
Abstract
Metabolic syndrome (MS) is a group of components associated with cardiovascular disease and type 2 diabetes mellitus. The prevalence of MS in the HIV population is increasing in epidemic proportions globally. However, the magnitude and characteristics of MS are not fully elucidated in developing countries. The aim of this systematic review was to assess the prevalence of MS and its components among people living with HIV (PLWH) in developing countries. Searches were carried out in MEDLINE, Embase, Web of Science, CINAHL, Cochrane Central Register of Controlled Trials, Scopus, other web sources, and by hand search. Articles were restricted to English language studies reporting on the prevalence of MS among PLWH in developing countries. Eighteen articles were included in the review. The studies were divided into Africa, South America, and Asia regions. The most frequent criterion used in the review was the National Cholesterol Education Program: Adult Treatment Program III 2001 definition. The prevalence of MS among PLWH ranged from 8.4% to 47% across the developing regions and comparable to the overall prevalence across the developed regions (7.8–52.2%). The mean prevalence was 30.5%, 21.5%, and 21.4% in Africa, Asia, and South America, respectively. The most frequent component observed was low high-density lipoprotein cholesterol (50.1%). This systematic review provides an essential overview on the distribution of MS in the HIV population across the developing regions. As these prevalences were comparably high in the developed regions, this review highlights the need for more robust research in developing countries.
Introduction
M
The prevalence of MS has exploded to epidemic proportions in almost all countries around the globe and, thus, MS is regarded as a clinical and public health crisis. MS results in two times the risk to develop CVD and five times the risk to develop DM in the general population. 6 The impact of MS in the general population has now extended to the HIV population. The decline in AIDS-related morbidity and mortality among people living with HIV (PLWH) by highly active antiretroviral therapy (HAART) has influenced the emergence of a number of metabolic derangements that resemble MS in the general population. 7,8 Reports from the developed countries suggest that although the estimates of prevalence are critically dependent on the definition used, the prevalence of MS among PLWH is now comparable to the general population. 9 –12
In addition to aging, there may be additional factors that increase the risk of MS among PLWH, as compared with the general population. 13 These factors however, are yet to be fully explored. PLWH develop metabolic complications and consequent MS at a younger age, as compared with the non-HIV population. 14,15 The accelerated metabolic complications among PLWH are also compounded by the adverse effects of HIV infection per se and HAART. 16 To some extent, the rising incidence of MS in resource-limited settings is complicated by the use of older drugs within the antiretroviral therapy (ART) classes, particularly ritonavir within the protease inhibitors (PIs) and stavudine within the nucleoside reverse transcriptase inhibitors (NRTIs). 17,18
The problems associated with MS in the HIV population highlight future directions and implications for the HIV epidemic, especially in the developing countries. This is an important issue, given the rise in noncommunicable diseases generally in such settings, especially DM and consequent CVD. 19 Despite the importance of MS in HIV, the magnitude and characteristics of MS and its associated risk factors in this population in the developing countries is not fully elucidated. This systematic review aims to assess the prevalence of MS and the pattern of the associated risk factors among PLWH in developing countries.
Materials and Methods
Search strategy
The search strategy was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. A total of 8125 records were retrieved from six searched databases. The search started on March 2014. The assessed databases were MEDLINE (628), Embase (3218), Web of Science (437), CINAHL (3043), Cochrane Central Register of Controlled Trials (17), and Scopus (782). The search included the MeSH terms HIV, prevalence, and MS. We also searched through other web sources and hand search to obtain relevant articles (10). The initial search was not limited by language and year. English language studies were filtered after retrieval of full text articles (last update: April 2015).
Study selection
We included English language studies that reported on the prevalence of MS among PLWH across the developing regions. Developing countries were defined according to the Gross National Income (GNI) per capita per year. Countries with GNI of US$ 11,905 or less were classified as developing countries. 20 Of the 68 studies assessed, 50 were excluded for the following reasons: 34 were carried out in developed countries, 6 reported on the general population, 3 had insufficient data, 3 were review articles, 2 reported on the incidence of MS, and 2 were non-English language articles. Accordingly, 18 studies were included in our systematic review.
Data extraction
The abstracts and titles of the retrieved records were evaluated by the corresponding authors (S.N., S.P., and S.B.K.). Potential abstracts that did not provide sufficient details for the inclusion criteria were retrieved for full text evaluation. S.N., S.P., and S.B.K. evaluated full text articles and determined study eligibility. Any uncertainty on the inclusion of the study was forwarded to A.K. and solved through discussion. A.K. also reviewed the eligibility of the included studies to provide better accuracy. Corresponding authors of the included studies were contacted to request data that were not included in the published articles.
The characteristics of the included studies were tabulated in Table 1. The characteristics were the country, authors, total number of subjects, percentage of men (%), mean age (unless stated otherwise), HAART/HIV status, definition for the classification of MS, prevalence of MS (%), and the significant association with p-value less than 0.05. The prevalence of the MS components (%) was tabulated in Table 2. The mean prevalence in this review was calculated as sum of the number of cases ÷ sum of the number subject × 100.
