
Abstract
It is unclear whether HIV-infected individuals remain at higher risk of invasive pneumococcal disease (IPD) compared with HIV-uninfected individuals. We conducted a cohort study of HIV-infected and demographically matched HIV-uninfected adults within Kaiser Permanente Northern California during the period 1996–2011. We used Poisson models to obtain rate ratios (RRs) for incident IPD associated with HIV infection and other risk factors. Among 13,079 HIV-infected and 137,643 HIV-uninfected adults, the IPD rate per 100,000 person-years was 160 (n = 109 events) for HIV-infected and 8 (n = 75 events) for HIV-uninfected subjects, with an adjusted RR of 13.0 [95% confidence interval (CI): 9.1–18.7]. For HIV-infected individuals, IPD incidence per 100,000 person-years decreased by 71% during study follow-up, from 305 in 1996–1999 to 88 in 2010–2011 (p < 0.001), with an adjusted RR of 6.6 (95% CI: 2.7–16.1) compared with HIV-uninfected subjects in 2010–2011. Risk factors for IPD among HIV-infected individuals included black compared with white race/ethnicity, smoking, cancer, and higher HIV RNA levels. The 23-valent pneumococcal polysaccharide vaccination was not associated with a reduced risk of IPD in HIV-infected or HIV-uninfected individuals. Among HIV-infected IPD cases, the most common serotype was 19A (33%), and 59% of serotypes were covered by the 13-valent pneumococcal conjugate vaccine (PCV13). Despite a dramatic decline in IPD incidence for HIV-infected adults since 1996, IPD rates were nearly sevenfold higher compared with HIV-uninfected adults in recent years, even after adjustment for risk factors. Timely antiretroviral therapy initiation, risk reduction strategies, and recent guidelines recommending PCV13 use may further reduce IPD incidence among HIV patients.
Introduction
I
Despite the observed decline in IPD rates among HIV-infected individuals, several studies have demonstrated a continued higher risk of IPD among HIV patients compared with the general population, even in recent years. 4,5,13 However, by relying on the general population as a comparison group, these studies have had limited ability to adjust for IPD risk factors that are likely to differ by HIV status, including lifestyle risk factors, comorbidities, and pneumococcal vaccine use. Thus, the continued higher risk of IPD among HIV patients may be explained, in part, by differences by HIV status in sociodemographic factors, such as access to care, 17,18 or by the higher prevalence among HIV patients of behavioral and clinical risk factors such as smoking, 19 coronary heart disease (CHD), 20 and cancer 21 that are associated with an increased risk of IPD. 4,22
The goal of this study was to assess trends in the incidence of IPD in a large cohort of HIV-infected and demographically similar HIV-uninfected adults from within the same healthcare system, accounting for differences by HIV status in key IPD risk factors. We examined IPD rates over 16 years of study follow-up and determined whether HIV-infected individuals remained at higher risk of IPD in recent years compared with HIV-uninfected individuals. We identified demographic characteristics, lifestyle risk factors, and comorbidities associated with the incidence of IPD among HIV-infected and HIV-uninfected individuals. Finally, for a subset of HIV-infected IPD cases, we described the distribution of S. pneumoniae serotypes to evaluate the potential impact of recent changes in vaccine guidelines.
Methods
Study design, setting, and population
We conducted a cohort study of HIV-infected and HIV-uninfected adults within Kaiser Permanente Northern California (KPNC), a large integrated healthcare system providing comprehensive medical care to 3.9 million members, with the KP membership mirroring the age, sex, and race/ethnicity distributions of the California population. 23 Members receive nearly all care at KPNC facilities, including immunizations, 24 which are provided conveniently and at no additional cost.
