
Abstract
We investigated the implementation feasibility and effectiveness of community-based HIV home-test voucher distribution in three Indianapolis African American communities. Community-based organizations augmented traditional outreach methods to distribute vouchers for home HIV tests redeemable at three pharmacies during three distribution waves from February to April 30, 2015. Voucher redemption served as a proxy indicator of intent to test for HIV. 315 vouchers were distributed and 47 vouchers were redeemed for a 14.9% redemption rate. Distribution was 46% of plan. Vouchers were redeemed at all three pharmacies, and 21% of visits involved redemption of more than one voucher. The original team of seven distributors in three organizations reduced to a remaining five distributors in two organizations by wave 2. This study suggests that outreach organizations could implement HIV home test voucher distribution, and that people would redeem the vouchers at a pharmacy for an HIV test. Future studies should explore how voucher distribution can expand the current HIV testing system.
Introduction
T
Gay and bisexual patients were at a particular disadvantage, as standard of care/routine screening practices were lowest for this population. These findings are significant because in Indiana, and elsewhere, HIV health inequity is experienced intensively by men of color who have sex with other men, and by injection drug users due to institutionalized homophobia and abstinence-based sexual health and drug use policy. 4
The 2012 FDA approval of home HIV tests created the opportunity to consider how current public health systems could integrate access to HIV testing via pharmacies. This is particularly important for racial and sexual minorities that disproportionately experience HIV and are often marginalized from full participation in the health system because of structural stigma. Pharmacies have been found to increase access to HIV testing by racial and sexual minorities, as well as injection drug users. 5 Exploring these opportunities in Indiana has enhanced the understanding of whether a lower HIV incidence state with a modest public health system infrastructure could support this alternative access to HIV testing.
Our recent studies among Indiana pharmacists found that they supported expanding services to include HIV testing,
6
and they valued over-the-counter HIV tests (also called ‘home HIV tests’) as an access opportunity especially for populations stigmatized about HIV.
7
Preference for home HIV tests through pharmacies has been expressed by gay and bisexual men in Indiana
8
and elsewhere;
9
–17
however, the price of a test is high (
We hypothesize a voucher, or payment coupon, for an HIV home test at pharmacies might ameliorate access barriers to HIV testing. A recent Los Angeles study found that HIV home test vouchers were redeemed by the population targeted by them, and surmised that such access would likely help to identify people with HIV who otherwise would not have known their status. 18 These findings reflect other voucher studies aimed at increasing sexual health screening 19 and access to reproductive health services. 20,21
A 2010 study by Cameron and colleagues to evaluate the effectiveness of vouchers for expedited partner therapy for Chlamydia found that voucher-based pharmacy access programs reduced stigma for people who did not wish to access services at an STD (or GUM) clinic. 22 While these studies support the use of vouchers to increase services access, an important yet unstudied component is the implementation aspect of the voucher programs. Specifically, whether outreach-oriented community-based HIV organizations can shift intervention modalities to integrate an individually focused or consumer/patient-driven voucher distribution program.
Voucher distribution is not like condom distribution or distribution of social marketing materials for two reasons. First, cost per unit is significantly higher for HIV home tests, and second, distribution is not solely about handing a person a voucher for a free HIV test. If cost were the only barrier to testing, then people would access the testing services freely provided in communities that are fortunate to have such resources. Stigma, system brokenness, and lack of availability of free HIV tests compound testing access decisions.
The failure of public health and primary care HIV testing in Indiana, combined with local pharmacist openness to pharmacy-based or home HIV testing and the preferences of gay and bisexual men for home HIV testing, led to the current study. While HIV home testing vouchers worked in Los Angeles, could they work in Indiana? The study purpose was to investigate the feasibility of implementing an HIV testing voucher distribution program in three African American communities in Indianapolis, and to evaluate the rate of redemption as an indicator of intent to use the test.
Methods
This study had a community-based participatory research (CBPR) orientation and was led by the African American HIV Action Team (AHIT): a coalition of four community-based organizations serving several Indianapolis African American communities, a pharmacy chain, and a school of public health. Each organization brought expertise in specific areas: gay, bisexual and transgender services; substance abuse prevention and treatment; local public health HIV prevention; community pharmacy services; and community based participatory research. Three of the community organizations provided HIV testing on walk-in and outreach bases.