Median.
3TC, lamivudine; AHA/NHLBI, American Heart Association/National Heart, Lung, and Blood Institute; ART, antiretroviral therapy; BMI, body mass index; D4T, stavudine; EFV, efavirenz; HAART, highly active antiretroviral therapy; IDF, International Diabetes Foundation; MS, metabolic syndrome; NA, not available; NCEP-ATP III, National Cholesterol Education Program: Adult Treatment Program III; NNRTI, non-nucleoside reverse transcriptase inhibitor; PA, physical activity; OR, odds ratio; PI, protease inhibitor; RR, risk ratio.
ATP III/AHA/NHLBI or IDF.
Mean.
Systolic blood pressure (≥130 mmHg).
Diastolic blood pressure (≥85 mmHg).
HAART, highly active antiretroviral therapy; HDL, high-density lipoprotein; NA, not available.
Quality of studies
The quality of the included studies was appraised based on the guidelines provided by the National Heart, Lung, and Blood Institute (NHLBI) for observational cohort and cross-sectional studies. Many of the studies had insufficient information for the study methodology. Numerical estimates were missing in some of the studies, leaving us to interpret the results ourselves. Nevertheless, most of the studies were rated as good, with few rated as fair, and one rated as poor.
Results
The search strategy summarized in Fig. 1, provided 8125 records from six searched databases, with additional 10 records from other web sources and hand search. Five hundred ninety (590) records were removed due to duplication, resulting in 7545 records. The titles and abstracts of these records were screened for potential studies, which narrowed the search to 68 records. A further 50 records were eliminated as the studies did not fit the inclusion criteria. Eighteen articles from the year 2008 to 2014, describing the prevalence of MS among PLWH in developing countries were included in this review.
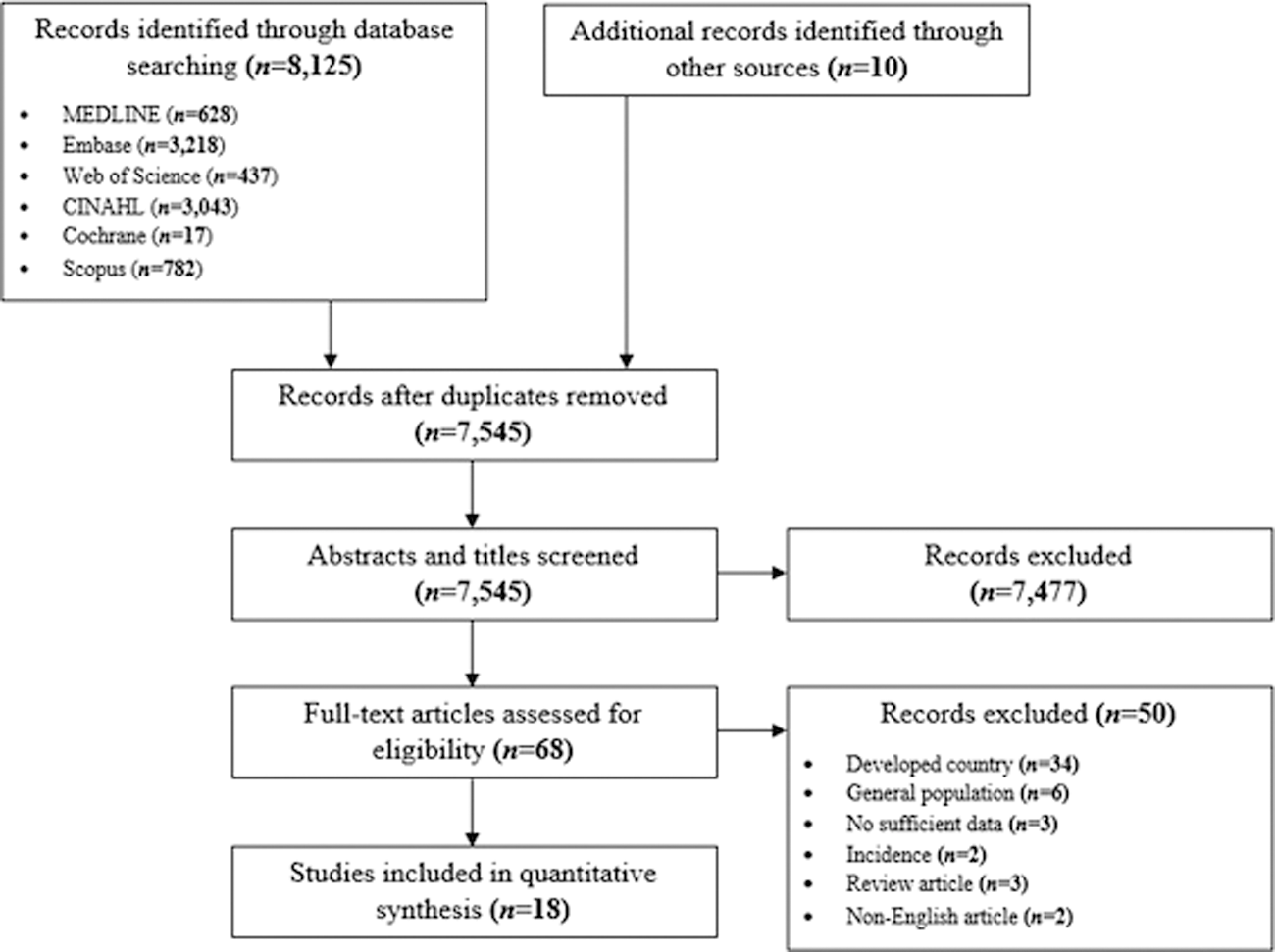
Search strategy flowchart.
