
Abstract
We sought to examine the trends of cigarette smoking, identify correlates of smoking, and examine the impacts of smoking on health-related quality of life (HRQOL) among people living with HIV in Ontario, Canada. Study sample included 4473 individuals receiving care and enrolled in the Ontario HIV Treatment Network Cohort Study. Self-report data on cigarette smoking, HRQOL, and demographic and sociobehavioral variables were collected between 2008 and 2014 through annual face-to-face interviews. Clinical data were abstracted from participants' medical records and enhanced through linkage with a provincial public health laboratory database. Analyses included descriptive statistics, generalized logit regression, and linear mixed-effects modeling. At first interview, 1760 participants (39.3%) were current cigarette smokers. Smoking prevalence declined annually by 1.6% between 2008 and 2014, but remained much higher than the prevalence in the general population. Current cigarette smokers were more likely to be younger, male, white or indigenous, Canadian-born, single, unemployed with lower education, heavy drinkers, nonmedicinal drug users, and to have current depression than former cigarette smokers or those who never smoked. Current cigarette smokers also had significantly (p < 0.001) worse SF-12 physical component summary (β = −2.07) and SF-12 mental component summary (β = −1.08) scores than those who never smoked after adjusting for demographic, socioeconomic, and HIV-related clinical variables. To reduce the burden of cigarette smoking, cessation interventions that take into account the complex social, economic, and medical needs of people living with HIV are needed urgently.
Introduction
T
People living with HIV have complex socioeconomic and medical needs that may influence smoking behavior. For example, some groups of the population [e.g., men who have sex with men (MSM), indigenous people, racial and ethnic minorities, and those who are economically disadvantaged] that are disproportionately affected by the HIV epidemic also have higher prevalence of smoking than the general population. 15 –19 In addition, individuals with HIV experience higher burdens of mental health and substance use disorders than the general population. 20 –23 While substance use and depression are strongly correlated with cigarette smoking and increased nicotine dependence, 24,25 they are also linked with lower readiness and decreased motivation to quit smoking. 26,27 Therefore, it is critical to understand correlates of smoking behavior in this population to design tailored and successful smoking cessation interventions.
With improvement in survival due to the advance in antiretroviral therapy, 28,29 HRQOL has gained importance as a measure of the burden of HIV disease. Cigarette smoking is one of the major determinants of HRQOL in this population. It is associated with greater risk of cardiovascular disease, chronic obstructive pulmonary disease, and non-AIDS malignancy, thereby contributing to higher comorbid illnesses. 9,30 In addition to its indirect impact on HRQOL through comorbid illnesses, smoking is also directly associated with lower physical and mental HRQOL. 8,11 While some studies have examined the relationship between smoking cessation and changes in HRQOL, 31 to our knowledge, no study has examined the longitudinal association between smoking and HRQOL in people with HIV in Canada. A better understanding of the relationship between smoking and HRQOL will help inform new or existing medical, psychological, and HRQOL interventions that ultimately improve the health of people living with HIV.
In light of the research gaps discussed above, we undertook the current study to (1) examine trend of smoking and smoking cessation among people living with HIV; (2) identify demographic and socioeconomic factors independently associated with cigarette smoking; and (3) examine the adverse impact of cigarette smoking on HRQOL in people living with HIV. We addressed these objectives using data from one of the largest ongoing studies of people living with HIV in Canada, the Ontario HIV Treatment Network Cohort Study (OCS).
Methods
Study participants
Data were drawn from the OCS, an observational open dynamic cohort of people receiving HIV care in Ontario, Canada. Details of the cohort have been described previously. 32 Participants were recruited from 11 hospital-based specialty HIV clinics, hospital-based family practice units, and community-based primary care physician practices and broadly represent people receiving HIV care in Ontario. Eligibility criteria included the following: (1) 16 years of age or older; (2) diagnosis of HIV infection; (3) resident of Ontario; (4) able to speak English; and (5) able to provide informed consent. Clinical data were abstracted from participants' medical records and enhanced through linkage with databases at Public Health Ontario Laboratories, which conducts all serological and viral and bacteriological tests in the province. Demographic, psychosocial, behavioral, and HRQOL data were collected annually through face-to-face interviews using a standardized questionnaire. Participants were compensated $20 and $50 for completion of the core version (30 min) and the extended version (120-min) of the annual questionnaire, respectively. Informed consent was obtained from all participants, and the OCS was approved by the Ethics Review Boards of individual study sites and the University of Toronto. As of December 2014, 6671 individuals had enrolled in the OCS. For the present analysis, however, only 4563 people who completed at least one annual questionnaire between 2008 and 2014 are eligible.
