
Abstract
Youth living with HIV (YLWH) are less likely than older adults to achieve and sustain viral suppression. While treatment guidelines recommend decreased viral load (VL) monitoring in individuals with well-controlled HIV, the appropriateness of this strategy for adolescents is unknown. We conducted a retrospective cohort study to describe longitudinal viral suppression and identify incidence of, and risk factors for, virologic failure among YLWH at a US adolescent HIV clinic from 2002 to 2015. We utilized Cox proportional hazards modeling to compare hazard ratios (HRs) for virologic failure stratified by baseline characteristics. Study participants (n = 365) were predominately African American (87%) and cisgender men and transgender women who have sex with men (80%) and the majority (79%) entered care from 2002 to 2012. Of antiretroviral therapy (ART)-treated participants (n = 201), 88% achieved viral suppression, with 29% subsequently developing virologic failure at a median 12.0 months [interquartile range (IQR) 6.9–22.4] after suppression. The cohort incidence rate of virologic failure was 200 (confidence interval [95% CI]: 151–264) per 1000 person years (PY), with a rate after ≥2 years sustained suppression of 113 (95% CI: 57–227) per 1000 PY. After adjusting for time to ART initiation, initial regimen class, and year of cohort entry, cisgender women had increased hazards of virologic failure (HR 3.2 95% CI: 1.3–7.9, p = 0.01). In conclusion, youth remained at high risk of virologic failure throughout their treatment course, with higher hazards of virologic failure among cisgender women compared with other youth. Maintaining frequent VL monitoring in YLWH may be warranted, even after prolonged viral suppression.
Introduction
Y
Recent changes in the Department of Health and Human Services (DHHS) HIV treatment guidelines recommend reducing VL monitoring for adolescents and adults with sustained viral suppression for ≥2 years. 14 However, the appropriateness of this approach for YLWH, who may be at a higher risk of virologic failure during their developmental trajectory toward adulthood, is unknown. A recent meta-analysis of viral suppression in YLWH identified few studies reporting longitudinal suppression rates in adolescents and young adults. 15 The limited existing data on longitudinal patterns of viral suppression demonstrate that younger individuals, even after achieving initial suppression, are more likely than older adults to experience virologic failure. 4,5,15 Each episode of failure in youth represents a period of potential disease progression and increased transmission risk. It is essential, therefore, to understand the risk of virologic failure after sustained suppression before considering less frequent virologic monitoring strategies in YLWH.
The study objectives were to: (1) describe patterns of viral suppression among a cohort of youth with behaviorally acquired HIV, (2) determine the incidence of virologic failure overall and after 2 years of sustained suppression and, (3) identify risk factors associated with virologic failure in YLWH initially achieving suppression.
Materials and Methods
Design
We conducted a retrospective cohort study of YLWH with behaviorally acquired HIV initiating care between January 2002 and June 2015 at a US-based adolescent HIV clinic.
Subjects and setting
The Adolescent Initiative Clinic at the Children's Hospital of Philadelphia (CHOP) provides HIV care to YLWH. Treatment is provided by a multidisciplinary care team encompassing medical management, social work support, and behavioral health. All patients receive intensive case management and adherence counseling. Patients transition to adult care at age 24. Participants were included if they were aged 12–24 at their initial visit, ART naive, and acquired HIV through sexual activity or injection drug use. Approval was received from the CHOP Institutional Review Board.
Measures
Data were abstracted from a research registry containing all clinical and laboratory visits during the study period. For our outcome measures, we defined viral suppression as plasma HIV RNA <200 copies/mL after ART initiation; sustained suppression as ≥2 years of consistent virologic suppression in those subjects with ≥3 VL measures in the 2 years after suppression; and virologic failure as plasma HIV RNA ≥200 copies/mL twice consecutively or >1000 copies/mL once after initial suppression. 16 Subjects were followed until the first episode of virologic failure or transition of care, lost to follow-up, or end of the study period. Lost to follow-up was defined by review of each subject's record at the end of the study period (June 30, 2015). Subjects were defined as lost to follow-up if they were still eligible to seek treatment at the study site, but had dropped out of care for >6 months (no contact by phone, email, or in-person visits documented in the electronic medical record).