Figure 2 illustrates the number of developing countries that have reported on the prevalence of MS among PLWH.
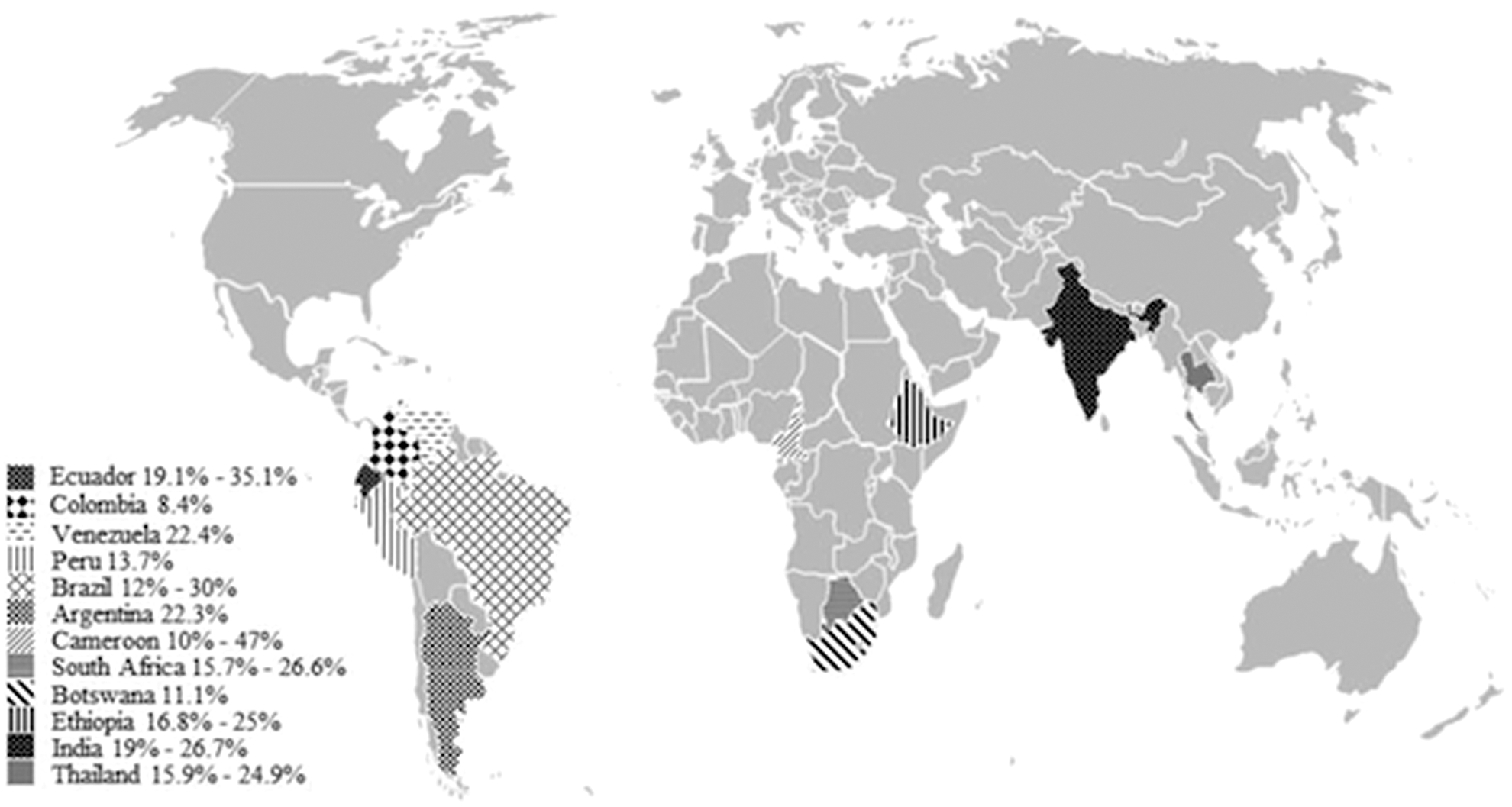
Developing countries that have reported prevalence of metabolic syndrome among people living with HIV.