Measures
Cigarette smoking
Self-reported data on cigarette smoking were collected using interviewer-administered questionnaires starting 2007. Participants were asked if they were current smokers (i.e., smoked in the past 30 days, occasionally or regularly), former smokers (i.e., smoked in the past, but not in the last 30 days), or never smoked.
Health-related quality of life
The standard version (4-week recall period) of the Medical Outcomes Study Short Form Survey (SF-12v2) was used to assess HRQOL. 33 The SF-12v2 is a generic health survey with 12 questions assessing eight domains of health: physical functioning, role functioning physical, bodily pain, general health, vitality, social functioning, role functioning emotional, and mental health. It has been validated with HIV-positive populations and was found to be suitable to monitor health status. 34 Two composite scores, physical component summary (PCS) and mental component summary (MCS), were computed following the developers' manual. 33 The PCS and MCS scores have a possible range of 0 to 100 with higher scores being indicative of better physical and mental health. The minimum clinically significant differences are two to three points for PCS score and three points for MCS score. 35
Demographic, substance use, and clinical characteristics
Demographic and socioeconomic data collected included the following: age, gender, sexual orientation, race and ethnicity, country of birth, education, employment status, personal income, and substance use history. We categorized sex (female vs. male, MSM vs. male-non-MSM), country of birth (Canada vs. other), and employment (employed part-time or full-time vs. other). We coded race into four categories (i.e., indigenous, African/black/Caribbean, Caucasian, and other), education into four major groups (i.e., less than high school, completion of high school, trade, college, or some university, and completion of university education). Data on annual personal income were collected in increments of $10,000 and coded into three categories (i.e., less than $20,000, $20,000–$49,999, and $50,000 or greater). The three-item Alcohol Use Disorder Identification Test—Consumption (AUDIT-C) questionnaire was administered to assess alcohol use in the past 12 months. 36 Participants were also asked whether they have used nonmedicinal drugs, excluding Marijuana, in the past 6 months. Nonmedicinal drugs were defined as any recreational drugs (except Marijuana) or prescription or over the counter drugs taken for nonmedical purposes. Depression and psychological distress symptoms were assessed using the 20-item Center for Epidemiological Studies (CES-D) scale or the 10-item Kessler Psychological Distress Scale (K10). 37,38 The presence of depression was determined using previously established cutoff points (≥22 for K10 and ≥23 for CES-D). 39,40
Data on date of HIV diagnosis, AIDS-defining illnesses, and recent CD4 T lymphocyte counts were extracted from medical charts and augmented with self-reported data. HIV viral load data were obtained from Public Health Ontario Laboratories, the sole provider of this testing in the province of Ontario, and were supplemented (where data were missing) with chart abstraction and self-report.
Statistical analyses
All statistical analyses were performed using SAS software (SAS Institute Inc, version 9.3). Of the 4563 participants who completed at least one questionnaire during the study period (2008–2014), we excluded 90 (2%) participants from all analyses due to missing data on smoking (n = 1), HRQOL (n = 40), or confounder variables (n = 49). The final sample consisted 4473 individuals with a median of four questionnaires [interquartile range (IQR): 2 to 5] and a total of 15,908 person-years of observations (median follow-up time: 3.5 years. IQR: 1.1 to 5.1).
We calculated prevalence of smoking as the number of current smokers divided by the total number of people interviewed for each year. Confidence intervals (CIs) for proportions of smokers were estimated using a simple binomial distribution. The trend of smoking prevalence over time was assessed using Generalized Estimating Equations methods with an exchangeable correlation matrix to account for repeated measures per subject.