For our exposure covariates, sex was defined as sex assigned at birth. Race was defined by self-report. Gender was defined by self-reported gender at the final visit. In keeping with previous longitudinal studies of sexual and gender minority youth, we used final visit data for the gender covariate to account for developmental trajectories in which youth did not report transgender status at the baseline visit, but transitioned gender later in the study period. 17,18 Gender was categorized as cisgender male (male sex assigned at birth with male gender identity), cisgender female (female sex assigned at birth with female gender identity), and transgender female (male sex assigned at birth with female gender identity). No subject identified as a transgender male during the study period.
Psychosocial variables were obtained at the baseline visit through clinician or social worker interview. Baseline mental health diagnoses were determined by a self-reported or chart-documented history of mental illness at the baseline visit or by clinical diagnosis by a medical provider (MD, nurse practitioner or social worker) at the baseline visit. Baseline substance use (tobacco, alcohol, marijuana) covariates were dichotomized to use or no use. Insurance status at each visit was dichotomized as insured (public or private) versus uninsured (no insurance or Ryan White pharmacy-only coverage). Baseline housing status was dichotomized as secure (owning/renting home or apartment, living with family, or living in school housing) versus insecure (staying with friends, transient housing, group home or foster care, incarceration, or unstable housing).
ART regimen class was categorized as protease inhibitor (PI), non-nucleoside reverse transcriptase inhibitor (NNRTI), or integrase strand transfer inhibitor (INSTI)-based and ART treatment status was recorded for each visit. We dichotomized participants into those who entered the cohort before or during 2012 versus after to assess for the potential impact of the introduction of universal ART recommendations by DHHS in 2012.
Statistical analyses
To delineate the background population of the study, baseline characteristics of the cohort stratified by ART treatment status were compared by chi-squared and Wilcoxon rank-sum testing. Survival analysis was used to examine the incidence rate of virologic failure within two subsets of participants: (1) those who achieved viral suppression and had ≥1 VL measurement after suppression, and (2) those participants who started ART before 2013 and achieved ≥2 years sustained suppression. Participants were followed from the first date of viral suppression until the date of first virologic failure or transition of care, lost to follow-up, or end of the study period. Kaplan–Meier graphs were constructed to examine the time to virologic failure among those participants achieving initial virologic suppression, and compared based on baseline characteristics through log-rank testing. Cox proportional hazard models compared rates of virologic failure stratified by gender, race, age, time from diagnosis to ART initiation (measured as a continuous variable in months), ART regimen class, substance abuse, depression, housing, and insurance status. We utilized a stepwise model inclusion wherein covariates with a p-value ≤0.1 were included in the final multivariable model. We set statistical significance for the final model at p < 0.05. The proportional hazards assumption for the final multivariable model and the individual model covariates were assessed using Schoenfeld and scaled Schoenfeld residuals.
For binary covariates with missing data (substance use covariates, housing status and presence of baseline mental illness), we ran sensitivity analyses, where missing values were imputed as absence of the risk factor (i.e., missing smoking was coded as nonsmoker) in the regression models. For categorical covariates with missing data (race and baseline ART regimen), these were analyzed with a complete case analysis approach in the univariate and multivariable models. All analyses were completed with Stata 14.0 (StataCorp LP, 2015, College Station, TX).
