
Abstract
Long-term use of antiretroviral therapy (ART) increases the risk of developing lipodystrophy. Few studies from Africa have used longitudinal data to assess the development of lipoatrophy and lipohypertrophy. We use clinical anthropometry and dual-energy X-ray absorptiometry (DEXA) to describe changes in body fat distribution over a 24-month period in individuals initiated on ART. A convenience sample of black South Africans (55 men and 132 women) were recruited and followed for 24 months after commencing ART. Body fat distribution was assessed using anthropometric measurements and DEXA scans at baseline and then at 3, 6, 12, 18, and 24 months after commencing ART. DEXA was also used to estimate abdominal visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT). Women gained more overall weight and more regional fat in all areas analyzed on DEXA scans. Women, not men, experienced a significant increasing trend in trunk fat and a significant decreasing trend in limb fat, when expressed as a percentage of total body fat. In men, the risk of developing lipoatrophy was more than two times greater than that of women, after adjusting for age, baseline body mass index, and ART regimen. Lipohypertrophy occurred similarly in men and women. VAT and SAT increased significantly in men and women, with women gaining considerably more than men. These findings are of great concern as an increased waist circumference is associated with increased mortality in HIV-infected populations. Further investigation is required to understand the mechanisms underlying the sex differences in changes in body fat distribution and its effects on cardiovascular risk.
Introduction
S
Subjective methods, such as patient report, 4,7,8 and objective methods, such as dual-energy X-ray absorptiometry (DEXA), 9,10 computerized tomography (CT), and magnetic resonance imaging, have been used to detect lipoatrophy and lipohypertrophy. 2 However, few studies from Africa have distinguished between lipoatrophy and lipohypertrophy, 3,4,11 and none have used changes in DEXA measures. Longitudinal studies using DEXA measures to define lipoatrophy and lipohypertrophy have frequently been done in high-income countries 10,12 and have shown that lipoatrophy occurs more frequently in patients using a stavudine-based ART regimen. However, subjects in these studies were mostly middle-age white men, demographically different to the majority of patients receiving ART in sub-Saharan Africa.
The aim of our study was to use DEXA scans to describe the changes in fat distribution over a 24-month period in a population of black South African men and women initiated on ART and to investigate the factors associated with these changes.
Methods
Participants
A convenience sample of HIV-infected men and women presenting at Crossroads Community Health Centre in Cape Town was enrolled in a 24-month longitudinal study. A sample size calculation based on a population of 500, 5% margin for error, and 95% confidence interval, indicated that a sample size of 184 participants was needed. ART initiation occurred after enrollment into the study and completion of baseline evaluations. During the course of the study, there was a change in the nucleoside reverse transcriptase inhibitors (NRTIs) used in first-line ART regimens in South Africa, from stavudine or zidovudine to tenofovir, together with lamivudine, and efavirenz or nevirapine. The second-line regimen consisted of zidovudine, lamivudine, and lopinavir/ritonavir. 13
Testing procedures
An interviewer-administered questionnaire was used to collect sociodemographic information from participants at the beginning of the study. Anthropometry (weight and height) and DEXA were performed at baseline, 3, 6, 12, 18, and 24 months. DEXA (Discovery-W®, software version 12.7.3.7; Hologic, Bedford, MA) was used to measure fat mass according to standard procedures. DEXA cutoff lines positioned at anatomical markers were used to obtain fat mass for the whole body as well as for the various regions of interest (arms, legs, and trunk). The trunk comprised the region between the neck and waist, excluding the arms. Limb composition was determined by summing the arms and legs. The percentages for regions were calculated as a proportion of the whole body fat mass. A more detailed description has been previously described. 14 Abdominal visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) areas were estimated by a trained analyst using image analysis software (SliceOmatic V4.2; TomoVision, Montreal, Quebec, Canada). The DEXA measure of VAT has been shown to perform as well as VAT measured using CT scans. 15 Clinical records obtained from health facilities were reviewed to obtain information on ART regimens, viral loads (VLs), and CD4 counts.
Ethical approval
The study proposal was approved by the Research Ethics Committee of the Faculty of Health Sciences at the University of Cape Town. Written informed consent was obtained from all participants before participation in the study.
Data analysis
Data analysis was carried out using the STATA/SE statistical software package version 12.0 (StataCorp., College Station, TX). Baseline measurements were collected between November 2008 and November 2010. Because the data were not normally distributed, continuous variables were described as medians and interquartile ranges, and were compared using Wilcoxon Rank Sum tests. Binary variables were described using frequency and percentages, and compared using chi-square tests. The Jonckheere–Terpstra test for ordered variables was used to measure trends over time.
