosis was less common when transmission occurred via MSM than with other routes, 39,40 which might be due to outreach programs aimed at promoting testing or research studies that include testing in MSM. 41 Furthermore, MSM might be associated with a higher probability of undergoing HIV testing owing to a higher perception of risky sexual behavior. 19 In addition, IDU might be excluded from HIV services because of stigma, discrimination, criminalization, 39 and barriers in healthcare, 40 resulting in a higher risk of late HIV diagnosis and entry to care. In our study, IDU were less likely to progress to AIDS within 1 year following HIV diagnosis compared with MSM, which might be related to the younger ages of IDU than MSM (median age: 30.00 vs. 37.5 years, p<0.05). 42
Low socio-economic status has also been correlated with late presentation, 17 and educational attainment is associated with late HIV diagnosis and delayed initiation of treatment. 37,43,44 However, another study showed that low educational attainment with free and equal access to healthcare was not associated with late or very late presentation of HIV, time to HAART initiation, or HAART response, consistent with the findings of the multivariate analysis in our study. 45 However, low educational attainment might increase the risk of HIV diagnosis among heterosexual individuals, and substantially increase lifestyle-related mortality, indicating that the increased mortality in HIV-infected patients with low educational attainment could mainly be attributed to risk factors unrelated to HIV, such as greater consumption of tobacco or alcohol. 45,46 Owing to a lack of HIV knowledge, lower perception of HIV infection, and structural barriers to seeking care in a rural setting, farmers and workers, as well as those living in suburbs might also have a higher risk of late diagnosis. 37,47
In China, diagnosis of HIV primarily occurred in severe or acute clinical circumstances, high-risk groups, blood donors, or VCT. 19 In our study, over half (57.14%) of PLWHA were diagnosed in medical institutions, while only 16.02% were diagnosed in VCT. Patients diagnosed through special projects had a lower risk of AHD and AIDS within 1 year than did those diagnosed in VCT, which might be due to the fear of stigma and discrimination that acts as a major barrier to agreeing to have VCT. 48 Therefore, increased efforts to increase access to VCT and improve awareness of HIV and active acceptance of VCT among the general public are needed. 19,48,49
The main strength of our study is the comprehensive analysis of risk factors for AHD and late entry to care, with reference to consensus definitions, 5,23 using HIV surveillance data. AHD reflects patients who are unaware of their HIV infection and are not tested until their CD4 cell count has declined or until AIDS-related symptoms appear, while late entry into care is reflective of individuals who are conscious of their HIV status but choose not to seek HIV-related care. 25 The analysis of AIDS within 1 year of diagnosis and short-term mortality are additional strengths, which provide complementary evidence of the consequences of late presentation. 9,50
Some limitations must be noted. Data on viral load were not available, although this is also an indicator of late entry to HIV care. 23 Increased engagement in care was associated with improved viral suppression, and was related to decreased risk of HIV transmission to others. 51 The generalizability of our findings may be limited to regions with similar socio-economic status because the study sample was restricted to residents of Wuhan, a metropolitan area of a million people in central China; however our study still highlights the importance of late HIV diagnosis in China.
In conclusion, the proportions of HIV patients in residents of Wuhan who were diagnosed with AHD, who progressed to AIDS within 1 year of HIV diagnosis, and who entered late into HIV care between 1994 to February 2012 were 29.49%, 39.39%, and 20.84%, respectively. AHD and late entry to HIV care were associated with a significantly increased incidence of AIDS or death, particularly in the first year after HIV diagnosis. Short-term mortality, proportion of AHD, and late entry to care showed a similar downward trend from pre-2003 to 2011. The findings of our study suggest that more attention should be directed towards patients at risk of AHD and late entry to HIV care, and more efforts should be made to assure early diagnosis and timely entry into care.
Footnotes
Acknowledgments
We acknowledge the staff in the Wuhan Centers for Disease Control, who spent many hours working with us in obtaining, verifying, and cleaning the data used in this study.
Author Disclosure Statement
There is no support or conflicting funding to report.