
Abstract
As lifelong antiretroviral therapy (ART) for pregnant women is implemented, it is important to understand the attitudes and norms affecting women's postpartum ART adherence. This is a qualitative cross-sectional study of HIV-positive postpartum women (n = 112) enrolled in a 2-year observational prospective cohort in Rwanda. Informed by the Theory of Reasoned Action (TRA), we conducted in-depth interviews with women whose children were 0–6, 7–12, 13–18, or 21–24 months of age to describe factors contributing to adherence and changes over time. Positive ART attitudes reported by women included mothers' health promotion, prevention of infant HIV infection, higher CD4 count, and improved physical appearance. Negative attitudes were few, but included side effects and the lifelong nature of treatment. Learning from people living with HIV (PLHIV) was identified as a norm facilitating adherence; ART adherence was inhibited by fear of disclosure or stigmatization in communities and clinics. Poor adherence behaviors were common immediately after HIV diagnosis, not necessarily during prevention of mother-to-child transmission (PMTCT). Women with older children, most of whom stopped breastfeeding by 13–18 months, reported more barriers and missed doses than women with younger children. The TRA was useful in identifying the collective influence of attitudes, norms, and intentions on behavior. Findings suggest that HIV-positive women are vulnerable to poor adherence following HIV diagnosis and around the time of breastfeeding cessation. Lifelong treatment adherence can be supported through PLHIV exemplifying long-term ART use, fewer and less stigmatizing clinic visits, and counseling messages highlighting the benefits of drugs on appearance and illness prevention and incorporating biological feedback.
Introduction
I
Studies on longer-term postpartum retention help further understanding on adherence postdelivery, although there is limited evidence in Option B+ settings. Women who are not attending services and picking up their ART medication are also likely not complying with their treatment, but women may still remain engaged in care with inadequate adherence. 4 Few studies address maternal retention when women complete the PMTCT cascade and there is a need to tailor interventions by better understanding barriers to ensure women are adherent and remain engaged in care for their own health and subsequent pregnancies. 5 A study in South Africa found the perception that the mother cares more about her child's health than her own and lack of financial resources, conflict with work commitments, negative treatment by clinic staff, and denial or lack of disclosure of the mother's HIV status were challenges to postpartum retention under Option B+. 6 Barriers to postpartum retention in Tanzania included stigma and the perception that ART was unnecessary as the mother felt healthy, confusion about drug adherence or facility appointments, doubts about drug treatment bringing tangible benefits, and concern about side effects. 7
As Option B+ is still in its early years of implementation, an understanding of women's perceptions of ART and factors influencing adherence behavior can be utilized to develop effective counseling messages. Pregnant women in Ethiopia who received counseling on HIV medication, which included the advantages to adherence and antiretroviral (ARV) side effects, were nearly five times more adherent to Option B+ compared with those without counseling. 8 A lack of information and counseling was also highlighted as a challenge for women enrolling in Option B+ programs with same-day diagnosis and treatment in Malawi and Uganda. 9
Cross-sectional qualitative data on adherence were collected through one-time in-depth interviews (IDIs) from four different groups of HIV-positive women, who were already enrolled in a prospective cohort study: women with children 0–6, 7–12, 13–18, and 21–24 months of age. The aim of this study was to describe attitudes and norms contributing to adherence for women engaged in care and how these might change from around the time of delivery to when their child is at or near the end of breastfeeding. Understanding these factors will help to tailor counseling messages and to enhance clinic and support services to HIV-positive women during breastfeeding and following transmission risk to protect the health of the mother and her child.
Methods
The Kabeho Study was an observational prospective cohort of 608 HIV-positive women in Kigali, Rwanda, enrolled during the third trimester of pregnancy or within 2 weeks postpartum from PMTCT programs. Mothers and infants were followed until the children reached 24 months of age. As per national guidelines, the mother/child pair remain in the PMTCT program following delivery through ∼18 months postpartum. 10 HIV-positive mothers are counseled to cease all breastfeeding by the time the child is 16.5–18 months of age. Following breastfeeding cessation, children should receive a final HIV test. Mother/child pairs are transitioned to adult HIV/ART services once the child's final HIV status is determined, which could be later than 18 months if the breastfeeding period was extended or if the child is HIV positive.
