
Abstract
We assessed the value of screening for cognitive abnormalities in a chronically infected HIV population (N = 388) and investigated the association with clinical correlates. The mean age was 48 years (±11), the majority of the patients were male (89%), the median duration of infection was 6 years [interquartile range (IQR) = 2–12], the median CD count was 600 (IQR = 450–780), and 326 (84%) had a viral load below 200 copies/mL. Screening for cognitive complaints was applied using the three Simioni questions and the international HIV dementia scale (iHDS). Neuropsychological assessment (NPA) included 13 well-validated tests assessing motor speed, concentration, and memory. A total of 69 patients completed the NPA. CD4 (nadir), viral load, combination antiretroviral therapy (cART) duration, and the presence of comorbidities were evaluated for associations with NPA result. A total of 127 (33%) reported cognitive complaints during screening. The sensitivity and specificity of the Simioni questions were 82% and 24%, respectively. Adding the iHDS resulted in a sensitivity of 50% and a specificity of 73%. A CD4 nadir count <50 cells/m3 was associated with an abnormal NPA (p = 0.01). Comorbidities were more prevalent in patients with an abnormal NPA, although not statistically significant (p = 0.276). Age, current CD4, viral load, and cART duration were not associated with abnormal NPA. The authors conclude that current screening strategies are insufficient in detecting HIV-associated neurocognitive disorder. A low CD4 nadir is associated with poor neurocognitive outcome in HIV.
Introduction
H
The European AIDS Clinical Society (EACS) advises treating physicians to actively screen for cognitive complaints in their patients. Not all patients who are eligible will be referred due to the limited capacity of neuropsychologists and relatively high percentage of patients at risk. Screening tools could reduce the quantity of wrongfully referred patients. These tools assist the clinician in deciding to refer patients for further neurocognitive evaluation by standardizing the neurocognitive screening procedure. A number of screening tools exist to assess cognitive functioning, such as the Mini-Mental State Examination, 4 the Montreal Cognitive Assessment, the HIV Dementia Scale, 5 and the more widely used international HIV Dementia Scale (iHDS). 6 Since HIV is regarded nowadays as a chronic illness, studies investigating cognitive dysfunction in HIV should account for factors such as treatment duration and age. It remains unclear whether screening tools remain specific enough in an aging study population.
Comorbidities in HIV-infected individuals have gained a great deal of attention in the recent decade. Although cART initiation greatly reduces AIDS-related diseases, chronically infected individuals seem to remain at increased risk for other, non-AIDS-associated illnesses such as cardiovascular disease, metabolic abnormalities, and certain malignancies. 7,8 For some comorbidities, such as vascular deficits, it seems understandable that they could negatively impact cognition. With the increasing age of the HIV-infected population, the chance of developing such comorbidities increases. The percentage of people living with HIV above the age of 50 has risen from 39% to 45% in the past 3 years in the Netherlands. 9 Whether a relationship between comorbidities and cognitive deficits exists remains uncertain.
The present study aimed to address the use of cognitive screening instruments in HIV-infected individuals in an uncontrolled clinical setting. We investigated the prevalence of cognitive deficits in a chronically HIV-infected cohort with a mean age of 48 years, a generally favorable immune status, and with a large majority being virally suppressed below the level of 200 copies/mL. We hypothesized that the most widely used screening tool for cognitive disorders in HIV, the iHDS, is sensitive to detect cognitive deficits. We investigated whether known correlates of disease severity remained adequate clinical predictors for HAND. Considering the potential impact of non-neurological comorbidities, we also determined the burden of non-neurological comorbidities in HIV-infected patients with and without cognitive deficits.