The information tabulated in Table 1 summarizes the results of the 18 included studies. All of the studies were cross-sectional studies. The total number of subjects was 9638 HIV individuals from the outpatient population visiting the HIV clinics. One study did not report on the total number of men and women. 21 Of the 17 studies that did report on the gender distribution (9438 HIV individuals), 54.4% of the subjects were males and 45.6% were females. 22 –38 The mean age of the HIV individuals in this review were between 30 and 45 years of age.
Various criteria were used to diagnose MS. Of the 18 studies, 7 studies used the criteria proposed by NCEP-ATP III (2001), 21,23 –25,27,30,37 3 studies used ATP III/AHA/NHLBI (2005), 32,36,38 2 studies used IDF (2005), 28,35 1 study used HARMONIZED (2009), 31 2 studies used both NCEP-ATP III (2001) and IDF (2005), 29,33 2 studies used both ATP III/AHA/NHLBI (2005) and IDF, 26,34 1 study used NCEP-ATP III (2001), IDF (2005), and ATP III/AHA/NHLBI (2005). 22
The NCEP-ATP III 2001 definition requires the presence ≥3 of the following components: low HDL cholesterol ≤1.03 mmol/L (40 mg/dL) for men and ≤1.29 mmol/L (50 mg/dL) for women, hypertriglyceridemia ≥1.7 mmol/L (150 mg/dL), hypertension ≥130/85 mmHg, hyperglycemia ≥6.1 mmol/L (110 mg/dL), or abdominal obesity ≥102 cm (40 inches) for men and 88 cm (35 inches) for women. The NCEP-ATP III 2001 definition updated by the AHA/NHLBI in 2005 (ATP III/AHA/NHLBI 2005) reduced the threshold for hyperglycemia from ≥6.1 mmol/L (110 mg/dL) to ≥5.6 mmol/L (100 mg/dL). The IDF definition requires the presence of abdominal obesity adjusted by recommended ethnic-specific waist cut-off value, as a prerequisite component in the diagnosis of MS. The HARMONIZED definition has similar set of criteria as the IDF definition. However, the HARMONIZED definition places equal emphasis on all of the five components of the MS.
The methods of measurements of the individual components of MS were not elucidated in all of the included studies. HDL cholesterol, triglycerides, and glucose were measured from ≥8 h fasting blood. 21,22,25,26,29 –35,37,38 Blood pressure was either measured using automated or manual blood pressure at a seated position. 22,25,26,29,30,33 The waist circumference was measured at the midpoint between iliac crest and lower costal margin. 22,25,29,33,34,37
Prevalence of metabolic syndrome
Overall, the prevalence of MS among PLWH in developing countries ranged from 8.4% in Colombia to 47% in Cameroon (Table 1).
In South America, the prevalence of MS ranged from 8.4% in Colombia 27 to 35.1% in Ecuador. 26 The mean prevalence of MS among PLWH in South America was 21.4%.
The prevalence of MS in the African region ranged from 11.1% in Botswana 28 to 47% in Cameroon. 31 The mean prevalence of MS among PLWH in Africa was 30.5%.
The prevalence of MS in the Asian region varied from 19.1% to 26.7% in India, 36,37 and 22.2% in Thailand. 38 The mean prevalence of MS among PLWH in Asia was 21.5%.
With regard to ART, the study population in this review was heterogeneous. Of the 18 studies, 6 studies assessed patients on HAART, 23,25,27,28,32,35 1 study assessed on HAART-naive, 31 and 11 studies included both HAART and HAART-naive. 21,22,24,26,29,30,33,34,36 –38
Of the 18 studies, 8 studies assessed and compared the prevalence of MS among individuals on HAART and HAART-naive. 21,24,29,30,33,34,36,38 Seven studies reported a higher prevalence of MS among those on HAART. 21,24,29,30,33,34,38 Bajaj et al. reported a lower prevalence of MS among individuals on HAART compared with individuals who were HAART-naive (19.1% vs. 21.7%). 36
Three studies from Africa, 30,31,34 and one study from India, 21 assessed and compared the prevalence of MS among PLWH and non-HIV individuals. Mbunkah et al., 30 Awotedu et al., 34 and Mital et al. 21 reported a higher prevalence of MS among HAART and HAART-naive compared with the non-HIV population (15.6% vs. 8%; 22.9% vs. 19.3%; 20% vs. 7.5%). Similarly, Ngatchou et al. found that the prevalence of MS was 47% among the HAART-naive individuals and 21% among the non-HIV individuals. 31 All of the four studies showed an increased prevalence of MS in the HIV population irrespective of treatments.