Structured enrollment and monthly interviews
At the study enrollment visit, data collected from all women included demographics, HIV and ART-related information, and pregnancy history. Women then attended study visits each month that were often aligned with their routine clinic visits. At these visits, women were interviewed using a structured questionnaire on topics such as adherence measured by self-reported recall of doses missed in the past 3 days, side effects experienced in the past month, current breastfeeding practices, time counseled on ART, receipt of food supplementation, and any major household changes. RNA-polymerase chain reaction (PCR) testing for VL in women was done at the time of enrollment, delivery, 18, and 24 months postpartum by the National Reference Laboratory using the Roche COBAS Ampliprep/COBAS TaqMan HIV-1 (V2.0). As standard of care, CD4 testing was conducted for all women testing HIV positive at antenatal care (ANC) clinics and then every 6 months thereafter. CD4 test results were abstracted from women's medical records if available.
All interviews were conducted in Kinyarwanda. Responses from enrollment and monthly visit interviews were documented on paper forms and electronic tablets. Data were reviewed for completeness and quality and entered into the study database using a data capture system (SurveyCTO, Version 2.10, Dobility).
In-depth qualitative interviews
A subset of women were recruited to participate in IDIs. To ensure equitable representation of women's perceptions and experiences throughout the postpartum study period and to identify any potential differences over time, the postpartum period was divided into four child age ranges (0–6, 7–12, 13–18, and 21–24 months of age). Recruitment was conducted concurrently at all 14 study facilities during women's monthly study visits. Approximately two interviews per age range per facility were targeted with an overall target of 28 women in each child age group. Beginning the first day of recruitment for qualitative interviews, which was determined by study coordinators, study nurses recruited participants consecutively until targets for each age group were reached. Recruitment took place from July 2014 to July 2015. Women who refused for one age range interview were not asked to participate again. Interviews either took place during a regular study visit or at another time convenient to the participant. No woman was interviewed more than once. Interviews covered aspects of adherence and infant feeding in the context of the Option B+ program; this article presents women's perceptions and experiences of ART and ART adherence. Questions included the following: What do you think about taking lifelong medicine? How have your thoughts about taking medicine every day changed from when you started until now? What motivates you to take your medicine every day? What have been your main challenges with taking the medicines? What do people say about this medicine?
All study staff received multiple trainings on data collection and on research with human subjects. Study nurses were also trained in qualitative interviewing, including topics such as active listening and probing, in addition to repeated practice with the interview guide. Study coordinators reviewed interview recordings for quality. Any areas of weakness identified were addressed through individual or group refresher trainings to improve subsequent interviews.
IDIs lasted ∼1 h. They were audio-recorded, transcribed, and then translated from Kinyarwanda to English. A standardized codebook was developed based on the Theory of Reasoned Action (TRA) and included groups of codes comprising the major theoretical elements: attitudes, subjective norms, intention, and behavior. 11 Four trained members of the study team coded transcripts using MAXqda (V10, Marburg, Germany). Each transcript was coded by a single rater who worked with other raters to determine how to code ambiguous segments of text. Textual data were first read carefully by an investigator. Data were then reduced to matrices, in which each code was analyzed separately by the four infant age groups and organized by theoretical element. Thematic content analysis was used to identify similarities and differences between age groups and overall patterns in the data. 12 These patterns and their nuances were continually reviewed, referring back to original transcripts as needed. Other data, such as perspectives on lifelong treatment, were further analyzed according to whether or not women were on ART at their first ANC visit.
Selected demographics and HIV/ART history
Data from the structured interviews at enrollment were extracted from the overall database for study women who participated in IDIs. Structured interview data in the postpartum period were also extracted from the monthly follow-up visits, which correspond to the specified time period in which women participated in IDIs. For instance, if a woman participated in an IDI when her child was between 7 and 12 months of age, selected HIV/ART information from monthly visits she attended during the 7- to 12-month timeframe was extracted. Since women may have attended multiple study visits within the child age range, responses for current ART regimen and recall of missed doses were included from the last visit women attended within the timeframe or child age range in which the IDI took place. Because changes, such as divorce or job loss, could have long-lasting effects on adherence, events were included if they occurred anytime within the interview time period plus 6 months on either end of the age range if applicable (e.g., any events occurring from 0 to 12 months for the 0- to 6-month child age group and from 7 to 24 months for the 13- to 18-month child age group were included).
Descriptive statistics were calculated overall and stratified by child's age group at the time of women's IDIs. Medians were reported with interquartile ranges for all continuous variables, and frequencies were reported with percentages for all categorical variables. The data analysis was generated using SAS/STAT software, Version 9.4 (SAS Institute, Inc., Cary, NC).