Results
The cohort was comprised of 365 behaviorally HIV-infected youth who were followed for a median of 2.1 years [interquartile range (IQR) 0.8–4.1]. Participants were predominately African American (87%), cisgender males (83%), and acquired HIV through male–male sexual transmission (80%). The baseline demographic characteristics of the cohort are displayed in Table 1. At the end of the study period, 28% (n = 103) of participants remained in care at the study site, 39% (n = 143) had transitioned to adult HIV care, 12% (n = 44) relocated or transitioned to another regional adolescent HIV provider, 19% (n = 68) were lost to follow-up, and 2% (n = 7) died.
Variables obtained at subject engagement in care (first clinic visit).
Bold test in table indicates statistical significance p < 0.05.
Interquartile range.
Sample sizes for variables with missing data noted in characteristic column.
ART, antiretroviral therapy.
ART was initiated in 55% (n = 201) of participants, at a median age of 20 years (IQR 18–22). The median time from HIV diagnosis to ART initiation was 9.8 months (IQR 5.0–23.7), and participants were followed for a median of 21.4 months (IQR 7.8–38.4 months) after ART initiation. There was a significant decrease in time between diagnosis and ART initiation for those who enrolled in the cohort after 2012 (12.5 months vs. 4.9 to ART, p < 0.001), although there was no difference in the proportions of participants starting ART between the pre- and post-universal guidelines period. Compared with non-ART-treated participants, those who initiated ART were younger at diagnosis, had lower baseline CD4+ T lymphocyte counts, lower