The study population was selected from a previously described cohort. 21 HIV-infected individuals were identified using the KPNC HIV registry, which includes all known HIV/AIDS cases since the early 1980s, with HIV status confirmed by review of medical charts or medical center case lists. Individuals not included in the HIV registry were considered HIV uninfected. HIV-uninfected members were frequency-matched 10:1 to HIV-infected individuals by age (5-year age groups), sex, medical center, and initial year of study follow-up. The start of follow-up (baseline) for HIV-infected adults was the earliest date on or after January 1, 1996, when they met the following criteria: KPNC member, ≥18 years of age, known to be HIV infected, and in HIV care, defined as the first CD4 count measurement recorded in the healthcare system. The start of follow-up for HIV-uninfected adults was the earliest date during the year selected in frequency matching when they met the following criteria: KPNC member and ≥18 years of age. Individuals were followed until the earliest of IPD, death, health plan disenrollment, or December 31, 2011.
The institutional review board at KPNC approved this study with a waiver of written informed consent.
Study measurements
The outcome of interest was incident IPD, defined as culture-positive S. pneumoniae from a normally sterile culture, including blood, cerebrospinal fluid, bone, or joint; in our study, almost all isolates were from blood. All microbiology testing at KP, including testing for IPD, is sent to a centralized laboratory in Berkeley, California, which has been certified according to Clinical Laboratory Improvement Amendment standards. We searched KPNC electronic health record (EHR) databases to identify the first occurrence of IPD for each patient.
Other data extracted from the EHR included laboratory test results (CD4 counts and HIV RNA levels); pharmacy prescription fills (ART and antihypertension medications); age; race/ethnicity (with imputed data where missing for 3% of HIV-infected and 31% of HIV-uninfected individuals 25,26 ); use of PPV23 vaccine; health plan enrollment periods; dates of death from hospital records, California death certificates, and Social Security Administration datasets; diabetes and cancer, as defined by inclusion in the KPNC diabetes 27 and cancer 28 registries; and inpatient or outpatient clinical diagnoses, including smoking/tobacco use [International Classification of Disease codes, version 9 (ICD-9): 305.1, V15, V65, 649, internal social history codes], hypertension (ICD-9: 401–405 or antihypertension medication use), CHD (ICD-9: 410–414), and stroke (ICD-9: 433–437). Data on S. pneumonia serotype were only available for 36% of cases, but there were no differences in age, sex, or race/ethnicity between those with and without serotyping data. Finally, we created a neighborhood socioeconomic status (SES) index based on 2000 US census measures of income, occupation, and education. 29
In addition to HIV status, the KPNC HIV registry was used to obtain data on race/ethnicity, HIV transmission risk factor, years of known HIV infection, nadir CD4 count recorded at KPNC, recent CD4 count and HIV RNA level, and ART use for HIV-infected individuals.
Statistical analysis
We conducted a time-dependent analysis. Time-fixed variables included sex, race/ethnicity (white, black, Hispanic, other/unknown), and SES (quintiles). Smoking was also treated as a fixed variable, defined as ever/never from 2 years before study entry through the end of study follow-up. The remaining analytical variables were time dependent, including current age (18–39, 40–49, 50–64, 65+ years); calendar era (1996–1999, 2000–2003, 2004–2007, 2008–2009, 2010–2011); prior receipt of the PPV23 vaccine (yes/no); and prior diabetes (yes/no), hypertension (yes/no), stroke (yes/no), CHD (yes/no), and cancer (yes/no). For HIV-infected individuals, additional time-dependent variables were recent CD4 count (<200, 200–499, ≥500 cells/μL), recent HIV RNA level (<500, 500–9999, ≥10,000 copies/mL), and prior ART use (yes/no).