Ethical considerations
All women provided written informed consent to participate in this minimal risk study. Ethical approvals were obtained from the Rwandan National Ethics Committee, the Rwanda National Health Research Committee, and the George Washington University Institutional Review Board. The protocol is registered with the US National Institutes of Health at
Results
Study population
In each of the four child age ranges, 28 women enrolled in the Kabeho Study participated in an IDI for a total of 112 women or nearly 20% of the cohort. Forty-four women refused to participate in these interviews, citing lack of time as the main reason. Selected demographics and HIV and ART history from the enrollment visit by the child's age group are presented (Table 1). Women had a median age of 30 years (IQR 26–34) and 41.0% (n = 43) were diagnosed with HIV more than 5 years before study enrollment; 70.9% were on ART before pregnancy with nearly half (47.3%, n = 53) on ART for one or more years before their first ANC visit for their current pregnancy. The most common ARV regimen (53.6%, n = 60) was tenofovir (TDF), lamivudine (3TC), and efavirenz (EFV). Only two women who participated in the interviews experienced a regimen change during the study: one in the 7- to 12-month and one in the 13- to 18-month age group. Most women (82.1%, n = 92) had disclosed their HIV status to their partner.
ART, antiretroviral therapy; IQR, interquartile range.
Selected HIV/ART information from postpartum visits of women who participated in an IDI by child's age is presented (Table 2). The majority of women reported that they took all their doses in the last 3 days (95.5%, n = 106). The number of women who reported side effects was low overall (17.0%, n = 19), with a trend toward decreasing side effects in women in the older child age groups. There were similar numbers of viral suppression across the time points: 83.9% (n = 94) of women at enrollment, 92.0% (n = 23) at delivery, 73.9% (n = 17) at 18 months, and 81.8% (n = 18) at 24 months of age had a VL of <1000 copies/mL. The lowest proportion of viral suppression was among mothers in the 13- to 18-month child age group; this group also had the most mothers on ART for more than 1 year (n = 18) compared with the other child age groups. Between the 7- to 12-month and 13- to 18-month child age categories, the majority of women switched from breastfeeding their infants (75.0%, n = 21) to no longer breastfeeding (78.6%, n = 22), respectively. The number of women who received ART counseling at any visit in the timeframe decreased with increasing child age; however, the time spent counseling remained fairly consistent and was a mean of 5 min overall [standard deviation (SD) 3.5–10.0]. Only 33.0% (n = 37) received food supplementation at any visit in the timeframe. The most common major household changes were move from residence, divorce/separation, job loss, and a change in household members. Women in the 13- to 18-month child age group experienced the most events (37.0%, n = 20), followed by women in the 0–6 child age group (29.6%, n = 16).
Only 84 women could have contributed viral load outcomes here as it was assessed at delivery, 18, and 24 months.
Some women reported more than one side effect.
Average time spent counseling was first calculated for each woman at all visits within the timeframe in which ARV counseling was provided, then an average for all women within the timeframe was calculated.
3TC, lamivudine; ART, antiretroviral therapy; ARV, antiretroviral; AZT, zidovudine; EFV, efavirenz; NVP, nevirapine; SD, standard deviation; TDF, tenofovir.
Three of the children whose mothers were interviewed became HIV infected during the study period. Two of the children were identified as infected at 6 weeks, both of whom were aware of the infection at the time of the interview; one woman was interviewed when the child was aged 21–24 months and another was interviewed when the child was <6 months of age. The woman interviewed when her child was 13–18 months of age did not receive a diagnosis of HIV infection in her infant until 24 months. All three mothers with infected children were on ART at first ANC visit.
Qualitative findings
The findings are organized according to the adapted elements of the TRA: positive and negative behavioral beliefs and attitudes, subjective norms, behavioral intention, and the behavior (ART adherence). Element definitions were adapted from the original theory (Fig. 1). Table 3 includes illustrative quotes to exemplify each of these components.