Of the 18 studies, 10 studies adjusted the prevalence of MS according to gender. 22,24,26,29,30,32,33,35,37,38 Eight studies reported a higher prevalence of MS among women (19.2% vs. 15.2%; 46.8% vs. 26.9%; 44.4% vs. 19%; 23% vs. 17.4%; 28.2% vs. 15.1%; 18.7% vs. 5.1%; 24.1% vs. 7.5%; 26% vs. 17.9%). 22,26,29,30,32,33,35,38 Silva et al. 24 and Bajaj et al. 36 found that the prevalence of MS among women were lower than men (13.7% vs. 16.3%; 15% vs. 45%).
Prevalence of metabolic syndrome components
The prevalence of the individual components of MS among PLWH was tabulated in Table 2. Of the 18 studies, 11 studies reported the prevalence of all the components of MS. 22 –26,28 –30,32,36,38 Study by Cahn et al. only reported the prevalence of low HDL cholesterol, hypertension, and abdominal obesity. 27 Julius et al. did not assess the prevalence of hyperglycemia because fasting blood glucose (FBG) was not measured in the study. However, they did report on the prevalence of DM. 35 Awotedu et al., 34 Idiculla et al., 37 and Tesfaye et al. 33 did not document the overall prevalence of hypertension, but reported on the prevalence of high systolic and diastolic blood pressures, respectively. Ngatchou et al. 31 and Mital et al. 21 reported all components as mean. The mean was documented as HDL cholesterol mmol/L, triglycerides mmol/L, systolic and diastolic blood pressure mmHg, FBG mmol/L, and waist circumference cm.
Low HDL cholesterol
The prevalence of low HDL cholesterol was reported in 16 studies. 22 –30,32 –38 The prevalence ranged from 6.3% in Botswana 28 to 100% in India. 37 The mean prevalence of low HDL cholesterol in the 16 studies was 50.1%. The mean prevalence of low HDL cholesterol in South America, Africa, and Asia was 50.1%, 32.8%, and 53.2%, respectively. The differences in prevalence of low HDL cholesterol between individuals on HAART and HAART-naive were compared in seven studies. 24,29,30,33,34,36,38 Five studies reported higher prevalence of low HDL cholesterol among HAART-naive. 24,30,33,34,38
Hypertriglyceridemia
The prevalence of hypertriglyceridemia was reported in 15 studies. 22 –26,28 –30,32 –38 The prevalence ranged from 11.5% in Cameroon 30 to 93.8% in India. 37 The mean prevalence of hypertriglyceridemia in the 15 studies was 45.7%. The mean prevalence of hypertriglyceridemia in South America, Africa, and Asia was 54.4%, 24.9%, and 45.8%, respectively. The differences in prevalence of hypertriglyceridemia between individuals on HAART and HAART-naive were compared in seven studies. 24,29,30,33,34,36,38 All the seven studies reported a higher prevalence of hypertriglyceridemia among those on HAART.
Hypertension
The prevalence of hypertension was reported in 13 studies. 22 –30,32,35,36,38 The prevalence ranged from 12.5% 25 to 78.8% in Brazil. 23 The mean prevalence of hypertension in the 13 studies was 32.3%. The mean prevalence of hypertension in South America, Africa, and Asia was 35.2%, 21.6%, and 24.8%, respectively. The differences in prevalence of hypertension between individuals on HAART and HAART-naive were compared in 5 studies. 24,29,30,36,38 Four studies reported a higher prevalence of hypertension among those on HAART. 29,30,36,38
Abdominal obesity
The prevalence of abdominal obesity was reported in 16 studies. 22 –30,32 –38 The prevalence ranged from 0% in India 36 to 64.2% in South Africa. 34 The mean prevalence of abdominal obesity in the 16 studies was 23%. The mean prevalence of abdominal obesity in South America, Africa, and Asia was 19.8%, 20.9%, and 26.8%, respectively. The differences in prevalence of abdominal obesity between individuals on HAART and HAART-naive were compared in seven studies. 24,27,29,30,33,34,36 Six studies reported a higher prevalence of abdominal obesity among those on HAART. 24,29,30,33,34,36
Hyperglycemia
The prevalence of hyperglycemia was reported in 15 studies. 22 –26,28 –34,36 –38 The prevalence ranged from 7% in Brazil 24 to 48.6% in Cameroon. 29 The mean prevalence of hyperglycemia in the 14 studies was 22.5%. The mean prevalence of hyperglycemia in South America, Africa, and Asia was 21.4%, 18.1%, and 23.4%, respectively. The differences in prevalence of hyperglycemia between individuals on HAART and HAART-naive were compared in seven studies. 24,29,30,33,34,36,38 Five studies reported a higher prevalence of hyperglycemia among those on HAART. 24,30,33,34,38
Factors associated with metabolic syndrome in HIV
Of the 18 studies, 8 studies assessed the associations between MS and the possible risk factors. 22,23,26,28,32 –34,38 The risk of MS in this review was found to increase significantly with body mass index (BMI), age, marital status, duration of ART, type of regimens, gender, lipodystrophy, high cholesterol, and food insecurity (Table 1). The most common associations were observed with BMI, age, and gender.