rates of tobacco and marijuana use, and higher VLs (Table 1). There were no significant differences between the two groups at the baseline visit with respect to race, sex, gender, housing, insurance, alcohol use, or mental illness. The initial regimen was PI-based in 39%, NNRTI-based in 38%, and INSTI-based in 21%, with 1% of participants starting triple-class regimens.
Among ART-treated participants with ≥1 VL measurement after starting ART (n = 196), 88% achieved viral suppression on their first ART regimen with a median time to suppression of 2.5 months (IQR 1.3–4.3). Of these participants, 29% (n = 50) developed virologic failure at a median of 11.6 months (IQR 6.9–17.6) after initial suppression.
The survival analysis sample examining time to virologic failure included 154 participants who achieved viral suppression and had ≥1 subsequent VL measurement. These participants contributed 926 visits and 250 person years (PY) of follow-up time. The baseline demographic characteristics of the sample are displayed in Table 2. The incidence rate of virologic failure in this cohort was 200 per 1000 PY (confidence interval [95% CI]: 151–264). The cohort Kaplan–Meier survivor curve for time to virologic failure is displayed in Fig. 1. In log-rank testing, there was a statistically significant difference in virologic failure-free survival for cisgender females compared with cisgender males (Fig. 2, log-rank p < 0.001).
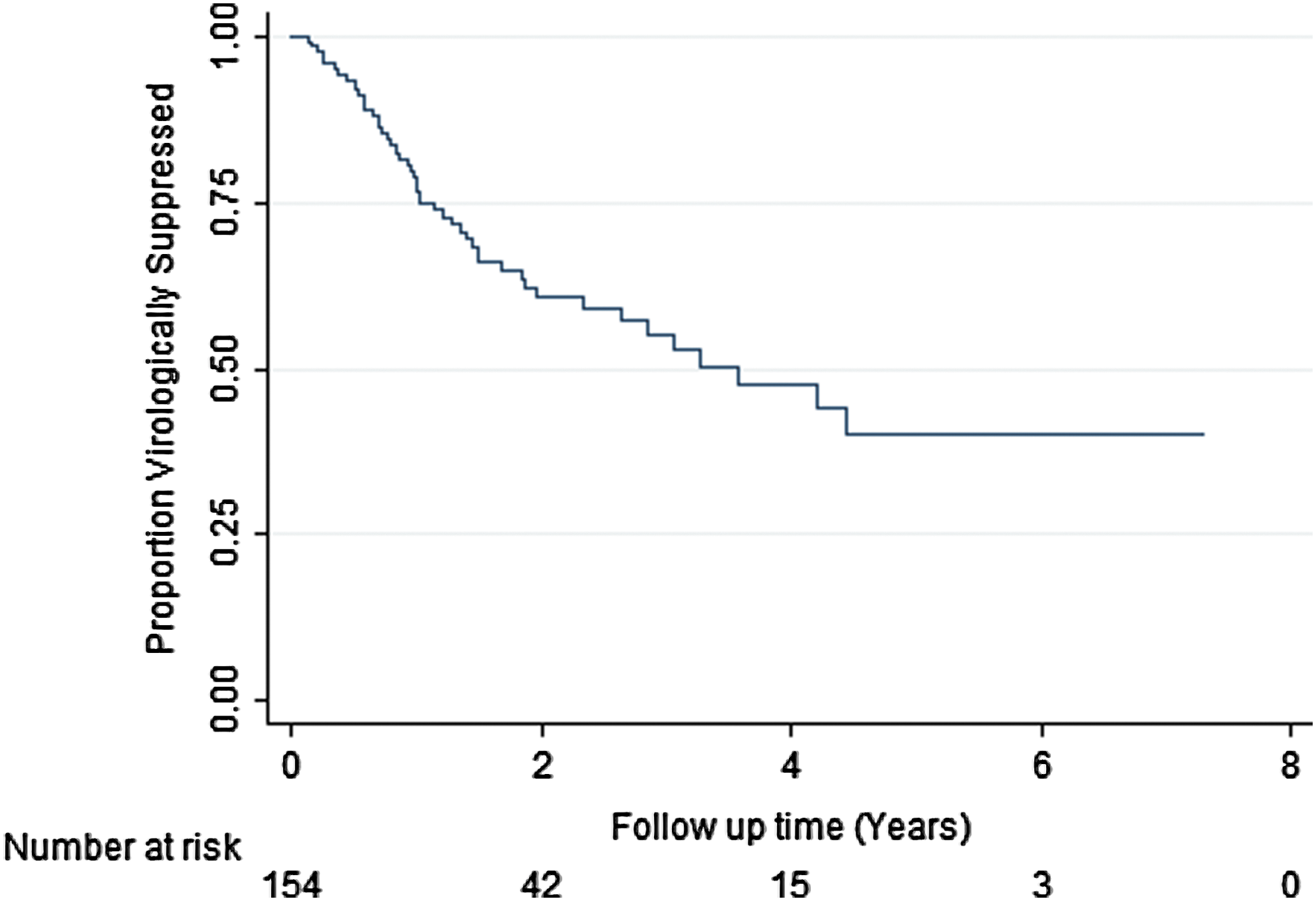
Kaplan–Meier survival estimate of virologic failure-free survival among HIV+ youth achieving virologic suppression (n = 154).
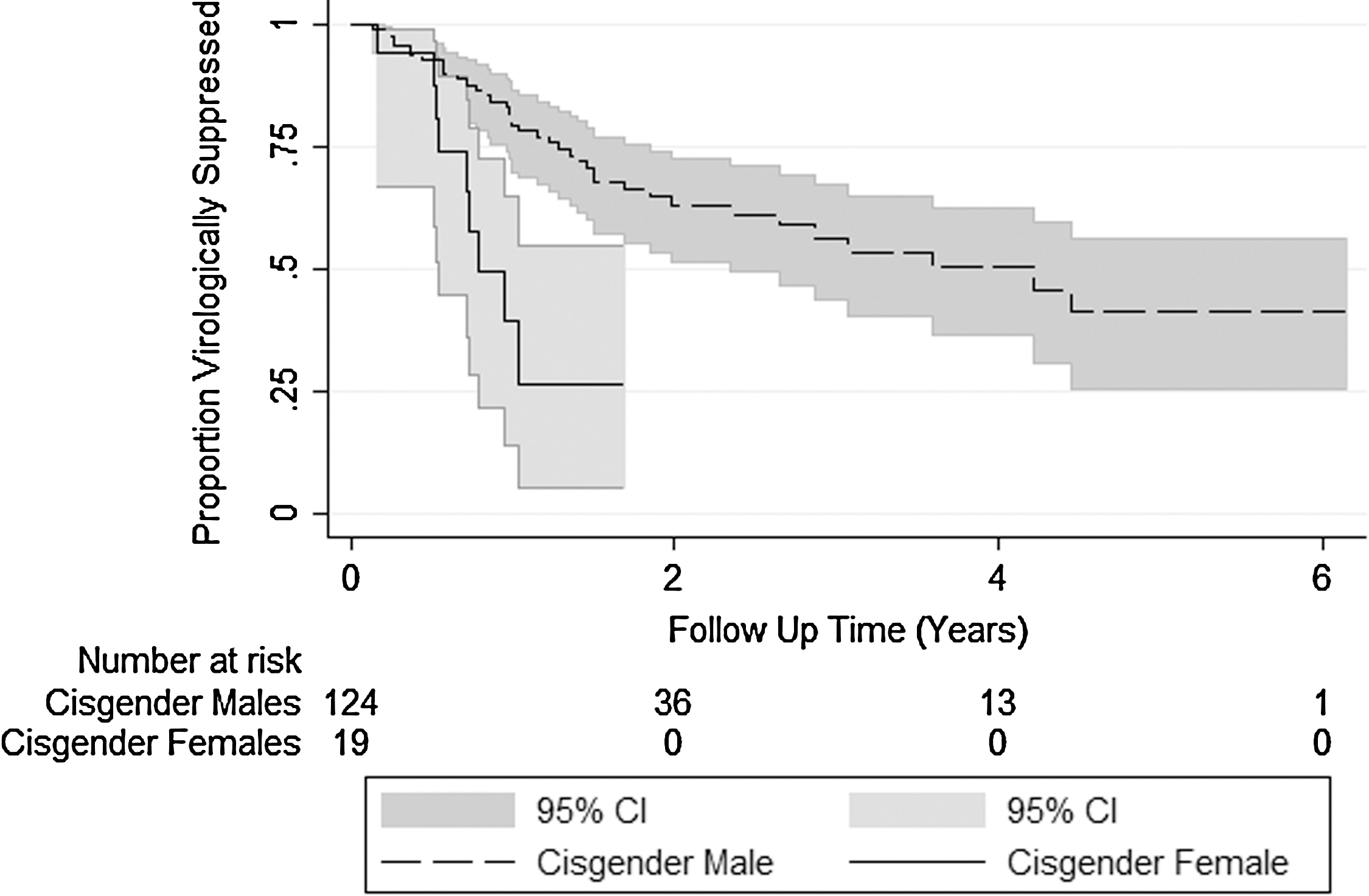