Methods
The TREVI study was designed to investigate the prevalence of cognitive disorders in a well-treated HIV population. We recruited patients attending the outpatient clinic of the Erasmus Medical Center in Rotterdam (The Netherlands) in consecutive order for a period of 1 year between December 2012 and December 2013. All patients had to master the Dutch or English language to appropriately compare the NPA. Patients with major neurologic comorbidities that could affect the outcome of NPA were excluded. Patients were asked to participate in neurocognitive screening and sign the informed consent. Patients were asked if they had any cognitive complaints, based on the three Simioni questions as advised by the EACS guidelines. 10 This included any problems encompassing concentration, attention, and/or memory that patients perceived in their daily lives. A trained research assistant screened patients using the iHDS. A cutoff score of 10 is currently applied to determine whether patients are indicated for further investigation. 6 Patients were consecutively asked to participate in NPA and divided into two groups (with an iHDS score of 10 or less and with a score of 10.5 and higher). As NPA is a time-consuming process, only a limited proportion of eligible patients could be referred due to time and fiscal constraints. An experienced neuropsychologist supervised the tests used in the NPA.
The test battery was adapted to the CHARTER study as much as possible to increase international validity. 11 The duration of the NPA is ∼2 h, and it contains 13 validated and commonly used tests. In brief, the NPA included the following tests (in this order): Mini-Mental State Examination, 15-word task (an episodic memory task that measures learning abilities and memory consolidation), Trail making task 12 (attention, executive functioning), Stroop color-word task 13 (attention, executive functioning), Fluency (language and/or semantic memory), Wechsler Adult Intelligence Scale-III 14 (visual-motor coordination, motor and processing speed), Rey Complex Figure Test 15 (visuoconstructive abilities, visual memory), Boston Naming Test 16 (word retrieval and language), WAIS-III (working memory, attention, and concentration), Wisconsin Card Sorting Test 17 (attention, executive functioning, and cognitive flexibility), Grooved Pegboard 18 (constructional praxis), Similarities (WAIS-III; verbal comprehension and reasoning), Block Design (WAIS-III, visuoconstruction). The scores from all tests were converted to z-scores. All z-scores were weighed and converted to a Global Deficit Score (GDS). A GDS above 0.5 was considered abnormal.
The sensitivity of the iHDS was assessed in a 2 × 2 table by the ability to accurately predict NPA outcome, as represented by a GDS above or below the cutoff. Medical history of all participants was assessed for treatment duration and comorbidities. Laboratory history was assessed for immunologic and viral parameters. CD4 (nadir) counts were grouped and GDS of these groups was compared using the Mann–Whitney test. The amount of comorbidities was scored and grouped based on dichotomous GDS (impaired vs. normal). Comorbidities that were nonchronic (e.g., a thromboembolic event or myocardial infarction) were only included if it occurred less than 6 months before inclusion. The proportion of patients without comorbidities was compared between Global Deficit (GD) categories using the Pearson chi-square test.
Results
Patient characteristics
Of a population of 1648 patients, we recruited a total of 400 patients for this study. Four patients were excluded during the study because the iHDS could not be performed optimally and eight patients withdrew from the study. Of the 388 patients, 127 (33%) reported to have problems in concentration, attention, and/or memory (Fig. 1). The mean age of all 388 patients was 48 years (±11), the majority of the patients were male (89%), the median CD count was 600 [interquartile range (IQR) = 450–780], and 326 (84%) had a viral load below 200 copies/mL (Table 1). As mentioned in the Methods section, proper NPA is a time-consuming endeavor, and therefore, we were only able to thoroughly investigate a subpopulation, rather than all 388 participants. During a period of 1 year, we were able to perform NPA in 74 of the initial 388 patients; five patients were excluded from the NPA analysis because the GDS could not reliably be calculated. A total of 69 patients were used for analysis. Characteristics of this group (Table 2) were comparable to the entire cohort, although patients were older (53 ± 11). Detailed characteristics comparing patients with and without complaints are listed in Table 3.