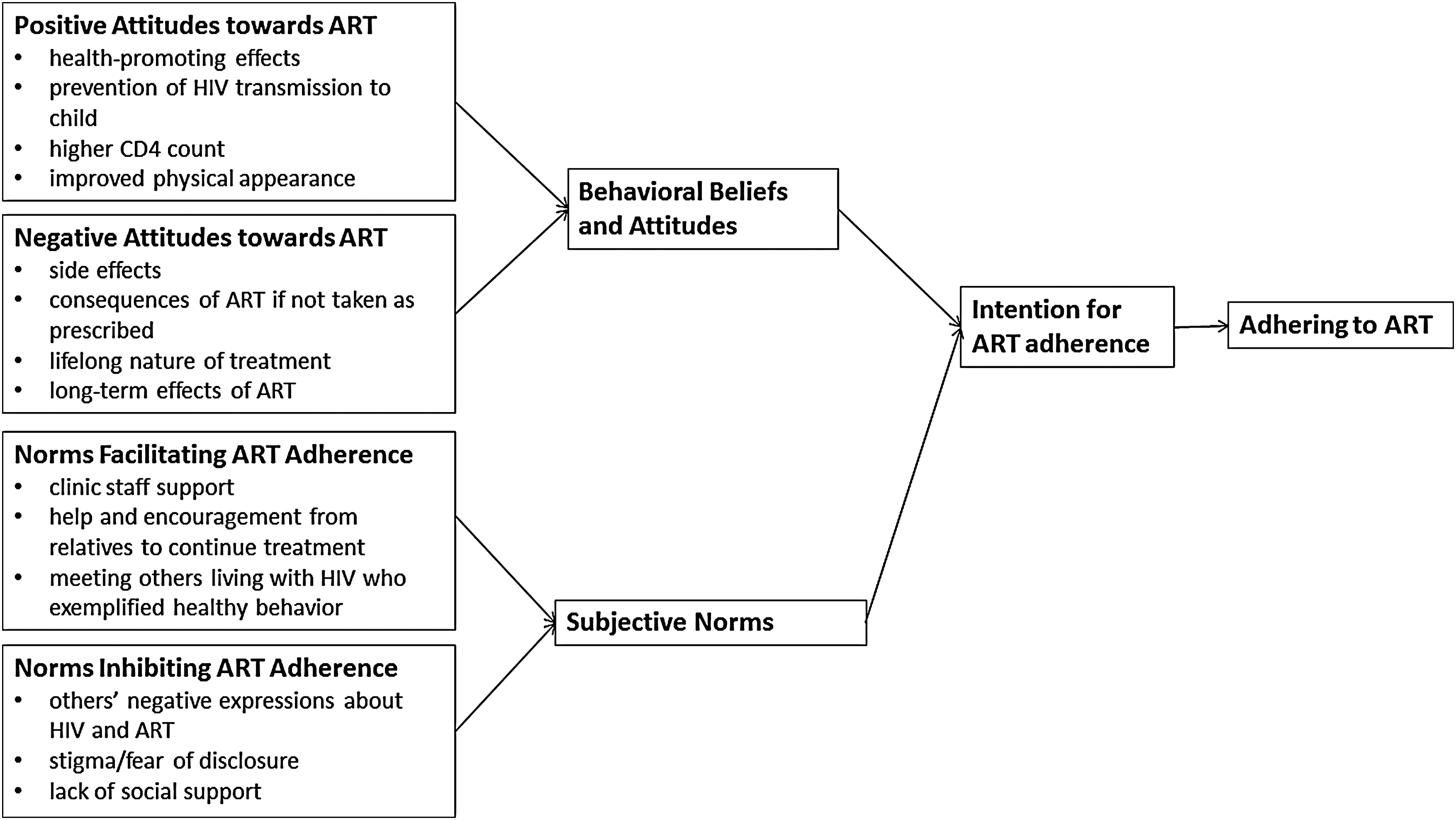
Adapting the theory of reasoned action: ART adherence among Kabeho study mothers. ART, antiretroviral therapy.
ART, antiretroviral therapy; ARV, antiretroviral.
Behavioral beliefs and attitudes
According to the TRA, a behavioral belief is defined as a “belief that behavioral performance is associated with certain attributes or outcomes” and an attitude as the “overall evaluation of the behavior.” 13 As women have already started taking ART and have varying levels of adherence, these factors reflect attitudes based on their experience or belief that adherence will lead to a particular outcome either positive, such as PMTCT, or negative such as long-term negative effects of ART use.
Positive attitudes toward ART
Positive outcomes of ART adherence reported by women included health-promoting effects, preventing transmission of HIV to their infant, higher CD4 count, and improved physical appearance. Unless noted, perceptions were mentioned in generally the same frequency across mothers in all child age groups.
Mothers' health promotion was the most commonly cited positive ART attitude across all age groups, although most often in the 21- to 24-month child age group and least often in the 13- to 18-month child age group. Women reported that ART allowed them to be healthy and live longer lives, regain or improve their strength, prevent opportunistic infections (OI), and decrease the frequency and severity of other illnesses. Skin infections were most frequently mentioned as having been avoided or no longer occurring. Other illnesses were mentioned—cold, pneumonia, and malaria—in which women felt they suffered less intensely than before ART initiation. Some women explained further that they wanted to be healthy and strong and remain alive to raise their children, work, and be productive. This desire seemed to be critical in women's acceptance of lifelong treatment. They valued living healthier, presumably longer lives, with fewer episodes of illness and hospitalizations and visible physical improvements. Therefore, they recognized their lifelong adherence to ART as the path to sustaining good health, particularly if they initiated ART when they were sick, and believed that stopping their treatment would lead to a reversal of these benefits. Indeed, some women who missed doses noticed immediate adverse physical changes.