Characteristics of the sample by cigarette smoking status at first interview were summarized using descriptive statistics (i.e., median and IQR for continuous variables and frequencies and percentages for categorical variables). We compared characteristics of current smokers with former smokers and people who had never smoked using chi-square tests for categorical variables and Kruskal–Wallis one-way ANOVA test for continuous variables. We used multivariable generalized logit regression models to identify correlates of current or past smoking, compared to those who never smoked.
We used linear mixed-effects modeling to examine the association between cigarette smoking and physical and mental HRQOL with people who had never smoked as the referent group. The simplest form of mixed-effects modeling with random intercepts was used to allow variation across individuals in baseline values of PCS and MCS. Cigarette smoking status was treated as a time-varying variable and models were adjusted for time since first interview and study site. Confounder variables were selected for multivariable analyses based on prior knowledge and by examining differences in effect sizes between unadjusted and adjusted estimates (a change of 10% or greater). When two or more variables measured similar concepts or were highly correlated (e.g., employment and income), we retained the variable that showed the strongest association with the outcome variable. Continuous variables were mean-centered before they were entered into the regression models.
Finally, we conducted subanalyses among participants with two or more follow-up interviews (n = 2874; 13,631 person-years) to examine smoking cessation and initiation rates. We defined sustained cessation as being a current smoker at first interview and reporting being a former smoker on all follow-up interviews. Initiation or re-initiation of smoking was defined as having reporting being a former smoker or never smoker at first interview and be a current smoker in all follow-up interviews.
Results
The study sample comprised predominantly white male adults with higher level of education and lower income and who were on antiretroviral treatment with undetectable HIV viral load (Table 1).
Kruskal–Wallis one-way ANOVA test for continuous variables and chi-square test for categorical variables.
Data missing for 113 individuals.
p < 0.05, current smoker versus former smoker.
p < 0.05, current smoker versus nonsmoker.
IQR, interquartile range.
Boldface indicates statistical significance (p < 0.05).
Prevalence and trends of cigarette smoking
At first interview, 1760 individuals (39.3%; 95% CI: 37.9–40.8%) were current smokers, 1044 individuals (23.3%; 95% CI: 22.0–24.4%) were former smokers, and 1669 individuals (37.3%; 95% CI: 36.0–38.9%) had never smoked. Among current smokers, 783 (44.5%; 95% CI: 42.1–46.7%) were light smokers (≤10 cigarettes/day), 604 (34.3%; 95% CI: 32.3–36.8%) were moderate smokers (11–20 cigarettes/day), and 373 (21.2%; 95% CI: 19.2–22.9%) were heavy smokers (>20 cigarettes/day). For current smokers, the median duration of smoking was 26 years (IQR: 18–33).
Smoking prevalence declined from 39.3% (95% CI: 36.8–41.5%) to 32.7% (95% CI: 30.8–34.6%) between 2008 and 2014 with a mean annualized rate of decline of 2.96% (95% CI: 2.23–3.67%) (Fig. 1). The mean annualized rate was 1.58% (95% CI: 0.79–2.36%) after adjusting for age, sex, race, and study site, suggesting that the decline in smoking prevalence in the sample was partially due to the change in the demographic characteristics of the sample. To assess the potential effect of loss to follow-up on the trend of prevalence, we repeated the analyses in a subset of participants who completed four or more questionnaires (n = 2284; 11,861 person-years). Although the overall prevalence of smoking was slightly lower in this subgroup, it declined from 35.8% to 31.0% with a mean unadjusted annualized rate of decline of 3.14% (95% CI: 2.29–3.98%) and an adjusted annualized rate of 1.24% (95% CI: 0.27–2.22%).