Lipoatrophy was defined as (1) ≥20% loss of limb fat (all limbs combined) from baseline [10] and (2) ≥10% loss of limb fat (all limbs combined) from baseline by DEXA scan. 16 Lipohypertrophy was defined as ≥20% gain in trunk fat from baseline by DEXA scan. 17,18 Differences in time to lipoatrophy and lipohypertrophy between men and women were calculated using the Kaplan–Meier method. The log rank test was used to test differences between groups. Cox proportional hazards regression modeling was used to analyze the contribution of the following variables, selected a priori: age, gender, body mass index (BMI), and individual NRTIs, and non-NNRTIs, to the development of lipoatrophy. The Cox proportional hazards assumption was not met for lipohypertrophy; therefore, logistic regression modeling was used to analyze the same variables as used in the lipoatrophy model. Latent class mixed effects models are used to estimate mean longitudinal trajectories in potentially heterogeneous populations, by assigning a model of latent factors that determines class membership. The number of classes was set a priori and class membership was estimated by posterior probabilities. Latent class mixed effects models were fit to longitudinal data for limb fat and trunk fat change independently, with the same set of covariates as prior regression models. Two and three class models were fit and the final model was chosen by best Aikaike Information Criterion. Posterior probabilities were estimated and latent classes characterized by summary statistics.
Results
Baseline characteristics of participants are shown in Table 1. The study sample consisted of 55 (29.4%) men and 132 (70.6%) women who were ART naive. Men were significantly older than women (35 vs. 31 years; p = 0.008). Significantly more women than men were obese (20% vs. 4%; p = 0.005). After baseline measurements were collected, 25 participants (13.3%) were excluded from further participation in the study as they either did not meet the eligibility criteria for ART initiation or their ART initiation had been delayed. The number lost-to-follow-up increased from 25 to 57 (30.5%) participants at 12 months and to 84 participants (44%) at 24 months on ART.
BMI, body mass index; IQR, interquartile range; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor.
Bold values indicate that p values are statistically significant.
More men (71%) than women (56%) were initiated on a stavudine-based regimen. After 12 months on ART, the proportion of participants on stavudine and tenofovir was no different than at baseline. However, after 24 months on ART, the proportion of participants on a stavudine-based regimen had decreased and those on a tenofovir-based regimen had increased. Only one participant was exposed to a drug regimen containing a protease inhibitor. After 6 months on ART, 73% of participants were virally suppressed (VL <50).
Change in weight, BMI, and regional DEXA fat measures in men and women over the 24-month follow-up period are shown in Fig. 1. In women, the total limb and trunk fat increased (p < 0.001), whereas limb fat as a percentage of whole body fat decreased (p < 0.001), primarily as a result of the decrease in leg fat (45.2–42.1%; p < 0.001). Trunk fat in women increased from 7.6 to 11.7 kg (p < 0.001). In men, none of the regional changes in fat distribution was significant other than trunk fat, which increased from 3.65 to 4.16 kg (p = 0.027). An increase in the derived variables of abdominal SAT and VAT was observed in both men and women (p < 0.05).

Body composition changes (weight, BMI, and DEXA measures) in men and women over 24 months. BMI, body mass index; DEXA, dual-energy X-ray absorptiometry.
Kaplan–Meier plots of time to lipoatrophy and lipohypertrophy in men and women are shown in Fig. 2. Lipoatrophy was observed in 20 of the 161 participants and occurred more frequently in men than in women (20% vs. 9.4%; p = 0.066), but this difference was only significant when lipoatrophy was defined as ≥10% loss in limb fat (42.2% vs. 22.2%; p = 0.011). Lipohypertrophy was observed in 90 of the 161 participants (55.9%), and was similar in men and women. Time to development of lipoatrophy and lipohypertrophy was not significantly different between men and women.

Kaplan–Meier curves of time to lipoatrophy and lipohypertrophy in men and women.
Men have a greater than two times increased risk of developing lipoatrophy (HR = 2.29 [0.93–5.66]; p = 0.071) than women (Table 2), adjusted for age, baseline BMI, and ART regimen. The risk of developing lipohypertrophy (Table 3) did not differ by gender, but showed a large (0.59 [0.23–1.52]; p = 0.271) effect, though not statistically significant. None of the antiretroviral drugs were significantly associated with lipoatrophy or lipohypertrophy.
BMI, body mass index; HR, hazard ratio; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor.
ART, antiretroviral therapy; BMI, body mass index; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; OR, odds ratio.
Bold values indicate that p value is statistically significant.