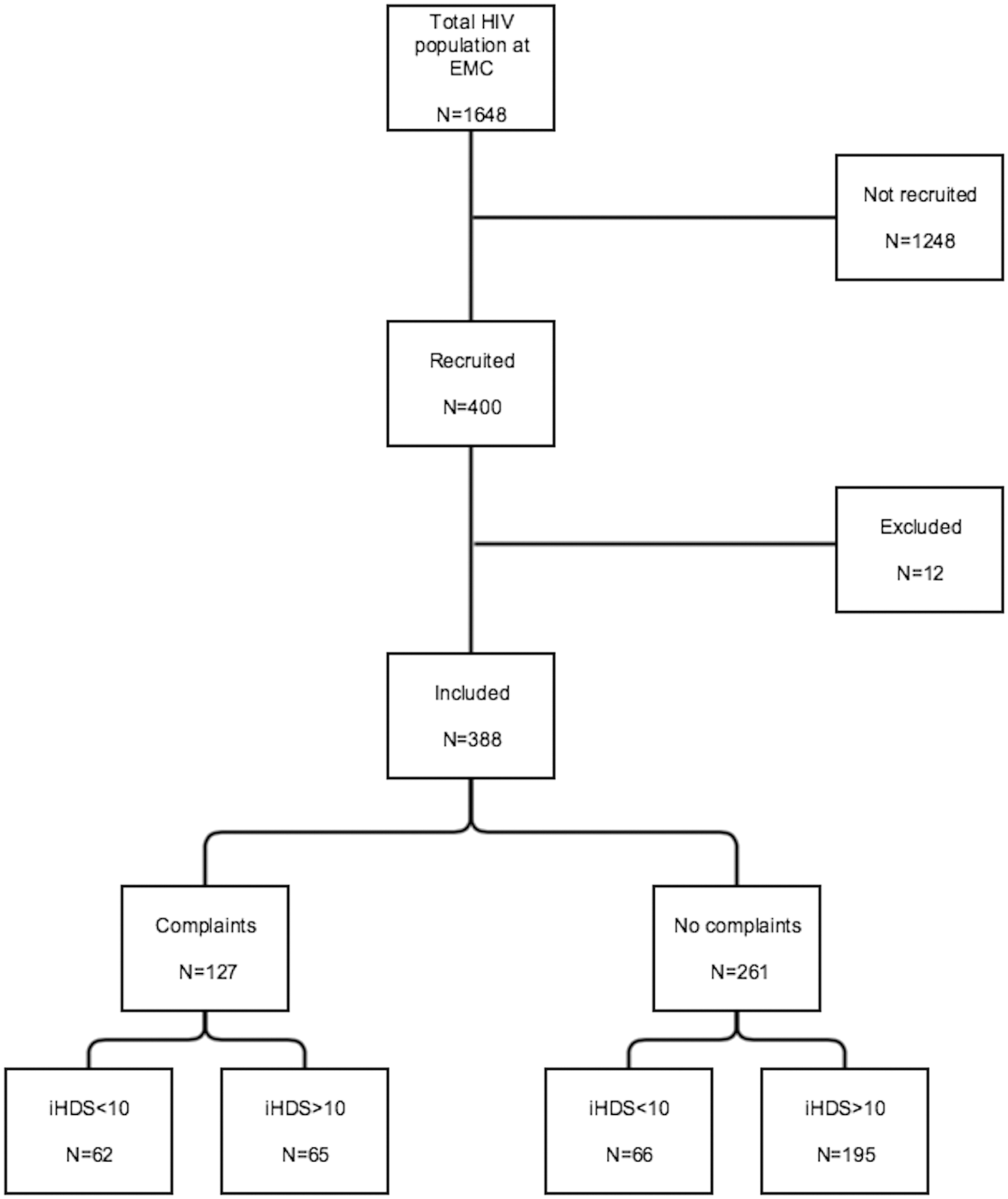
Flowchart of the TREVI study on neurocognitive impairment. Complaints were assessed by applying the three Simioni questions. iHDS, international HIV Dementia Scale.
General characteristics of the TREVI cohort. All 388 patients underwent neurocognitive screening.
IQR, interquartile range; SD, standard deviation.