Gender-stratified virologic failure-free survival among HIV+ youth achieving virologic suppression (n = 143).
Sample sizes for variables with missing dates noted in characteristic column.
ART, antiretroviral therapy; INSTI, integrase strand transfer inhibitor; IQR, interquartile range; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
In the univariate Cox proportional hazard regression analyses (Table 3), cisgender females had a nearly fourfold increase in hazards of virologic failure [hazard ratio (HR) 3.9, 95% CI: 1.8–8.6, p = 0.001] compared with cisgender males. Compared with starting a PI-based regimen, ART initiation with an NNRTI-based regimen was associated with a decreased hazard rate of virologic failure (HR 0.5, 95% CI: 0.3–0.9, p = 0.03), whereas there was no statistically significant difference in HRs in those starting INSTI-based regimens (HR 0.3, 95% CI: 0.1–1.2 p = 0.09). There were no statistically significant associations between hazards of virologic failure and age, race, insurance status, housing, substance use, mental illness, or cohort entry after 2012. In the sensitivity analyses, where missing values of the binary covariates (substance use covariates and presence of baseline mental illness) were coded as absence of the risk factor, there was no change in the patterns of association with time to virologic failure. The final multivariable model adjusted for initial ART regimen class, time from HIV diagnosis to ART initiation, and cohort entry after 2012. Adjusting for model covariates had minimal impact on the increased hazards of virologic failure in cisgender women (HR 3.2 95% CI: 1.3–7.9 p = 0.01, see Table 3).