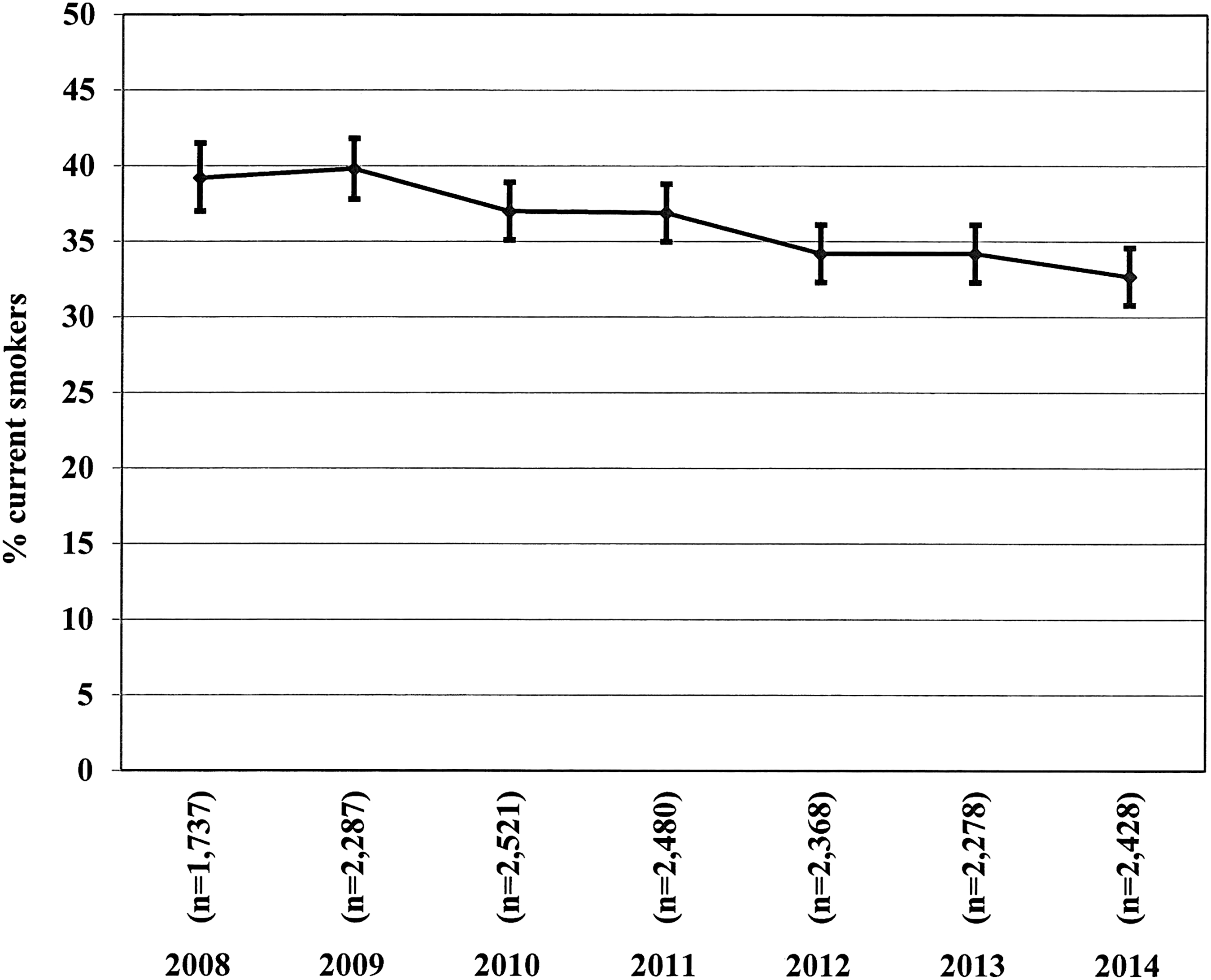
Annual cigarette smoking prevalence among OCS participants, 2008–2014.
In subanalyses among 1092 persons who were current smokers at first interview and completed two or more follow-up interviews, 56 (5.1%) reported sustained cessation (i.e., reported being a former smoker on all follow-up interviews) and 266 (24.4%) reported intermittent cessation (i.e., reported being a former smoker on at least one follow-up interview). On the contrary, among 1782 individuals who were former smokers or had never smoked at first interview and completed two or more follow-up interviews, only 40 (2.2%) (6 who never smoked and 34 former smokers) reported sustained initiation of cigarette smoking (i.e., reported being a current smoker on all follow-up interviews) and 121 (6.8%) reported intermittent smoking.