Latent class modeling was used to show limb fat and trunk fat change over time for each individual (Fig. 3 and Table 4). The mean posterior of class membership in the limb fat model was class 1 = 0.91, class 2 = 0.89, and class 3 = 0.85. The mean posterior probability for class membership in the trunk fat model was class 1 = 0.91, class 2 = 0.94, and class 3 = 0.82. For both limb fat and trunk fat, class 2 showed an increase over time.
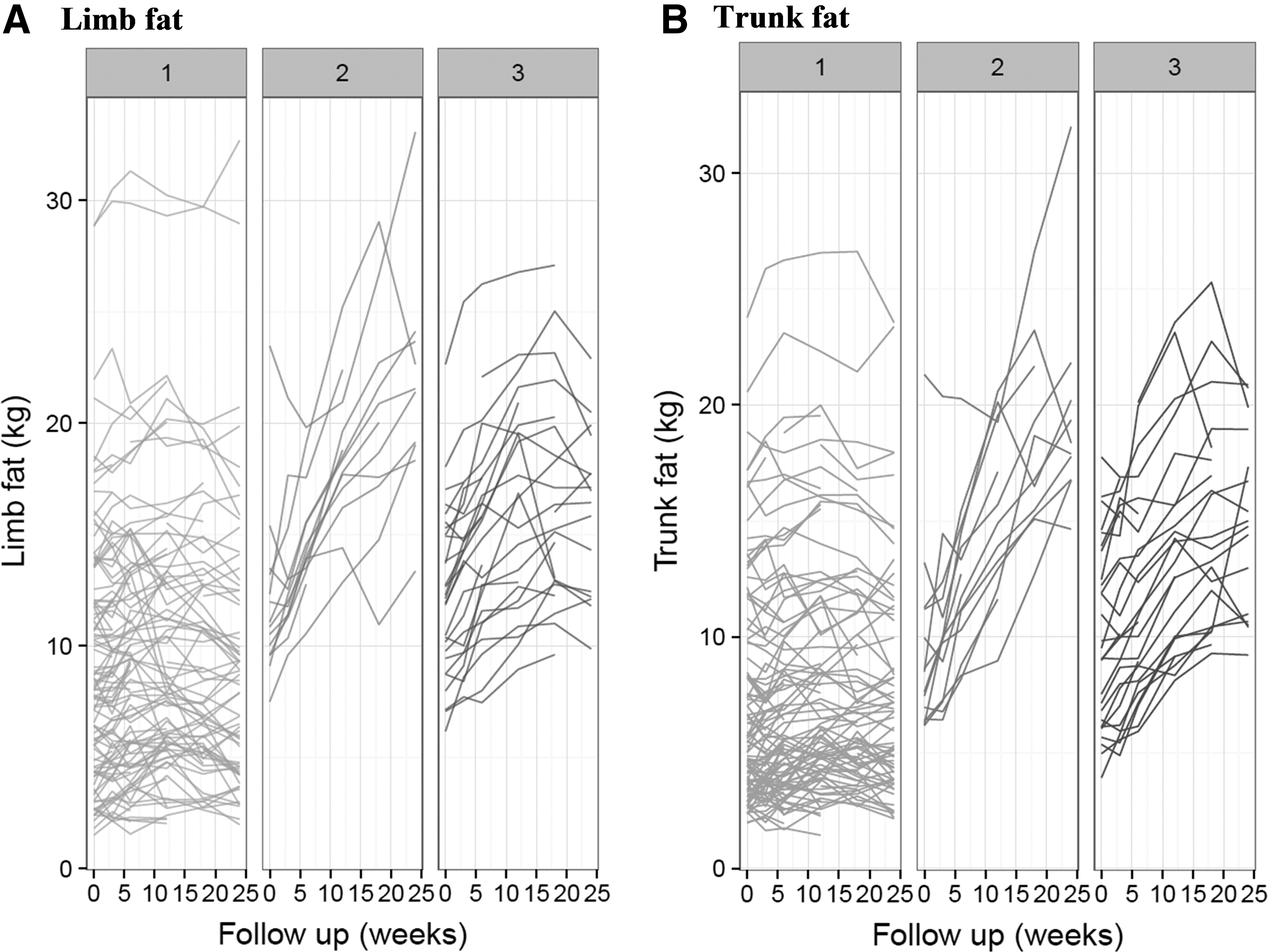
Limb fat
BMI, body mass index.
Discussion
This is the first longitudinal study from sub-Saharan Africa to document changes in body composition using DEXA in patients starting ART. After the initiation of ART, we observed striking gender differences in weight gain, with women gaining more overall weight and more regional fat in all areas analyzed on DEXA scans. Women, but not men, had a significant decrease in limb fat expressed as a percentage of total body fat, and a significant increase in trunk fat percentage, which are markers of lipoatrophy and lipohypertrophy, respectively. The incidence of lipoatrophy expressed as a categorical variable was higher in men than in women. The incidence of lipohypertrophy, when expressed as a categorical variable, occurred similarly in men and women. The derived variables, abdominal VAT and SAT, increased significantly from baseline in both men and women, with women gaining substantially more than men.