General characteristics of TREVI cohort that underwent neuropsychological evaluation. Patients with and without complaints were included, both with normal and abnormal cognitive screening.
iHDS, international HIV Dementia Scale; IQR, interquartile range; SD, standard deviation.
General characteristics based on complaints expressed by patients. Complaints were assessed by asking the three Simioni questions.
iHDS, international HIV Dementia Scale; IQR, interquartile range; SD, standard deviation.
Predictive value of screening
Of the 69 patients who underwent NPA, 54 patients reported cognitive problems in daily functioning. A total of 23 of these 54 patients had an abnormal NPA. However, 5 of 15 patients without complaints also had an abnormal NPA. This results in a reasonable sensitivity (82%), but a low specificity (24%). Adding the iHDS greatly improved the specificity (73%) but at the expense of sensitivity (50%). The iHDS on its own correctly predicted an abnormal NPA result in 19 of 34 patients, but 9 of 35 patients with a normal iHDS still had an abnormal NPA (Table 4). The sensitivity of the iHDS alone was 68% and specificity 63%.
A contingency table assessing complaints and the results of the iHDS compared to the gold standard, neuropsychological evaluation. A GDS was calculated to determine which patients scored below average.
GDS, Global Deficit Score; iHDS, international HIV Dementia Scale.
Clinical correlates
Patients with an abnormal NPA had a significantly lower iHDS score (p = 0.009). Age, current CD4, viral load, and cART duration were not associated with abnormal NPA outcome (Table 5). The nadir CD4 counts of patients were grouped based on clinically relevant cutoff values (50, 200, 350, and 500). Patients with a CD4 nadir count <50 cells/m3 had a statistically lower GDS compared to patients with a CD4 nadir >50 cells/m3 (0.18 vs. 0.55; p = 0.01). No significant difference in GDS was detected in the groups with CD4 nadir count below 200 (p = 0.334), 350 (p = 0.802), or 500 (p = 0.780). In the group with abnormal NPA, a larger proportion had one or more comorbidities (Fig. 2), although not statistically significant. In comparison, 70% of patients in the normal NPA group had no comorbidities versus 61% in the abnormal NPA group (p = 0.276).