Correlates of cigarette smoking
At first interview, demographic, behavioral, and clinical characteristics of current smokers differed significantly from those who never smoked cigarettes (Table 1). Compared to those who had never smoked, current smokers were more likely to be male; Caucasian or indigenous; single, divorced, or widowed; born in Canada; less educated; unemployed; current drug users; frequent heavy drinkers; have depression or anxiety. They were, however, less likely to be on antiretroviral treatment and more likely to have low CD4 cell counts and detectable plasma HIV viral load than those who never smoked cigarettes.
Similar to current smokers, former smokers were more likely than those who had never smoked to be older; male; gay, lesbian, or bisexual; Caucasian; and Canadian-born. They reported higher prevalence of drug use and heavy drinking. They have also been infected with HIV for a longer period of time. In terms of education and income, there were no significant differences between former smokers and people who had never smoked.
In multivariable generalized logit regression analysis (Table 2), current smokers were more likely to be younger, male (MSM or non-MSM), single, born in Canada, less educated, unemployed or retired, current drug user, heavy drinker, and to have major depressive disorder. They were also more likely to be indigenous, but less likely to identify themselves as African, Caribbean, or black. Results from the multivariable regression model also indicate that, compared to those who never smoked, former smokers were more likely to be indigenous, non-MSM male, born in Canada, less educated, unemployed or retired, and heavy drinker. Unlike current smokers, they were more likely to be older and married or in a committed relationship than those who never smoked cigarettes.
Results are from multinomial logit regression model and adjusted for study site. The reference category is “nonsmoker”
AOR, adjusted odds ratio; CI, confidence interval; OCS, Ontario HIV Treatment Network Cohort Study.
Boldface indicates statistical significance (p < 0.05).
Cigarette smoking and HRQOL
In bivariable linear mixed-effects models (Table 3), PCS scores were lower for current smokers (β = −3.34, p < 0.001) and former smokers (β = −2.31, p < 0.001) than people who never smoked. Current smokers also had significantly lower MCS scores (β = −2.25, p < 0.001) than people who never smoked. The difference between current smokers and former smokers on MCS scores, however, did not reach statistical significance (β = −0.18, p = 0.986).
n = 4473 participants and 15,908 person-years. Results presented are (regression coefficient and p-value) from linear mixed-effects regression models. Multivariable regression models are further adjusted for study site and time since first interview in addition to the variables shown.
MCS, mental component summary; PCS, physical component summary.
Boldface indicates statistical significance (p < 0.05).
Results from multivariable mixed-effects models for PCS indicated that the negative effect of smoking remained significant after adjusting for age, sex, race, immigration status, education, employment, frequency of heavy alcohol use, drug use, and clinical variables, including antiretroviral treatment, duration of HIV infection, CD4 counts, and HIV viral load. Although the strengths of associations between smoking and PCS score were reduced from that of the bivariable model, the effect size for current smokers (β = −2.07, p < 0.001) remained greater than the minimally important difference. The association between smoking and MCS score was also weaker in the multivariate mixed-effects models. Current smoking remained significantly associated with lower MCS scores (β = −1.08, p < 0.001) although the effect size was lower than the minimally important difference of three points.
In a subsample of participants who were current smokers at first interview and completed two or more follow-up visits (n = 1092; 5091 person-years), those who quit intermittently or achieved sustained cessation had a higher PCS score than those who remained smokers in bivariable (β = 2.20, p < 0.001) as well as multivariable (β = 1.28, p = 0.021) mixed-effects models, suggesting some benefit of smoking cessation with respect to physical HRQOL. The difference in MCS score between those who quit intermittently or successfully versus those who remained smokers, however, was marginal in both bivariable (β = 0.70, p = 0.266) and multivariable (β = 0.04, p = 0.944) mixed-effects models.