We first compared baseline characteristics between HIV-infected and HIV-uninfected individuals using the Pearson chi-square test for categorical variables and the Kruskal–Wallis test for continuous variables. We calculated rates of IPD per 100,000 person-years, overall and stratified by calendar era of study follow-up, using Poisson models to assess trends over time. We then used Poisson models to estimate unadjusted and adjusted rate ratios (RRs) by HIV status, overall and within calendar eras. Adjusted RRs were obtained from models that included variables for age, sex, race/ethnicity, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use, with the overall model additionally including a variable for calendar era. We constructed multi-variable Poisson models for HIV-infected and HIV-uninfected individuals separately to identify factors associated with IPD, again evaluating age, sex, race/ethnicity, SES, calendar era, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use, and with the addition of recent CD4 count, recent HIV RNA level, and prior ART use for HIV-infected individuals. Finally, we used descriptive statistics to assess the distribution of S. pneumonia serotypes in a subset of HIV-infected IPD cases.
Analyses were performed with SAS 9.3 (Cary, NC). All statistical tests were two-sided, and statistical significance was defined as p < 0.05.
Results
The study population included 13,079 HIV-infected and 137,643 HIV-uninfected adults, contributing 67,936 and 898,112 person-years, and a mean of 5.2 and 6.5 person-years per person, respectively. The mean age was about 40 years for both HIV-infected and HIV-uninfected individuals, and about 90% of both groups were men (Table 1). The groups differed by race/ethnicity, and HIV-infected individuals had a slightly lower mean SES quintile. HIV-infected individuals more frequently had a history of smoking, cancer, and diabetes, whereas a history of hypertension, stroke, and CHD was similar by HIV status. A greater proportion of HIV-infected individuals compared with HIV-uninfected individuals received the PPV23 vaccine before baseline or during follow-up. Among HIV patients, the most common risk factor was men who have sex with men, and nearly half had antiretroviral experience before study entry.
CHD, coronary heart disease; PPV, pneumococcal polysaccharide vaccine; SD, standard deviation; SES, socioeconomic status.
There were 109 and 75 IPD events among HIV-infected and HIV-uninfected individuals during study follow-up, corresponding with incidence rates of 160 and 8 per 100,000 person-years, respectively. Compared with HIV-uninfected individuals, HIV-infected individuals had a 19-fold higher incidence of IPD during the period 1996–2011 [RR 19.2; 95% confidence interval (CI): 14.3–25.8, p < 0.001], with a 13-fold higher incidence after adjustment for age, sex, race/ethnicity, calendar era, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use (RR 13.0; 95% CI: 9.1–18.7, p < 0.001).
Crude IPD incidence rates for HIV-infected and HIV-uninfected individuals are shown by calendar era in Fig. 1, with unadjusted and adjusted RRs shown in Table 2. For HIV-uninfected individuals, crude IPD rates declined by 18% during study follow-up, with rates of 11 per 100,000 person-years in 1996–1999 and 9 per 100,000 person-years in 2010–2011, although this decrease was not statistically significant (p = 0.53). For HIV-infected individuals, IPD incidence per 100,000 person-years decreased by 71% during study follow-up, from 305 in 1996–1999 to 88 in 2010–2011 (p < 0.001). The unadjusted RRs comparing IPD incidence between HIV-infected and HIV-uninfected individuals decreased from 27.4 (95% CI: 16.2–46.1, p < 0.001) in 1996–1999 to 9.7 (95% CI: 4.1–23.1, p < 0.001) in 2010–2011. These estimates were attenuated after adjustment for age, sex, race/ethnicity, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use, yet a greater risk of IPD remained for HIV patients in all calendar eras, including in recent years, with an adjusted RR of 6.6 (95% CI: 2.7–16.1, p < 0.001) in 2010–2011.