The several years of experience among AHIT members informed the belief that African Americans were highly stigmatized about HIV testing, and as such would not likely access HIV testing in the community or ask their own doctors for an HIV test. The working hypothesis was if vouchers for free home HIV tests were distributed on a private, individual basis, people would redeem them and likely test for HIV on their own. However, members surmised that distribution would need to be different than traditional outreach in order to result in voucher redemption and ultimately home testing. Therefore, a practice change would need to occur because these organizations were accustomed to providing community-level testing outreach to high-risk populations. Figure 1 depicts the outreach practice change designed by the AHIT team members for study implementation.
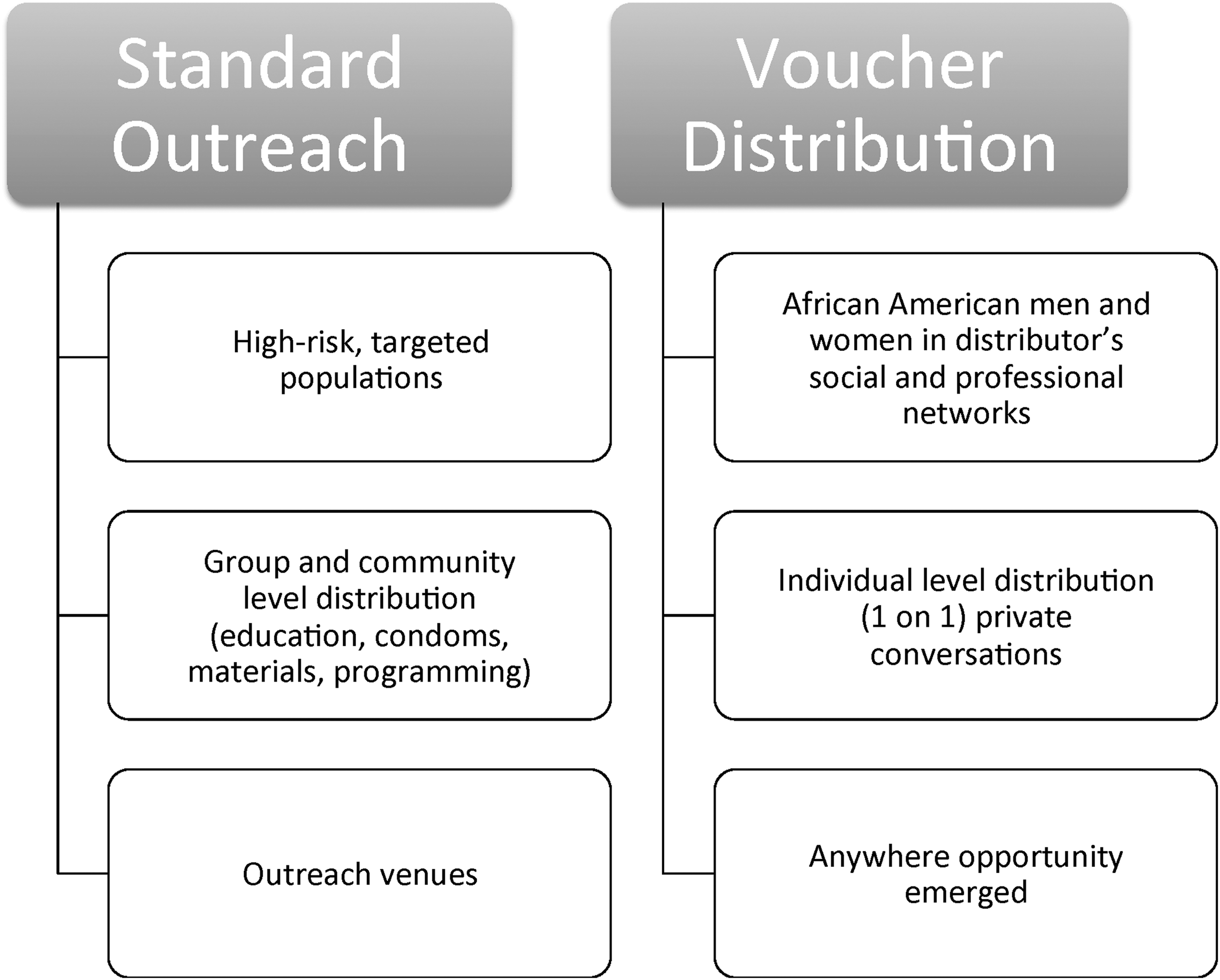
Practice change for HIV test voucher distribution.