Discussion
We examined the trend of smoking among HIV-positive people in Ontario, Canada, and found that nearly four in ten participants (39.2%) were current smokers at first interview, a rate that is three times higher than the 13% prevalence in the general population. 41 While this is consistent with estimates from some studies (36–42%), 4,42,43 it is lower than prevalence estimates reported by others (49–75%). 44 –46 The prevalence of smoking decreased from 39.0% in 2008 to 32.8% in 2014 with a mean adjusted annual decline rate of 1.58%. Similar declining trends were also observed in the Multicenter AIDS Cohort Study (from 53.9% to 36.9% between 2002 and 2012) and in the Swiss HIV Cohort Study (from 60% to 44% between 2000 and 2009). 45,46
We also examined demographic, socioeconomic, substance use, and mental health factors associated with cigarette smoking. Consistent with other studies, 4,42 current smokers were more likely to be younger than former smokers or those who never smoked. While men in general were significantly more likely to be current smokers than women, heterosexual men had higher odds of being current smokers than MSM. The higher prevalence of smoking observed in men relative to women is in agreement with evidence from the general population as well as in people living with HIV. 23,42 A significant association between ethnicity and smoking status was also observed with increased odds of being a current smoker in indigenous persons, but decreased odds of being a current smoker among participants from African, Caribbean, or black ethnic groups. This pattern mirrors data from the general population showing smoking rates of 32.3%, 19.5%, and 7.6% for Aboriginal, Caucasian, and black Canadians, respectively. 47 As reported elsewhere, 42 we found an association between smoking and marital/relationship status, with higher odds of smoking among participants who were single, divorced, or widowed than those who were married or in a committed relationship. In line with the literature, 4,25,45,48 lower level of education and unemployment were associated with higher odds of smoking in the current study.
We also identified a syndemic of cigarette smoking, alcohol use, and nonmedicinal drug use in our sample. Prevalence of smoking was significantly higher among heavy drinkers than nondrinkers. In addition, greater frequency of heavy drinking was associated with increasing rates of smoking among heavy drinkers. Participants who reported nonmedicinal drug use were also twice more likely to be current smokers than those who did not use nonmedicinal drugs. The co-occurrence of drug and alcohol use disorders among HIV-positive smokers has been documented previously. 25,42,43,45,48 The intersecting epidemics of smoking and heavy drinking are concerning as smoking increases the craving for alcohol and alcohol consumption augments the pleasure from smoking. 49 Illicit drug use can also play an important role in the relationship between smoking and alcohol consumption as previous research has shown that illicit drug use is associated with lower levels of interest and readiness to quit smoking. 26
Consistent with previous research, 4,43,45,50 we also found a substantial burden of depression among current smokers compared with former smokers or those who never smoked. This is a great concern as depression and smoking may affect each other reciprocally. Among current smokers, for example, depression has been associated with higher nicotine dependence and lower readiness to quit. 26,51 Among smokers who attempt to quit, those with a history of depression are more likely to experience severe withdrawal symptoms than those without depression. 52 On the contrary, long-term use of nicotine can produce low levels of serotonin that might trigger or worsen depression. 53,54 The progression of depressive symptoms over the course of smoking cessation may, in turn, decrease the chances of successful quitting. For instance, a study that examined readiness to quit among HIV-positive smokers found that depression, stress, and anxiety were reported frequently as causes of relapse among those who attempted to quit. 55
Further, we found a statistically and clinically significant association between current cigarette smoking and lower physical and mental HRQOL after adjusting for age, gender, race, marital status, education, employment, alcohol use, illicit drug use, CD4 cell counts, HIV viral load, and antiretroviral treatment status. We also found a statistically significant association between intermittent or sustained cessation and higher physical HRQOL. Our findings are consistent with previous cross-sectional studies that reported relationship between smoking and decreased PCS and MCS scores as well as lower scores in general health perception, physical functioning, bodily pain, energy, role functioning, and cognitive domains. 2,8,11 Lower HRQOL can be a direct consequence of smoking cigarettes, given that substances inhaled in cigarettes have been linked with muscular weakness, vitality loss, and psychological disturbances. 56 It is also plausible that low HRQOL among smokers may be due to indirect consequences of comorbid illnesses, including lung diseases, ulcers, cancers, and cardiovascular disease, associated with smoking. 57,58