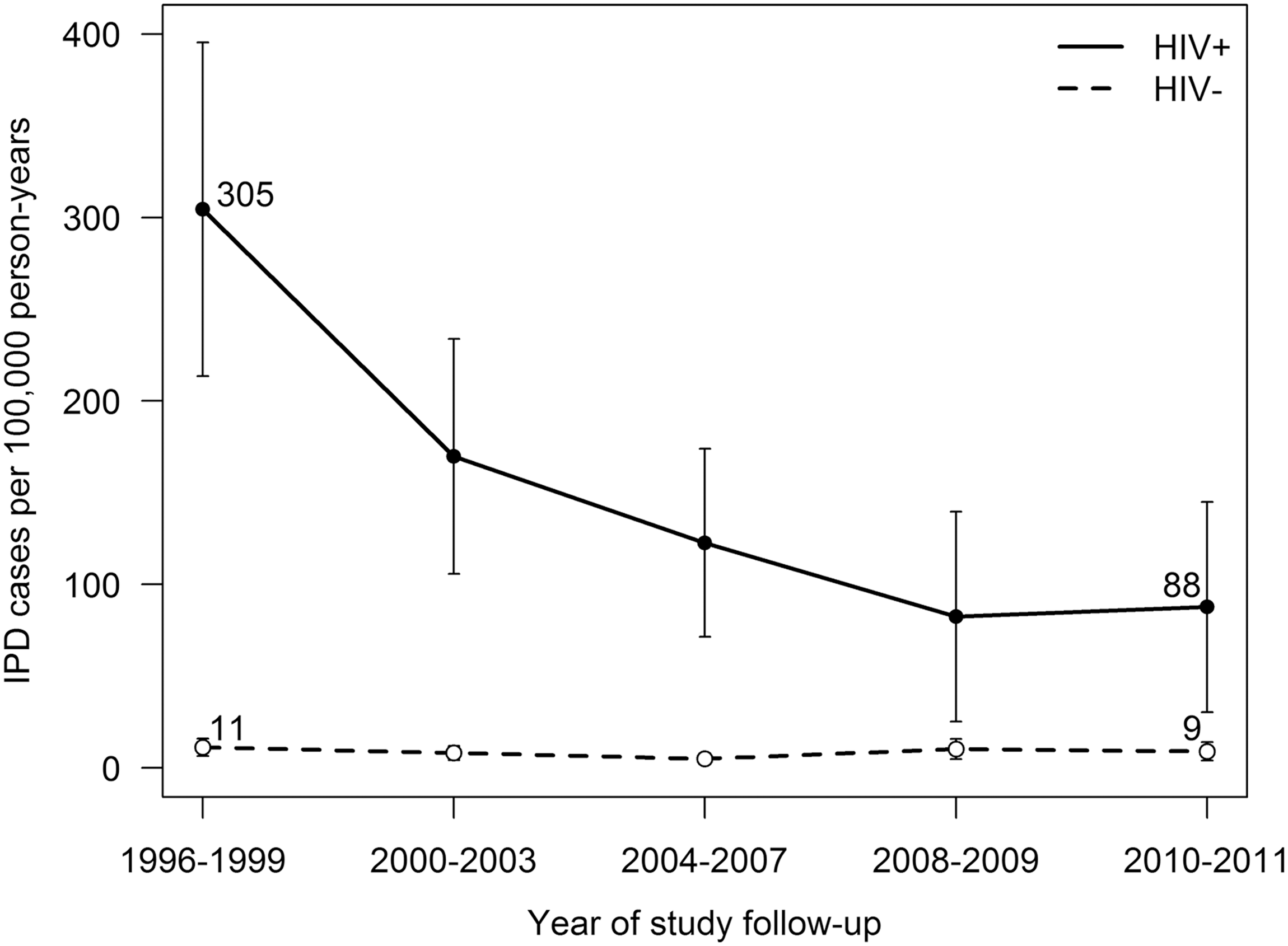
Unadjusted rates of IPD among HIV-infected and HIV-uninfected adults. Changes over time were statistically significant for HIV-infected (p < 0.001), but not HIV-uninfected, individuals (p = 0.53). IPD, invasive pneumococcal disease.
Adjusted RRs derived from Poisson models, including variables for age, sex, race/ethnicity, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use.
CHD, coronary heart disease; CI, confidence interval; IPD, invasive pneumococcal disease; PPV, pneumococcal polysaccharide vaccine; RR, rate ratio; SES, socioeconomic status.