Of the eight studies, four studies reported increased risk of MS with BMI. 22,23,28,33 Malangu reported that odds of developing MS was 16 times higher among HIV individuals who were obese [odds ratio (OR) 16.16 (5.44–47.98)] than those who were not obese. 28 Tesfaye et al. reported that the risk of MS was about 11 times [OR 11.4 (3.6–36.2)] and 3 times [OR 3.3 (1.1–9.7)] higher among overweight and normal weight HIV individuals, respectively, when compared with the underweight individuals. 33 Signorini et al. had 27% increased risk of MS for every 1 kg/m2 increase in BMI [OR 1.27 (1.2–1.4)]. 23 Similarly, Alencastro et al. had increased risk ratio among overweight and obese HIV individuals. Overweight and obese men had risk ratio of 3.55 (2.59–4.87) and 6.28 (4.34–9.09), respectively. On the other hand, overweight and obese women had risk ratio of 3.2 (2.20–4.64) and 4.77 (3.30–6.89), respectively. 22
Four studies found significant association between MS and age. 22,26,33,38 Tesfaye et al. reported that odds of developing MS was six times [OR 6.3 (1.8–21.9)] and three times [OR 3 (1.1–8.5)] higher among HIV individuals who were above 45 years and between 25 and 34 years, respectively, compared with those who were less than 25 years of age. 33 Jantarapakde et al. found that HAART-naive individuals who were 35 years and above had four times [OR 4.2 (1.6–11)] risk to develop MS than those who were younger. 38 Similarly, Villamar et al. showed HIV individuals above 30 years had three times odds of developing MS [OR 3.16 (1.15–8.7)] than the younger HIV individuals. 26 Alencastro et al. had increased risk ratio among HIV individuals who were between 30–49 and 50–78 years. HIV men who were between 30–49 and 50–78 years had risk ratio (RR) of RR 2.04 (1.37–3.03) and 3.82 (2.45–5.96), respectively. HIV women who were between 30–49 and 50–78 years had risk ratio of 3.2 (2.20–4.64) and 2.51 (1.76–3.58), respectively. 22
The association between MS and gender was reported in four studies. 32 –34,38 Awotedu et al. reported that odds of developing MS was 11 times higher among the male individuals [OR 11 (3–48)] than the female individuals. 34 Similarly, Tesfaye et al. found that female individuals were almost three times more likely to develop MS compared with male individuals [OR 2.9 (1.4–5.7)]. 33 Likewise, Berhane et al. and Jantarapakde et al. reported similar odds among female individuals, respectively, [OR 2.3 (1–5.27)] 32 and [OR 1.7 (1–2.8)]. 38
Discussion
MS prevalence in developing countries has increased rapidly mainly due to lifestyle changes, driven by industrialization. 39 Reports from developing countries estimate the prevalence of MS in the general population to be varied, ranging from 9.8% to 86%. In Asia, the MS prevalence in the general population was 32.6%, 43.4%, and 19.2% in Thailand, Malaysia, and India, respectively. 40 –42 In the African regions, the MS prevalence ranged from 17.9% in Ethiopia to 86% in Nigeria. 43 –46 Studies from the South American countries reported the MS prevalence of 18.8% in Peru, 31.2% in Venezuela, 33% in Brazil, and 43.3% in Puerto Rico. 47 In comparison to the developing countries, developed countries such as Portugal, Norway, and United States reported similar or lower prevalence at 27.5%, 29.6%, and 34%, respectively. 48 –50 The high prevalence of MS in the general population has also extended to the HIV population. 9,11,12,51 The impact of MS in the HIV population has yet to be fully explored, especially across the developing countries, where the prevalence of HIV infection is higher, as compared with the developed countries.
The high prevalence of MS among PLWH in Africa, South America, and Asia regions may reflect the high prevalence of MS in the general population of the respective regions. The high prevalence may indicate the possibility of a cohort effect in these regions; which over past few decades have undergone rapid shifts in population structures from rural to urban areas, as well as socioeconomic changes. This may also explain why the prevalence of MS in this review was similar to the prevalence of MS among PLWH in developed countries. Reports from developed countries such as Spain, United States, Italy, and Portugal reported MS prevalence from 15.8% to 52.2%. 10,11,52,53 The wider range of ethnicities across developing regions such as Asia may also contribute to the differences in the prevalence of MS. Therefore, further studies to assess its effects on MS and components are required.