Protecting their child from HIV during pregnancy and breastfeeding and keeping him or her healthy were also frequently reported. References to the positive attitude surrounding PMTCT in the interviews decreased slightly in the interviews with women who had older children (13–18 and 21–24 months).
Several respondents in similar numbers across all four age group categories mentioned their increasing CD4 levels as contributing to their positive attitudes toward ART. Some women were even able to cite their past and current CD4 counts from memory during the interviews and credited their adherence to treatment for the increase.
Some women reported that they could hide their HIV status and thus reduce potential stigma due to the improvements ARVs brought about to their physical appearance. Taking their medication helped to avoid disclosure to those whom they did not want to tell because they looked healthy (e.g., no visible skin rashes, normal weight).
Negative attitudes toward ART
There were relatively few negative attitudes toward ART reported by women. They included side effects, consequences of ART if not taken as prescribed, the lifelong nature of treatment, and the long-term effects of ART. Negative perceptions were reported similarly across all age groups, except where noted.
Of those who reported side effects, nearly half said that they only occurred at the start of treatment; they either became accustomed to ARVs or their regimen was switched in a few instances before or during the study period. Dizziness was the most reported side effect and was often attributed to lacking sufficient food with which to take their drugs. In particular, many commented that ART caused weight gain and increased appetite, although weight loss following ART initiation was reported by a few participants. While weight gain could be perceived as a positive benefit of ART use, it became a source of gossip for people living with HIV (PLHIV) on treatment. ART was dubbed pork medicine, reflecting the perception that those taking it crave meat and have insatiable appetites. People taking ARV drugs that cause weight gain were ridiculed; however, if someone was very thin, it may be assumed that s/he has AIDS and could also be subjected to derision.
Several respondents stressed the negative consequences of ART if it is not taken as prescribed. This was often expressed as the development of OI or that the disease would become more virulent if doses were missed or medication stopped. As noted above, this often motivated women to continue treatment. However, in some cases, consequences were described in an alarmist manner, either from the women's own viewpoints or what they had heard others say. For example, they heard that death may result if drugs were not taken with food or if doses were missed and that the drugs themselves were so potent they could cause death.
When asked specifically if they had problems with taking drugs every day or with the experience of lifelong ART, approximately half of the respondents answered that lifelong ART posed no challenges or problems for them. However, this number decreased with increasing child age, with few such responses in the 21- to 24-month child age group. Women who identified taking ART for life as a challenge usually qualified it by saying that there was no other option but to accept lifelong treatment.
Only a few respondents expressed concern about the long-term effects of drugs, including liver problems and those affecting their reproductive health.
Subjective norms about ART behavior
Subjective norms are defined according to the TRA as “beliefs about whether most people approve or disapprove of the behavior.” 13 This section is divided into norms that facilitate ART adherence (involving those who approve of the behavior) and norms that inhibit ART adherence (involving those who disapprove of the behavior) directly or indirectly.
Norms facilitating ART adherence
Respondents described individuals or groups that they believed to support positive ART adherence behaviors and how they motivated women to adhere to treatment. These included counseling by clinic staff, help and encouragement from those close to women to continue treatment, and meeting with PLHIV who exemplified healthy behavior as a result of ART use. Overall, these norms were reported most frequently for the 0- to 6-month child age group and least frequently for the 13- to 18-month child age group.
The support and counsel provided by clinic staff, including doctors, nurses, and counselors, as well as the study nurses, were frequently reported as contributing to women's continued adherence to ART, particularly in the 0- to 6-month child age group. This advice was largely instructive in nature (e.g., taking the pills each day as prescribed, the importance of eating well), but clinic staff also seemed to offer comfort that encouraged women to take their drugs.
Encouragement to continue ART and support in various forms from relatives and household members also motivated women similarly across all child age groups to adhere to their medication. This included instrumental support, such as reminding women to take their drugs, attend their clinic appointments, and refill their prescription and picking up drugs for women when they were unavailable. This supportive role was most often the woman's current partner, but parents, siblings, friends, and neighbors to whom women have disclosed (and children in a few cases) were also mentioned as providing this type of support. Several women mentioned that their husbands were also HIV positive and they reminded each other to take their medicine. Emotional support from husbands and others included encouragement to continue ART by reinforcing the benefits of doing so, consolation by emphasizing that ART is not a death sentence and many are afflicted with the same disease, and help coping with idea of taking drugs every day for life.
Another key group providing support were other PLHIV, either existing friends or relatives or women met through the PMTCT program, such as cooperative group members. PLHIV expressed concern for the life and health of women and conveyed to them that to be well and have healthy children, it was important to take medication as prescribed and follow clinicians' instructions. Women, particularly those in the 0- to 6-month child age group, were also greatly encouraged by others who have been on treatment for the long term and who were living regular lives.