Risk factors for IPD differed for HIV-infected and HIV-uninfected adults in multi-variable analysis (Table 3). For HIV-infected individuals, the incidence of IPD differed by race/ethnicity (p < 0.001), with higher risk among black individuals compared with white individuals (RR 2.3; 95% CI: 1.5–3.5). IPD incidence was also higher among individuals who were ever smokers (RR 2.3; 95% CI: 1.5–3.5, p < 0.001) and those with a history of cancer (RR 2.3; 95% CI: 1.3–4.0, p = 0.004). Several factors were protective against IPD, including lower HIV RNA levels compared with ≥10,000 copies/mL (p < 0.001) and a borderline association for higher SES quintiles compared with the lowest quintile (p = 0.057). IPD was not associated with age, sex, calendar era of study entry, diabetes, hypertension, stroke, CHD, PPV23 vaccination, recent CD4 count, or prior ART use among HIV-infected individuals.
Adjusted RRs obtained from Poisson models adjusting for age, sex, race/ethnicity, calendar era of study entry, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use, with the addition of recent CD4 count, recent HIV RNA level, and prior ART use for HIV-infected individuals.
ART, antiretroviral therapy; CHD, coronary heart disease; CI, confidence interval; IPD, invasive pneumococcal disease; PPV, pneumococcal polysaccharide vaccine; RR, rate ratio; SES, socioeconomic status.
For HIV-uninfected adults, the incidence of IPD was higher for females compared with males (RR 2.5; 95% CI: 1.4–4.6, p = 0.002), for individuals who were ever smokers (RR 2.9; 95% CI: 1.7–2.9, p < 0.001), for those with a history of stroke (RR 5.1; 95% CI: 1.6–17.0, p = 0.007), and for those with a history of cancer (RR 3.5; 95% CI: 1.7–7.4, p = 0.001). IPD incidence differed by calendar era of study entry (p = 0.021), with lower incidence in later calendar eras compared with 1996–1999. IPD was not associated with age, race/ethnicity, SES, diabetes, hypertension, CHD, or PPV23 vaccination among HIV-uninfected individuals.
Of the 39 HIV-infected IPD cases with S. pneumoniae serotyping data available, the most commonly isolated serotypes were 19A (n = 13; 33.3%), 9 N (n = 4; 10.3%), and 22F (n = 3; 7.7%); all are covered by PPV23, while only 19A is covered by PCV13. Overall, 31 (79.5%) HIV-infected IPD cases had serotypes covered by PPV23, 23 (59.0%) were covered by PCV13, 6 (15.4%) were covered by PCV7, and 7 (17.9%) were not covered by any of the vaccines.
Discussion
In this large cohort of HIV-infected and HIV-uninfected adults from within the same healthcare system, we observed a dramatic decline in IPD incidence rates for HIV patients since 1996, but with a continued higher risk compared with HIV-uninfected individuals even in recent years. We found that IPD incidence was nearly sevenfold higher among HIV-infected adults compared with HIV-uninfected adults in 2010–2011, independent of age, sex, race/ethnicity, SES, smoking, diabetes, hypertension, stroke, CHD, cancer, and PPV23 use. Risk factors for IPD differed by HIV status, with black race/ethnicity, smoking, cancer, and higher recent HIV RNA levels independently associated with a higher incidence of IPD among HIV-infected individuals, and female sex, smoking, stroke, and cancer associated with a higher incidence of IPD among HIV-uninfected individuals. PPV23 vaccination was not associated with a reduced incidence of IPD in HIV-infected or HIV-uninfected individuals, and the majority of HIV-infected IPD cases had S. pneumoniae serotypes that were covered by the PPV23 vaccine. Our results suggest that the observed decline in IPD incidence among HIV patients was attributable to improvements in viral suppression among HIV-infected individuals, rather than direct benefits from PPV23 vaccination.