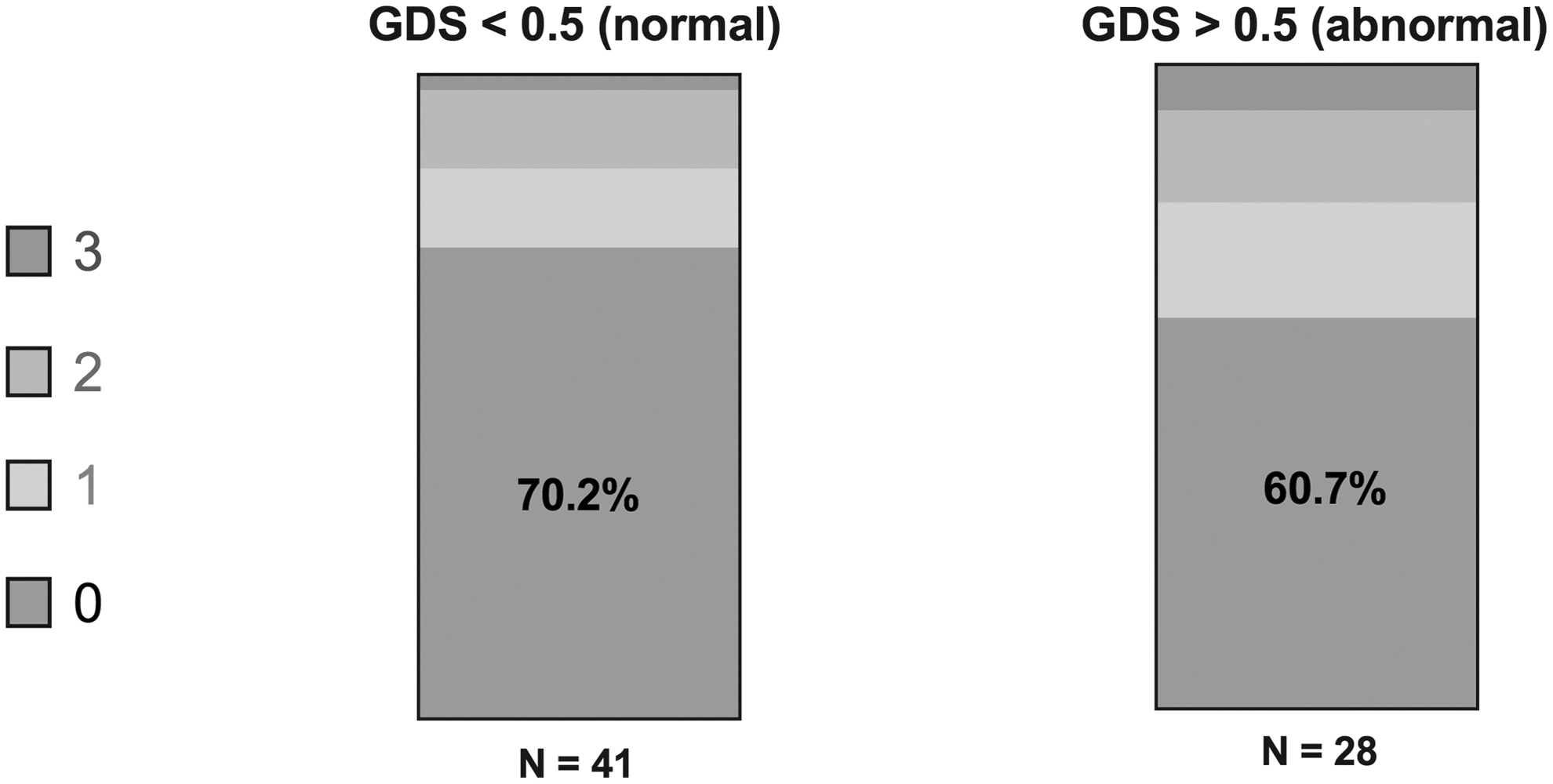
Distribution in number of comorbidities in patients with normal and abnormal NPA scores. 70.2% in the group with normal NPA results had no comorbidities versus 60.7% in the group with abnormal NPA results. GDS, Global Deficit Score; NPA, neuropsychological assessment.
Characteristics of patients as grouped based on the NPA score. The score of the international HIV Dementia Scale was lower in patients with abnormal NPA.
iHDS, international HIV Dementia Scale; IQR, interquartile range; SD, standard deviation.
Discussion
This study was designed to evaluate the use of the iHDS in a clinical setting and clinical factors associated with neurocognitive disorders. Current European guidelines stress the need to regularly screen for cognitive deficits in HIV-infected individuals. 10 The three Simioni questions should guide clinicians in determining whether the patient should be referred for extensive neuropsychological evaluation. Considering that NPA is a laborious exercise, it would be beneficial for both patient and clinician to have a screening test with a high specificity. We therefore investigated the use of the iHDS, one of the most widely used HIV-specific screening tools. A third of our study population was noted to have difficulties in concentration, attention, or memory. However, of the patients with complaints who underwent full neuropsychological investigation, 57% would prove to be unimpaired according to NPA results. By performing additional screening in patients who have complaints, the iHDS filters out false positives, but also results in a disappointing low sensitivity (50%). We concluded that current clinical practice to detect neurocognitive disorders in HIV-infected individuals is unsatisfactory. Considering the impact that neurocognitive deficits can have on an individual, more sensitive and specific screening tools are needed.