Norms inhibiting ART adherence
On the other hand, women also identified individuals who could inhibit their adherence. This included others who viewed ART negatively, those women feared disclosing to, and close family members who failed to provide support. Overall, women with children in the older two child age groups described inhibiting norms most frequently.
Not all PLHIV were promoting positive adherence behaviors. Women described others they knew who refused treatment or did not take their drugs as prescribed. Some PLHIV thought they would die even with ART and thus they continued drinking alcohol while taking medication or believed in a religious cure, for example. These reactions were viewed as being unappreciative of ART. However, many of the negative comments about HIV and ART were stated by people who were (presumably) HIV negative. This included ridiculing PLHIV for eating too much as described above and referring to ARV in a derogatory manner. Women indicated that because others did not experience the disease, what they said about ART was generally not viewed as credible.
Fearing disclosure or stigmatization due to HIV status was fairly consistent across all child age groups. This generally took the form of not wanting to attend the clinic for fear others would see the woman in a particular queue or waiting area or having to hide pill taking in the presence of others, resulting in missed or ill-timed doses. Several women mentioned attending clinic services far from their homes to avoid people from their communities seeing them at the clinic, which may exacerbate challenges of paying or arranging transport. A respondent suggested private rooms at clinics to serve HIV-positive pregnant women because other clients gossip when they see them in an area designated for HIV services. Of particular concern was women's fear of taking their ART as well as administering the infant nevirapine (NVP) doses in the maternity ward. Some felt other women would stigmatize them, while others feared stigmatization from the medical staff. Although most women had disclosed to someone, some still described challenges with not yet disclosing to a husband, close family members, or coworkers.
While not as frequently reported as the others, lack of support or rejection resulting from disclosure of women's HIV status was a notable norm inhibiting adherence, largely reported by women with children in the older two age groups. This was most often not only from husbands or partners but also included the woman's family and ranged from failing to support women to attend the clinic or take medication to abandonment after testing HIV positive.
ART adherence intention
Intention is defined according to the TRA as the “perceived likelihood of performing the behavior.” 13 Some respondents reported no challenges with taking their medication, while others acknowledged challenges, but resolved to do whatever was needed to adhere to their treatment. This included ensuring there was money to buy food to eat with medication and complying with clinic appointments, even when it meant walking to the clinic when one could not afford the transport fare or missing work to respect the appointment. Other women persevered through the experience of side effects or vowed not to concern themselves with what others might think who see them taking drugs or attending the clinic.
However, before study enrollment, many women—both ART-experienced and ART-naïve at the first ANC visit as well as the three women with HIV-infected children—described an initial struggle to adhere to their medication when first prescribed. A lack of intention among these women was often signified by hopelessness upon learning their HIV status and the need to take lifelong ART, a belief that they would die regardless of medication and occasional suicidal ideation. They most commonly cited meeting and learning from other PLHIV as the turning point to acceptance and eventually adhering to treatment. Other factors contributing to this turning point included advice from clinicians and other important people in their lives as described above, experiencing tangible improvements to their health (e.g., weight gain), or becoming pregnant. The coping process took anywhere from a week to several months.
ART adherence behaviors
Women committed themselves to taking their drugs on time at the same time every day. This was facilitated by having someone remind them, using their phone alarm as a reminder, or other external triggers, such as the start of a radio news program or the call to prayer at a nearby mosque, and encouraged by those who supported their adherence as described above. Sometimes women missed doses or took them late; this was most frequently mentioned by women with children in the oldest age group. Women pointed to forgetfulness and being too busy as reasons for missing doses. It was not common practice for respondents to keep their drugs with them (likely due to fear of inadvertent disclosure), so doses were also skipped if they worked late or traveled and forgot to pack them.
More serious adherence breaches were reported infrequently, including initial treatment refusal and treatment interruption, typically outside of the study period. This often occurred among women who struggled at first with living with HIV and who lacked an explicit intention to adhere to their medication and the support to do so. Women across all child age groups reported that lifelong ART was something they needed to become accustomed to first and that acceptance took time. Some women described their current drug-taking behavior as habitualized as eating or drinking. Others reported that they have now coped because there is no other choice but to take the drugs, even in the face of challenges or despite their dislike of pill taking.
Discussion
When examining ART adherence of HIV-positive women enrolled in the Rwandan PMTCT program over time using the TRA, attitudes and intentions leading to poor adherence behaviors were most prominent immediately after HIV diagnosis, which was not necessarily during the PMTCT period. This was true for both ART-naïve and ART-experienced women at first ANC visit. However, there was a trend suggesting decreased adherence among women later in the 2-year postpartum period, around the time most women stopped breastfeeding.