We found that men had a 2.3 times greater risk of developing lipoatrophy than women, and that lipoatrophy occurred more frequently in men. These data are supported by other studies; 10,19,20 however, the data are conflicting as there are also studies showing the risk in women to be greater than in men, 3,11 whereas others found the risk to be similar by gender. 21 The greater risk in men in our study may be because of their lower baseline BMI as well as having less body fat, especially in the limbs, than women. In addition, more men than women were using stavudine at baseline, even though the difference was not statistically significant. Epidemiological studies from South Africa show that in the general population, a smaller proportion of black men are overweight or obese than black women (38.5% vs. 64.8%). 22 Our study showed that after 24 months on ART, 12% of all participants developed lipoatrophy when defined by ≥20% loss of limb fat, and this increased to 28% when defined as ≥10% limb fat loss. This is lower than the findings in a large multi-center randomized control trial 10 that showed a 32% occurrence when defined by ≥20% limb fat loss and 40% when defined by ≥10% limb fat loss. The difference may be explained, in part, by the majority of male subjects in the multi-center trial versus the majority of women in our study.
In 2003, the Lipodystrophy Italian Multiculture Study 21 reported different changes in fat distribution in men and women on ART, with women being more likely to develop fat accumulation around the abdomen. Similarly in 2009, McComsey et al. 23 found that women had a greater increase in trunk fat, SAT, VAT, and TAT than men.
A systematic review 2 found that lipohypertrophy was not an adverse drug reaction, but appeared rather to be a consequence of treating HIV infection, which reduces the inflammatory response that causes wasting. Our finding that lipohypertrophy occurred with similar frequency in men and women irrespective of drug regimen is in keeping with the findings of the systematic review. By contrast, the systematic review found good evidence that lipoatrophy is an adverse drug reaction, due largely to thymidine analogue NRTIs, especially stavudine. We showed that the incidence of lipoatrophy was 45% less with tenofovir than with stavudine, in keeping with numerous studies, 3,24,25 but the difference was not statistically significant, likely because of our small sample size.
We also showed that over the 24-month period, weight and BMI increased significantly in both men and women. Interestingly, almost half of all women were either overweight or obese at the beginning of the study, when the criterion for ART eligibility was a CD4 count of <200 cells/mm3. Further, their median BMI increased from 24.8 to 27.7 kg/m2, and their median VAT increased by 190 g during the 2 years. However, when using latest class analysis, we found a heterogeneous group within the sample, with the majority of individuals experiencing a longitudinal trajectory of limited to no weight change over time. A minority of individuals, as supported by the other analyses, experienced longitudinal trajectories characterized by significant weight change, indicating that a minority of participants were responsible for the significant change in median weight and BMI. Our findings of increased weight and BMI mirror those of another South African study, 26 showing that the BMI in HIV-infected women increased from 25 to 27.4 kg/m2 during the first year on ART. Although the increase in weight and BMI may be because of a return to health in both men and women, a combination of mismatched weight perception and a cultural belief that underweight is associated with HIV infection may contribute to the increasing number of HIV-infected overweight and obese women. Studies on weight perception in HIV-infected women 26,27 reported a mismatch between actual weight and the weight perception, with a tendency for women to judge themselves as less than their actual weight. In South Africa, HIV-infected women continue to experience discrimination, which may be the cause of intentional obesity as a mechanism of limiting the stigma. 28 These findings are of great concern as an increased waist circumference, and especially increase in VAT, is associated with increased mortality in HIV-infected populations. 29
Our study has some limitations. This was a nonrandomized study, and there were no untreated or uninfected controls for comparison. The study sample was relatively small, with a high rate of loss to follow-up, resulting in a lack of power. There was minimal exposure to protease inhibitors, so we can only make inferences about first-line ART. Despite these limitations, this is the only study from Africa to use longitudinal DEXA data.
In conclusion, we found that body fat changes differed in men and women on ART. Men, more frequently than women, developed lipoatrophy, whereas the risk of lipohypertrophy was no different in men and women. The percentage of trunk fat in women, but not in men, increased significantly, with median BMI and VAT increasing substantially more in women than in men. Further investigation is required to understand the mechanisms underlying the sex differences and its effects on cardiovascular risk.
Footnotes
Acknowledgments
We thank Linda Bewerunge for doing the DEXA scans, Sasha West for anthropometric measurements, and Carmen Delport for coordinating the study.
Author Disclosure Statement
No competing financial interests exist.