In our study, a low CD4 nadir seems to be associated with poorer neurocognitive functioning. In the CHARTER study, one of the largest cohort studies on HAND to date, CD4 nadir was also associated with poorer neurocognitive functioning. 11 This is comparable with results from other large cohort studies investigating HAND. 19 In addition, the CHARTER cohort demonstrated that a low CD4 nadir was also associated with a higher level of white matter damage and variability in subcortical volumes. 20 This might be explained by irreversible damage caused by factors such as opportunistic infections, chronic immune activation, or a history of HIV encephalitis. 21 We found no differences when applying higher (clinically relevant) cutoff scores, indicating that this effect occurs below a certain threshold. Preventing severe immunosuppression could protect HIV-infected individuals from cognitive deficits. Other mechanisms of neurological damage could include vascular damage and other existing comorbidities. We could not find a significantly higher degree of comorbidity in the group with cognitive deficits. It is also possible that direct viral cytotoxicity induces parenchymal damage. In vivo studies already demonstrated increased viral loads in the cerebral spinal compartment during the chronic phase of infection. 22 There have even been studies linking viral burden in the CNS to antemortem cognitive functioning. 23 Although the plasma viral load was undetectable in the majority of patients in our study, we cannot rule out the effect of cytotoxicity. We could not find any other clinical parameters that could help guide clinicians in determining which patients to screen.
The strength of this study is a clinical setup in a relatively uncontrolled environment, reflecting a realistic outpatient setting. Clinicians are often confronted with vague symptoms in chronically well-treated HIV-infected individuals. We implemented the application of current guidelines in a standardized way and identified the pitfalls in the evaluation of cognitive deficits. However, our study does have some limitations. First of all, it would have been optimal to perform NPA in all the included patients. However, we chose to perform NPA only in a subpopulation due to the extensiveness of this examination. Because we expected that patients without complaints and with an iHDS score above 10 would not fail the NPA, the groups with complaints or an abnormal iHDS score were larger. Our hypothesis is supported by the fact that all patients in the prior group passed the NPA. We only included Dutch and English-speaking individuals to minimize the effect that language can have during NPA. Cultural aspects can influence the perception of cognitive complaints and might affect CD4 nadir because immigrants have shown to present relatively late in the course of HIV infection. 24 Also, the proportion of HIV-infected individuals who express psychological symptoms is high 25 ; this could impact the prevalence of cognitive complaints found in our study. In addition, we only measured cross-sectionally and have no information on whether individuals with cognitive complaints progress in their symptoms.
This study demonstrates the limitations of brief cognitive evaluation and rapid screening tests such as the iHDS. Its intentional use is to identify those patients at risk for cognitive dysfunction. Based on our data, we would recommend caution when assessing a patient in a clinical setting. Ideally, all patients would have to be subjected to the gold standard of neurocognitive evaluation, that is, NPA. However, the authors realize that this consequently causes a burden to both patient and neuropsychologist.
In a chronically well-treated HIV population, the number of patients expressing cognitive complaints when asked is exceptionally high (33%). We used the iHDS, an internationally valid screening tool, to screen for cognitive deficits. We found a sensitivity of 68% for the iHDS, which decreased to 50% when applying this as an addition to the Simioni questions. The sole presence of complaints as indication of cognitive deficits resulted in an unacceptably low specificity (24%). The presence of a CD4 nadir below 50 cells/m3 was associated with a significantly lower GDS. We found no other clinical correlates associated with an abnormal NPA. We detected slightly more (nonconfounding) comorbidities in the group with an abnormal NPA but this was not significant. There is a need to improve neurocognitive screening and selection tools.
Footnotes
Acknowledgments
L.W.J.v.d.D. recruited the patients, performed the analysis, and wrote the article; M.N.W. recruited the patients and contributed in writing the article; L.C.J. and M.V. performed the NPA and contributed in writing the article; K.R.R. assisted in the interpretation of data and writing the article; and K.S.A. and E.C.M.v.G. assisted in the interpretation of data and writing the article. The authors also acknowledge the important contributions of T. Langerak, L. Vriend, D. van der Gaag, and the specialists and personnel at the outpatient clinic of Infectious Diseases at the Erasmus Medical Center, and the Janssen unrestricted educational grant.
Author Disclosure Statement
No conflicting financial interests exist.