This review highlights that the criteria used in the diagnosis of MS play a significant role in estimating the prevalence of MS. There was heterogeneity in the criteria used within the developing regions. Alencastro et al. from Brazil compared three definitions of MS and found the prevalence was 17.2% (NCEP-ATP III 2001), 24.7% (ATP III/AHA/NHLBI 2005), and 22.1% (IDF 2005). 22 The differences in prevalence were also reported by three studies from Africa 29,33,34 and one study from South America. 26 All of the studies, except the South American study, reported a higher prevalence of MS using the ATP III/AHA/NHLBI 2005 definition as compared with the IDF 2005 definition. These variations were mainly due to the different cut offs used to diagnose abdominal obesity. In comparison to NCEP-ATP III 2001 criteria, the IDF 2005, ATP III/AHA/NHLBI 2005, and HARMONIZED 2009 used lower cut-off measurements of waist circumference, which were ethnic-specific as seen in studies conducted from India 36 and Thailand 38 and certain studies from Africa 28,29,31,33 –35 and South America. 22,26 Furthermore, the presence of abdominal obesity is a prerequisite for the diagnosis of MS using the IDF guidelines. Hence, direct comparison of MS prevalence among the different regions could not be made in this review, which suggests the importance of unifying of its measurement within this population in the various regions.
The overall mean prevalence of the individual components of MS among PLWH in this review were highest for low HDL cholesterol (50.1%), followed by hypertriglyceridemia (45.7%), hypertension (32.3%), abdominal obesity (23%), and hyperglycemia (22.5%). The high prevalence of dyslipidemia in this review was in agreement with eight studies among PLWH in developed countries. 12,51 –57 However, in these countries hypertriglyceridemia was observed more frequently than low HDL cholesterol. 51 –53,56,57 One study from Denmark reported hypertension as the most prevalent component of MS. 58
The pathophysiology of HIV-related dyslipidemia is not fully elucidated. Existing literature suggests an interplay of various factors, including immune activation of HIV infection per se, ART use, genetic predisposition, and environmental exposures such as dietary patterns, smoking, and lack of physical activity. 59 Before ART initiation, HIV infection results in an increase in triglycerides and substantial decrease in total cholesterol, HDL cholesterol, and LDL cholesterol. 60 If dyslipidemia was considered in isolation with regard to ART, we found that those who were HAART-naive had a higher prevalence of low HDL cholesterol. 24,30,33,34,38 Similarly, Bergersen et al. from Norway found higher prevalence of low HDL cholesterol among HAART-naive individuals (51.8%). 51 Although lipid disorders account for at least part of increased risk of CVD seen in this population, initiating HAART should not be delayed for fear of HIV-related dyslipidemia. It is important to note that HDL cholesterol possesses anti-inflammatory and antithrombotic properties 61 and, hence, the initiation of HAART may increase HDL cholesterol levels and reduce the events of CVD to some degree. Besides that, the presence of low HDL cholesterol was found to be independently associated with insulin resistance (IR), an established risk factor for CVD and DM in the general population. 34
Abdominal obesity was more prevalent in the non-HIV-infected population compared with the HIV population in both the developing and developed countries. 9,12,30,34,51 This may only be partially explained by the higher BMI among the non-HIV individuals who were reflecting better nutrition status in the general population compared with those who were HIV infected. 51 In this review, abdominal obesity was found to be higher in those who were on HAART compared with HAART naive. 30,31,34 However, reports from developed countries have been inconsistent, reporting either higher, 51 or almost similar, 9 prevalence of abdominal obesity among HAART and HAART-naive individuals.
Hyperglycemia plays a pivotal role in the development of CVD and DM. In this review, hyperglycemia appeared to be either higher 30 or almost similar 34 in the HIV population than the non-HIV population. The prevalence of this component among HAART individuals were either similar 34 or higher 24 than HAART-naive individuals. The pathophysiology of hyperglycemia in the HIV population is multifactorial, which include traditional risk factors such as genetic predisposition, physical activity, dietary intake, and obesity. 62,63 Additionally, the HIV virus itself have been implicated, as shown in in vitro studies, where the HIV-1 accessory protein viral protein R (Vpr) contributes to the development of IR and lipodystrophy among PLWH by suppressing the peroxisome proliferator-activating receptor-γ, a key regulator of adipocyte differentiation and tissue insulin sensitivity. 64 The use of antiretroviral drugs and HIV infection has been implicated in the development of hyperglycemia and MS. 63 In this review, only one study from Africa found that NRTI was associated with IR. 34
The traditional risk factors associated with MS among PLWH were examined. As in the non-HIV population, 49 advancing age was found to be associated with higher prevalence of MS among PLWH in our study. 22,23,30,32,33,38 This may reflect the increase in longevity of the population in response to better socioeconomic development in the developing regions. One study showed that the risk for MS was six times higher in those who were above 45 years old and a three times higher risk in those between 25 and 34 years of age. 33 Similarly, advancing age has been associated with increased prevalence of MS in developed countries. 9,65 Phenotypically, PLWH are ageing faster than those without HIV in that they are experiencing more age-related comorbidities at a younger age. 66 Bonfanti et al. from Italy did a comparison study between the HIV population with the non-HIV population and found the age-adjusted risk of having MS among HIV individuals was twice as great as that in the non-HIV individuals. 9 Our review demonstrates the lack of similar studies in developing countries and the need to explore this trend in these regions.