The observed decline in IPD risk for HIV-infected individuals, but with a persistent disparity in recent years, is consistent with several previous studies that compared HIV patients with the general population. 4,5,13 In a study of HIV patients in Denmark, Harboe et al. found a declining risk of IPD during the period 1995–2012, but with a 20-fold higher risk compared with the general population in the latest decade. 4 Similarly, Heffernan et al. observed a dramatic decrease in IPD risk among AIDS patients in the United States during the period 1995–2000, but with a 35-fold higher risk remaining in 2000. 5 The decreasing risk of IPD over time for HIV patients in our study, although with a sevenfold higher incidence in 2010–2011, may have resulted from the inclusion of a healthier HIV patient population with equal access to care or from adjustment for IPD risk factors that are more prevalent among HIV patients. Indeed, we found that the association of HIV infection with IPD was attenuated after adjustment for smoking, cancer, and other risk factors. Our study suggests that confounding may explain some of the higher risk of IPD observed among HIV patients compared with the general population in prior studies, which had limited ability to adjust for individual-level risk factors such as smoking, cancer, and stroke.
Although we found an association of several traditional risk factors with IPD among HIV-infected individuals, HIV infection was associated with IPD even after adjustment for these factors. These results suggest that IPD risk in HIV-infected individuals is not fully attributable to a higher prevalence of IPD risk factors. Indeed, we found that higher recent HIV RNA was associated with a higher risk of IPD among HIV-infected individuals; we also observed a trend toward an association of lower recent CD4 count and IPD incidence, although this did not reach statistical significance. These results are consistent with prior studies finding that lower CD4 count and higher HIV RNA levels are associated with an increased risk of IPD among HIV patients. 3,4,12 Our results suggest that HIV disease severity explains some of the remaining difference in IPD risk by HIV status. Further, while we did not observe an independent association between prior ART use and IPD risk on an individual level, our results suggest that the observed population-level decline in IPD incidence may be attributable to the introduction of ART in 1996, which has been associated with substantial declines in opportunistic and other bacterial infections such as Pneumocystis carinii pneumonia. 16
Consistent with previous studies, 8 PPV23 vaccination was not significantly associated with a reduced risk of IPD among HIV-infected or HIV-uninfected individuals, with a high prevalence of PPV23-covered serotypes among HIV-infected IPD cases. Both HIV-uninfected and HIV-infected individuals may have benefited indirectly from PCV7 and PCV13 vaccination among children, licensed in 2000 and 2010, respectively. Although we did not observe a significant decline in IPD rates among HIV-uninfected individuals in our matched cohort since the licensing of PCV7 in 2000, as was observed in the general population, 30 PCV7 was used at KPNC beginning in 1996. Among HIV-infected individuals, Flannery et al. found that reductions in IPD were limited to serotypes included in the PCV7 vaccine for children, suggesting protection from herd immunity. 13 Of note, however, Heffernan et al. observed a significant decline in IPD risk among HIV patients subsequent to the introduction of ART and before the introduction of PCV7 among children, 5 lending support to the hypothesis that ART largely explains this trend. In our study, a substantial proportion of serotypes among HIV-infected individuals were covered by the PCV13 vaccine. These data, along with studies demonstrating better immunogenicity of PCVs compared with PPV23 for HIV-infected adults, 31 suggest that recent changes in vaccination guidelines 11 may further reduce IPD incidence in this population. A reduction in IPD incidence may also depend on efforts to increase pneumococcal vaccine coverage among HIV patients, a population with low overall vaccine use despite evidence of safety and effectiveness. 32,33
We identified several risk factors for IPD that were shared by HIV-infected and HIV-uninfected individuals, and others that were unique to each group. Smoking was a strong risk factor in both groups, consistent with prior studies among both HIV patients 4 and the general population. 34,35 Our study also confirmed previous studies finding that comorbidities, including cancer 22 and stroke, 36 were associated with a higher risk of IPD. Black race was a risk factor for IPD among HIV-infected individuals, but not HIV-uninfected individuals, reflecting previous studies among HIV patients, 3,5 but conflicting with studies finding that black race is associated with a higher risk of IPD in the general population. 22,34 Finally, female sex was associated with a higher risk of IPD among HIV-uninfected individuals, but not HIV-infected individuals, in contrast to prior studies that found male sex to be a risk factor in the general population. 34,37 Differences in risk factors across studies may be attributable to differences in the time periods included, the geographic areas examined, or the distribution of confounders in each study population. In addition to identifying subgroups of patients who may benefit from targeted pneumococcal vaccination, our data highlight the importance of the mitigation of modifiable risk factors, such as smoking cessation, 38 to reduce morbidity and mortality among HIV-infected patients.