Women did not immediately accept their HIV diagnosis and treatment to take for life, although they varied in the length of time needed to cope with such information. For some women, their initial struggle with adherence was primarily due to the experience of drug side effects, which improved with time. Other women described feeling hopeless and near death and did not believe medication would lead to improvement. McMahon et al. also described this despair among women learning they were HIV positive or as a result of being stigmatized. 7 Our qualitative data indicate that the proximity to diagnosis was particularly detrimental to their treatment habits. The risk of mother-to-child transmission is greater in women first learning they were HIV positive and starting ART during pregnancy. 14,15 Short ART duration could also be exacerbated by inconsistent or interrupted drug taking during the early treatment stage. Enrollment for this study took place 1 year after the policy of universal lifelong treatment for pregnant women was implemented, and ∼70% of women in our study knew their status and were on ART before their first ANC visit. This suggests that Option B+ programs will become more effective as they mature as greater numbers of women will be on ART for subsequent pregnancies and will have already adjusted to their medication.
All women interviewed had stopped breastfeeding by 21–24 months of age and most had stopped by 13–18 months, thus capturing perspectives of women with children who were no longer at risk of transmission. Tanzanian women with increasing VL revealed a decrease in motivation to take their drugs following successful weaning and a final HIV-negative test result of their child. 16 Even for virally suppressed and thus likely adherent postpartum women in South Africa, 10–26% did not remain engaged in care and treatment services. 17 In contrast, Haas et al. found that women demonstrated the poorest adherence during the first 3 months after delivery, suggesting that women immediately postpartum, facing the demands of caring for a new infant while continuing to take their own medication, may experience greater adherence challenges. 4
Findings from this study also suggest that women may be vulnerable to poor adherence as the focus of their motivation shifts from preventing HIV transmission to their infant to taking ART solely for their own health. While numbers were low and the majority of women had a VL of <1000 copies/mL, those with children in the 13- to 18-month age group were least often virally suppressed and had been on ART the longest. They reported the fewest number of facilitating factors and reported inhibiting factors more frequently than the younger two child age groups. They were less likely to cite the promotion of their own health and their child's health as positive ART attitudes when compared with the other groups. It should be noted that women in this group also experienced the greatest number of household changes and it is difficult to know the extent to which these life experiences affected their adherence independent of infant transmission risk. Fewer women in the child 21- to 24-month group indicated that they were comfortable with lifelong ART, compared with the other age groups, although they did not report more problems with ART than other women. Finally, there was a greater frequency of reported missed or late doses among women of older children. This may reflect fatigue with taking pills or simply represents a longer time period with which to make errors.
Women in this study were greatly influenced by those who were promoting positive ART behaviors. An important factor was women's interactions with those who strengthened normative beliefs about ART adherence through instrumental and emotional support and encouragement of proper drug-taking behavior. This was perhaps most effectively facilitated by PLHIV; by sharing their testimonials of long-term ART use, PLHIV conveyed to women that ART adherence can lead to healthy productive lives and raising HIV-negative children.
Identifying someone for support, ideally immediately following treatment initiation, will help to promote good adherence and treatment acceptance. Women who initially struggled to adhere cited interaction with other PLHIV as the impetus for eventually accepting their status and treatment more than any other factor. It was also mentioned most frequently by women with children in the youngest age group, 0–6 months, who may have more recently learned of their HIV-positive status or initiated treatment. While linkage with PLHIV is critical in the early postpartum months, emotional and instrumental support was reported consistently as facilitating adherence across all child age groups, suggesting its continued importance. In a systematic review, treatment supporters (as friends, family, community health workers, or PLHIV) were found to significantly improve adherence in intervention versus comparison groups. 18 Another study from Rwanda found that being part of a support group for PLHIV led to increased HIV-free survival of their children by 30%. 19
Others' perceived negative attitudes toward ART, particularly those not HIV positive, seemed to contribute minimally to women's adherence. However, stigma surrounding HIV and ART and fear of inadvertent disclosure were raised repeatedly by respondents. The concern that someone they know will see them when attending the clinic has often been reported as contributing to poor adherence. 6,7,16,20 Changes at the facility level could encourage better clinic attendance, such as having all women in the same waiting areas so that HIV-positive clients are not easily identified by other patrons. Establishing a private space to take their drugs and administer the newborn NVP dose would also help to ensure that this critical first dose is not missed during labor and delivery. Other facility-level changes to encourage attendance by making it less time-consuming should be considered, such as those related to clinic flow and staffing to minimize waiting times and less frequent visits when appropriate. Roy et al. has suggested that increased visit spacing for HIV-positive clinically stable adults on ART, particularly if replaced by community-based service delivery, could improve efficiency at facility level and contribute to better retention outcomes. 21