HIV-related factors such as higher CD4 count and lower viral load (VL) have been associated with increased risk for MS. 22,23,26,27 Only one study found association between CD4 count and risk for MS in this review. 23 Studies from developed countries however, reported varying results. 10,11,56,67 –69 Mondy et al. from the United States found high CD4 count as an independent predictor for the development of MS. The rise in CD4 count in this study was accompanied by increase in weight, improved nutritional and immunological status. These findings could be a reflection of physiological changes that accompany immune reconstitution. 10 However, other studies from the United States and Italy reported higher risk for MS in those with lower CD4 count and higher VL. Bonfanti et al. from Italy found that those with advanced HIV disease (VL >100,000 copies/mL and CD4 < 100 cells/mm3) were almost three times more likely to have MS [OR = 2.5 (1.1–6.5)]. 69 Squillace et al. from the United States found that HIV patients on HAART with detectable VL, ≥400 copies/mL, had significantly higher prevalence of MS than patients on HAART with undetectable VL, <400 copies/mL (32.2% vs. 22.7%), suggesting that HIV infection per se may contribute to the development of MS. 68
Not all studies included in this review made a comparison between those on HAART and HAART-naive. MS was found to be higher among those treated with HAART. 21,24,33,34 The use of HAART is a double-edged sword in HIV treatment. The higher CD4 count and lower VL among PLWH with MS represented the health return of the patients promoted by HAART. 10 However, the restoration of health is clouded by HAART-related metabolic consequences of a longer duration of therapy and type of HAART. A major potential difference in MS incidence between the resource-rich and resource-limited world is the inclusion of specific drugs within the two main offending classes; the PIs mainly ritonavir (either alone or in PI-boosted regimens) 18 and the older NRTIs, which include stavudine, didanosine, and lamivudine. 10,12,32,65 Furthermore, these classes, have been implicated in HIV/HAART-linked CVD. 18 The non-nucleoside reverse transcriptase inhibitors (NNRTIs) specifically efavirenz has been associated with increased risk for MS in one study in our review. 32 Interestingly, Sobieszczyk et al. from the United States found that nevirapine was protective against MS. 12
In addition to HAART, large cohort studies have shown that HIV individuals who smoke have substantially higher mortality from CVD and non-AIDS-related malignancies than the nonsmokers. 70,71 In the non-HIV population, tobacco use has been associated with increased risk of MS, mainly due to low HDL cholesterol, hypertriglyceridemia, and abnormalities in lipoprotein metabolism, hypertension, and hyperglycemia. 72 –74 The prevalence of smoking in the HIV population in this review ranged from as low as 2.7% in Ethiopia, 33 to as high as 94% in India. 21 Surprisingly, no significant association was found between smoking and the risk for MS. 22,25,26,28,33,38 This may be explained by the cross-sectional design and small study population of the studies in this review.
Limitation of review
The design of most the studies were cross-sectional in nature. This did not allow the possibility to determine the direction of association between the exposure factors and MS, and furthermore limited the interpretation of possible associated factors in this population. Lack of information on the antiretroviral drugs used in most of the study did not enable comparison between studies and the true effect of treatment on risk of MS in the HIV population. Most of the studies were carried out in South America and Africa. Hence, the results of this systematic review cannot be generalized. Nonetheless, this review can serve as a guide to region-specific studies that aim to examine MS among PLWH. Additionally, only English language articles were included in this review from six databases. Despite the limitations, this review has the advantage of using a systematic rather than a narrative approach to assess MS among PLWH in developing countries. To our knowledge, it is the first review to report on MS and the associated components in the HIV population in developing countries.
This review highlights the high prevalence of MS among PLWH and provides an essential overview on the current distribution of MS in the HIV population across the developing regions. Notably, this review revealed lack of MS and HIV research in developing countries. This review identified an important gap in the literature specifically from Asia, where the population is rapidly ageing and the HIV epidemic is second only to Africa. MS is a risk factor for CVD and DM, and the individual components of MS have also been associated with other comorbidities. Longitudinal studies would enable us to appreciate the true relationship between MS and its contributing factors among PLWH, both traditional and HIV-related risk factors. This review has important implications for clinical practice, in terms of early detection, prevention, and treatment of MS in the HIV population.
Footnotes
Acknowledgments
This study was funded by the University of Malaya High Impact Research Grant for the Malaysian Elderly Longitudinal Research group, MELOR (UM0000099/HIR.C3), Malaysia: HIV&Ageing group, MHIVA (H-20001-E000091), and the UMRG grant
Author Disclosure Statement
No competing financial interests exist.