This dissemination and implementation study used a Hybrid Type III research design with the following dual implementation and effectiveness aims: (1) to evaluate the feasibility of distributing individualized vouchers for home HIV tests within the social and professional networks of these primarily outreach-based organizations, and (2) to evaluate whether distribution would result in voucher redemption for HIV tests.
Unlike the Los Angeles study, this study did not follow up with those who redeemed the vouchers to learn whether tests were actually taken following voucher redemption or to learn about redemption experiences. 18 This was because AHIT members and the study community advisory board felt that in doing so, nothing about the vouchers would be ‘free’ because they would be tied to a form of follow-up generally associated with public health research; and therefore potentially stigmatizing. Thus, as this was a feasibility study, voucher redemption served as a proxy for intent to use the HIV test.
Vouchers were designed for distribution in three separate “waves” or 30-day periods beginning February 1 and ending April 30, 2015. Vouchers had a community building “power over your health” message and were the size of a business card for maximum privacy. Vouchers were uniquely coded by color and number to identify the distribution wave, distributing organization, and the distributer; and could be redeemed at one of three participating Walgreens pharmacies for an Oraquick HIV test kit (Orasure, Bethlehem, PA). Test kits were enhanced by a ‘post-it’ note message affixed to each box that had a 24-h/7-day week text/phone number that connected to a trained HIV test counselor and linkage to care specialist at a participating AHIT organization.
Distribution was measured by weekly voucher counts and experiences reported by distributors. Voucher redemption rates were calculated weekly as a ratio of redeemed vouchers to reported distributed vouchers.
Results
Voucher redemption
Over the course of the three waves, 315 vouchers were distributed and 47 were redeemed for a redemption rate of 14.9%. Wave 1 redemption rate was 12.9%, wave 2 was 18.9%, and wave 3 was 13.6%. The 47 vouchers were redeemed during 38 visits to the participating pharmacies, as 21% of the visits redeemed two vouchers, with one visit redeeming three vouchers. No calls to the HIV test counselor/Linkage-to-Care specialist were made during the study period.
Vouchers were redeemed at three times of day: morning (6:00 a.m.–12:00 noon), afternoon (12:01 p.m.–6:00 p.m.), and evening (6:00 p.m.–10:00 p.m. or later). Only one pharmacy was open 24 h. Redemption after midnight was coded as evening. Almost half (44.7%) of the vouchers were redeemed during the afternoon.
Voucher distribution
At study start, the distribution team had 7 people from four community organizations; three of which were AHIT members and one was a pastor of a local church who was a member of the community advisory board convened for the research study by the AHIT team. By the end of wave 1, three of the original distributors had dropped out of the study, and one person joined the remaining members of the distribution team. This resulted in a cohort of five distributors who continued as the core distribution team throughout waves 2 and 3. One distributor who left the cohort indicated that she could not continue because her social and professional network was not located near any of the participating pharmacies, the other two actually never distributed vouchers at all because they did not want to adopt distribution as designed. As will be discussed, voucher distribution was a new way of working, and this was not necessarily easy for distributors, given the difference with traditional modes of outreach.
Distributors planned their voucher distribution by wave and ended up distributing 46.0% of what was planned. Planned distribution was determined at the beginning of each wave and by each distributor after considering distribution and redemption patterns of the prior wave.
As noted in Table 1, planned distribution was adjusted downward with each successive wave. In the words of one distributor:
“(At first), I engaged a lot of people. So that was the disadvantage. It took me to get out and do a little more walking and talking to people. It was OK…The questions people asked of me were, ‘where to go, what do I have to do? Where do I use this?’ I gave them some experiences and stories of friends who passed away who didn't get tested. I told them how I felt about it.
–“Carl” who distributed to a “fellowship” of former substance users
Distribution was a different mode of operation for all participants, especially because it did not involve education about HIV or about the test. This type of outreach engagement was a difficult change for distributors because they were used to providing HIV education at any and all outreach opportunities. They were also used to the ‘reward’ of an HIV test as the outcome following community level interventions. Further, the voucher intervention design separated them from testing itself. One distributor initially struggled with not knowing whether ‘her people’ redeemed and then used the test. She came to terms with it this way:
Just because someone takes one (voucher) does not mean that someone will redeem it, take the test or even use the test once redeemed…We (distribution team) think that it is free and therefore cool, and then easy, but that does not necessarily seem that way to other people. There are gray areas, because we are not attached to the redemption, but we kind of are because it is our social network and we do care about them and want to be available. I had so many people who wanted to do it (took a voucher), but they did not redeem…Human behavior is different and we can't think that we know how people feel and respond to it.