Counseling messages should also highlight the benefits of drugs on appearance as well as the prevention of OI and other illnesses and incorporate biological measurements to illustrate healthy progression. A study in Malawi similarly found women's attitudes toward Option B+ to be largely health enhancing, with a reduction in illness, and noted that identifying people as HIV positive was no longer obvious since medication generally gave people a healthy appearance. 22 A fear of inadvertent disclosure can be turned around and used in counseling as a reason to accept and adhere to treatment. It could be reasoned that if medication is taken consistently and as prescribed, women may appear healthy and others will be less likely to suspect they are HIV positive. Many respondents also experienced an increase in their CD4 count as a result of ART, suggesting that immunological proof of improvement in health can serve as an effective tool in adherence counseling. While CD4 testing in Malawi is no longer required before pregnant or breastfeeding women are initiated on ART as a way of reducing barriers to treatment and simplifying the process under Option B+, recipients of the program still expressed a desire for testing. 22,23 What seemed to be important is having some biological measurement demonstrating the positive effects of their adherence. As VL monitoring and communication and follow-up of VL results with clients become more standardized as a part of care, they could have a similar impact as a motivating factor for adherence. 24
To our knowledge, this was the first study to use the TRA to explain adherence in this context. The framework was useful in identifying the collective influence of attitudes, subjective norms, and intentions on behavior. However, women generally demonstrated good adherence by the time they were interviewed postpartum, as evidenced by the qualitative responses as well as the VL results and pill recall, and described their journey to lifelong ART acceptance retrospectively. Their current perceptions and experience of ART may have colored their initial feelings. The model also did not explicitly allow for life experiences that may influence the behavior, but are not directly related to adherence, such as residence changes or job loss. They were also not directly explored in the qualitative interviews.
This study has other limitations. It did not follow the same women through each of these time periods to capture how perceptions and behaviors changed over the 2 years. Second, women had varying levels of exposure to ART and prophylaxis before study enrollment for this pregnancy, which may influence their perspectives. Positive attitudes, norms, and intentions of ART adherence could be overestimated, as women who were lost to follow-up and could not be interviewed might have different, possibly unfavorable, views regarding ART adherence. This study only focused on adherence for those who were retained in care. Moreover, by virtue of participating in the Kabeho Study, which provides regular contact with another nurse in addition to clinic staff, respondents may also have had a more positive experience with the PMTCT program overall. However, women were asked to speak about the perceptions of others and how their experience with drug taking changed from when they first learned they were HIV positive or initiated on treatment. It is through these responses that a more balanced picture of ART was described. Finally, the number of women in each group was small, thus only allowing for descriptive, rather than statistical, interpretations of differences among the four child age groups.
Despite limitations, this study provides continued evidence that the most critical time to provide support to HIV-positive women and others enrolled in universal treatment programs is at the time of ART initiation, as intentions to comply with lifelong treatment are nascent, particularly if this also coincides with their HIV diagnosis. Findings also echo other studies, in that women may be at risk of poorer adherence around the time of breastfeeding cessation. Interventions to support adherence in PMTCT include facility-level changes to make clinic visits for drug refills fewer and less stigmatizing and time-intensive and to tailor counseling messages, which highlight the benefits of drugs on appearance and illness prevention and incorporate biological feedback to illustrate healthy progression. Most importantly, women should be assured by clinic staff, loved ones, and other PLHIV that proper adherence can bring about desired outcomes. A better understanding of women's attitudes toward ART and factors contributing to their adherence following delivery, the weaning of their children, and beyond can be used to help women optimize their adherence so that they and their children lead healthy lives and uninfected children remain HIV free.
Footnotes
Acknowledgments
This study was funded by the US President's Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development and the generous support of the American people through USAID Cooperative Agreement No. AID-OAA-A-12-00024. Individuals employed or contracted by the funders did not contribute to the study design, data collection and analysis, decision to publish, or preparation of the article. The authors thank all of the Kabeho Study participants and the staff at study sites for their participation. The authors also recognize all current and former investigators, Kabeho Study nurses, the support team at EGPAF, and fellows at the EGPAF Rwanda office for their dedication, attention to detail, and commitment, as well as the Rwanda National Reference Laboratory, and colleagues at USAID for their technical support. Finally, the authors would like to acknowledge Laura Guay for her study leadership since the beginning and Lynne Mofenson for her critical review of the article.
Author Disclosure Statement
No competing financial interests exist.