A major strength of our study is the longitudinal data from a large and diverse sample that broadly represents people in HIV care in Ontario, Canada. However, findings of this study should be interpreted in the context of several limitations. First, our data on smoking are self-reported and not corroborated with objective measures such as cotinine concentration or exhaled carbon monoxide levels. Hence, our estimates of smoking prevalence may be lower than the true prevalence as previous studies have shown that self-report can underestimate smoking prevalence. 59,60 Second, attrition may have contributed to the declining smoking prevalence observed in our sample as those who were lost to follow-up had a higher smoking rate at first interview compared to those with repeated interviews. Third, although our analyses adjusted for several confounders, we cannot rule out residual confounding due to unmeasured variables or measurement errors on confounder variables. Finally, our results may not be generalizable to individuals who do not participate in the OCS. Although OCS participants represent the patient population receiving HIV care in Ontario, individuals who do not participate in OCS are younger and less likely to be male, Caucasian, and Canadian-born than those who are enrolled in the cohort. 22,32
Despite these limitations, our findings corroborate the fact that the prevalence of smoking among people living with HIV remains substantially higher than in the general population. Further, we have demonstrated that smoking is independently associated with poor physical and mental HRQOL in people receiving HIV care after adjusting for demographic, substance use, and clinical variables. This is the first study, to our knowledge, to validate the link between smoking and HRQOL using a large sample with repeated measurements in people living with HIV. As such, it adds to the growing evidence indicating the need for smoking cessation interventions in this population.
Given the persistent high prevalence of smoking in people with HIV, there is an urgent need for smoking cessation interventions. Smoking cessation interventions can result in significant improvement in HRQOL and reduction in mortality rate. 30,31 Although as many as three out of four smokers with HIV are interested in smoking cessation, only one in four quit successfully. 61,62 The risk factors associated with smoking in people with HIV are similar to those observed in the general population, but people with HIV are more likely to have several of these risk factors. 63 For example, co-occurring mental health, drug use, and alcohol use disorders are two to five times higher among people living with HIV than the general population. 64 –68 These risk factors interact to reinforce cigarette smoking behavior and act as barriers to successful implementation of smoking cessation interventions. 69,70 Hence, a successful smoking cessation intervention requires a comprehensive approach that addresses co-occurring mental health, alcohol, and drug use disorders. In this respect, novel strategies such as the use of electronic and mobile health technologies (e.g., cell phone apps) can play a key role in making smoking cessation and mental health interventions more accessible. 71
Footnotes
Acknowledgments
We gratefully acknowledge all the people living with HIV who volunteered to participate in the OHTN Cohort Study and the work and support of the OCS Governance Committee and Scientific Steering Committee members: Adrian Betts, Anita C. Benoit, Breklyn Bertozzi, Les Bowman, Lisungu Chieza, Tracey Conway, Patrick Cupido, Brian Huskins, Joanne Lindsay, Mark McCallum, John McTavish, Colleen Price, Rosie Thein, Barry Adam, David Brennan, Claire Kendall, Tony Antoniou, Ann Burchell, Curtis Cooper, Trevor Hart, Mona Lofty, Kelly O'Brien, Janet Raboud, and Anita Rachlis. The OHTN Cohort study also acknowledges the work of past Governance Committee and Scientific Steering Committee members. We thank all interviewers, data collectors, research associates, coordinators, nurses, and physicians who provided support for data collection. The authors wish to thank OCS staff for data management, IT support, and study coordination: Madison Kopansky-Giles, Jason Globerman, Beth Rachlis, Robert Hudder, Gokul Kalaimani, Lucia Light, Veronika Moravan, and Nahid Qureshi. We also acknowledge the Public Health Laboratories, Public Health Ontario, for supporting linkage with the HIV viral load database. The OHTN Cohort Study is funded by the AIDS Bureau of the Ontario Ministry of Health and Long-Term Care. The opinions, results, and conclusions are those of the authors and no endorsement by the Ontario HIV Treatment Network or Public Health Ontario is intended or should be inferred.
Author Disclosure Statement
J.R. acknowledges a Chair in Biostatistics award from the OHTN.