–“Donna” who distributed to a network of African American heterosexual women
Discussion
This feasibility study suggests that a voucher outreach program for HIV home testing has potential to work well in Indianapolis African American Communities. It also suggests outreach-based organizations could adapt and successfully shift gears from traditional and likely institutionalized HIV testing outreach methods to include one-on-one HIV testing voucher distribution, especially when designed by the distributors themselves. However, the distribution task and experience of it fluctuated as time progressed, and this likely adjustment may have contributed to reduced distributions over the course of the study. Distributors may have initially overestimated the vouchers they would distribute, especially prior to implementation experience, though learning was evidenced by the reduced estimates of planned distribution in successive waves.
The study also found that vouchers for a free HIV home test would be redeemed, and that this would likely happen in a normalized manner. This is indicated by daytime redemption data. Distributors interpreted this observation to mean that people may not have felt stigmatized about getting a home HIV test because they could access it while doing other business at the pharmacy. One distributor reported supporting evidence for this hypothesis when he experienced redeeming a test for a friend. He reported feeling very comfortable:
The pharmacist acted completely normal and immediately put the test in a regular Walgreens bag like it was nothing. And I heard from others that they had the same experience.
–“Allen” who distributed to young African American heterosexual men and women
Finally, the observation that multiple tests were redeemed almost one quarter of the time suggests the social nature of home testing, or perhaps a secondary distribution of HIV tests. One distributor remarked:
I went to people who know what I do but don't have questions about it because they are “not one of them [the LGBT people that I serve].” So in my cases, people would pretend that they would take it for ‘so and so’ or for a nephew or niece or ‘a good friend of mine.’
–“Luke” who distributed to gay and heterosexual African American men and women
This observation reflects the potential of social networks to leverage social-level HIV prevention such as with the Facebook study by Young et al. among African American and Latino men who have sex with other men. 23 This is also akin to what is seen in secondary syringe exchange networks, where peers obtain the clean syringes and share them within their own networks. 24,25
Finding a balance between voucher distribution and redemption may depend on several factors, including perceived and received societal stigma and decreased risk perception. We cannot discount the fact a voucher-based home HIV testing program may alleviate not only individual financial barriers, but also the stigma associated with attending community based HIV testing and outreach organizations. HIV care providers could integrate this into their array of outreach options and offer a new approach to HIV testing by using existing social networks. Clients who avoid HIV testing because they are afraid to enter a community based clinic may feel more secure using a voucher to get a rapid home test, thus controlling whom, if anyone, is involved in the process. This remains to be understood.
A significant outcome of the Los Angeles study suggests an HIV voucher program is also able to identify individuals who would not have otherwise known their serostatus. 18 Early screening and linkage to care is important if we hope to improve health outcomes associated with HIV. Because individuals who perceive themselves to be at decreased risk for HIV are less likely to test, the use of social networks to distribute vouchers may be an effective means to reach people who believe they are “not one of them”.
This is a particularly significant issue within the African American community where HIV and sexuality are stigmatized because it is largely associated with men who have sex with other men; leaving many to believe they are either not at risk for contracting or spreading HIV or fearful that accepting an HIV test may suggest they are engaging in same sex activity.
While our study suggests that an outreach voucher program for HIV home testing would result in test redemption in African American communities in a Midwestern city, the variables associated with voucher redemption are not clear. Future studies are needed to explore the barriers and facilitators to voucher distribution and redemption, and to understand the experiences of redemption and the use of the HIV test.
In conclusion, this feasibility study suggests that larger studies should follow, and that estimates of the proportion of vouchers needed in a community to sustain access throughout a year and beyond research ‘waves’ would be a helpful translation of research to program implementation. Communities, such as Indiana, where access to HIV testing remains difficult and also stigmatized, may benefit from opportunities to extend the reach of their HIV testing systems to include vouchers. The key is not just to remove the price barrier for people, but to also reduce the price point of the test in order to allow strained public health budgets to handle the cost.
Footnotes
Acknowledgments
This study was funded by the Indiana Minority Health Initiative Funding from the Indiana Minority Health Coalition, Inc.
Author Disclosure Statement
No conflicting financial interests exist.