There are several limitations to our study. First, because risk factors were collected from the EHR, there may have been some misclassification and we could not analyze these variables in detail. For example, smokers who were not asked about smoking behavior may have been misclassified as nonsmokers, and a variable that captured current smoking, rather than ever smoking, would likely have had an even stronger association with IPD. Second, there may be some risk factors for IPD that were not included in our analyses, such as splenectomy 39 and immune-mediated conditions other than HIV infection; 40 however, because these are rare, we expect their inclusion would have had minimal impact on our results. Third, while we may have overestimated the rate of IPD among HIV patients if they were more often tested for S. pneumoniae, IPD is a severe disease and would likely have been detected in most HIV-uninfected cases. Fourth, we only had serotyping data available for a subset of HIV-infected IPD cases; however, there were no demographic differences between cases with and without available serotyping data. Fifth, while many immunizations that are received outside of KPNC are back-entered into the EHR, some may not have been captured; however, a prior study found that KPNC data captured 89% of influenza vaccinations. 24 Finally, follow-up ended before the use of PCV13 among HIV-infected individuals, but our results can serve as a baseline for studies comparing IPD incidence by HIV status in more recent years.
Our study also has several strengths. First, to our knowledge, this is the largest study to directly compare trends in IPD incidence by HIV status. The KPNC EHR allowed for complete and accurate ascertainment of IPD, with serotyping data available for a subset of cases. Second, we used a well-characterized cohort of HIV-infected and matched HIV-uninfected individuals from the same healthcare system, thus allowing for adjustment of individual-level confounders and minimizing the selection biases that can be introduced by using an external comparison group. Further, because KPNC members have comprehensive medical insurance coverage, differences in IPD incidence by HIV status were unlikely to be attributable to differential access to care. Third, the KPNC HIV registry allowed for high-quality ascertainment of known HIV infection. Finally, the KPNC membership mirrors the age, sex, and race/ethnicity distributions of the surrounding Californian population, 23 and the demographics of HIV-infected members are comparable with those of reported AIDS cases in California. 41 Thus, our results are likely to be generalizable to the broader insured population.
In summary, despite decreasing incidence of IPD among HIV-infected individuals, we found a nearly sevenfold higher risk compared with HIV-uninfected individuals in recent years, even with comprehensive access to care and after adjustment for key risk factors. Given 2012 guidelines recommending PCV13, followed by PPV23 vaccination for HIV-infected individuals, 11 and 2014 guidelines recommending PCV7 vaccination for older adults in the general population, 42 future studies should examine more recent trends in IPD incidence and changes in the distribution of IPD serotypes by HIV status. Our results suggest that a continued emphasis on timely ART initiation and risk reduction strategies, as well as recent changes in pneumococcal vaccination guidelines, may further reduce the risk of IPD among HIV patients.
Footnotes
Acknowledgment
This research was supported by a research grant from Pfizer Pharmaceuticals.
Author Disclosure Statement
W.A.L. received research grant support from Pfizer. J.L.M. received research grant support from Merck. M.A.H., C.P.Q., M.J.S., and C.R.C. received research grant support from Pfizer and Merck. W.J.T. received research grant support from Pfizer, Merck, Gilead, Bristol-Myers Squibb, ViiV Healthcare, and Vertex. All other authors report no conflicts of interest.