Bolded values reached statistical significance.
Final multivariable model adjusted for gender, initial ART regimen, time from HIV diagnosis to ART initiation, and entry in care after 2012.
ART, antiretroviral therapy; CI, confidence interval; INSTI, integrase strand transfer inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
The second survival analysis sample consisted of those participants who had achieved sustained virologic suppression (n = 41, or 48% of all participants with 2 years of follow-up time after ART initiation). Participants in the sustained suppression cohort were predominately African American (90%) men (85%) and transgender women (15%), 19% of whom developed subsequent virologic failure. The incidence rate of virologic failure after ≥2 years of sustained suppression was 113 per 1000 PY (95% CI: 57–227).
Discussion
In this retrospective cohort study, ART-treated youth living with behaviorally acquired HIV remained at high risk of virologic failure throughout their time in care, with an incidence rate of virologic failure of 20% per year, further reinforcing the dynamic nature of adherence in this vulnerable population. These data demonstrate the limits of treatment as prevention as a sole strategy of containing the youth HIV epidemic, and stress the need for integrated strategies such as increasing adherence support for YLWH and increasing access to HIV pre-exposure prophylaxis for HIV-negative youth. These data also suggest caution in reducing VL monitoring frequency among YLWH, even after prolonged suppression. After 2 years of consistent viral suppression, the incidence rate of virologic failure decreased to 113 per 1000 PY. While we report a lower incidence of virologic failure in those achieving sustained suppression than in the general cohort, a failure rate of >10% per year, with the upper bounds of our CI suggesting a rate as high as 23% per year, is arguably clinically significant in light of the increased potential for HIV transmission in adolescents and young adults. 19 To develop optimal virologic monitoring strategies for this vulnerable population, robust studies are needed to identify longitudinal trends in, and factors that predict, virologic failure.
Cisgender young women in the cohort had markedly increased hazard rates of virologic failure compared with cisgender males. Prior studies of the US adult HIV care continuum have found mixed results with respect to suppression rates in cisgender women living with HIV compared with cisgender men. 20 –22 However, these studies have not accounted for effect modification by age in the relationship between sex and viral suppression, and our data suggest that younger women may be uniquely vulnerable to poor outcomes. In their recent study of nearly 1900 YLWH, Kahana et al. also identified that cisgender young women were less likely to be suppressed than cisgender young men. 23 It is possible that sex-based disparities in viral suppression may be accounted for by lapses in care related to pregnancy and delivery in young cisgender women at the height of their reproductive years. 24 Future research is needed to determine the mechanisms for gender-based disparities in virologic failure, and the combined effects of age, gender, and reproductive status on virologic failure.
Our study is subject to limitations, including our sample size, which limited our ability to detect small differences in VL outcomes stratified by subject characteristics. This may account for our failure to find risk factors for virologic failure other than gender. We were unable to account for pregnancy status in the data registry, which is a potential source of the gender disparities in virologic failure in our cohort. As our data were abstracted from a retrospective registry of clinical visits, rather than a prospective research cohort, we were limited by missing values of baseline psychosocial covariates. However, we conducted sensitivity analyses of data, which demonstrated that our findings were robust to the conservative assumption that missing values denoted absence of the risk factor. The overall rate of ART prescription in the cohort was relatively low (55%); however, our rate of ART initiation is consistent with a substantial body of literature demonstrating lower rates of ART prescription in youth compared with adults, 25 –27 as well as recent data from youth linked to care at Adolescent Treatment Network sites reporting a 59% rate of current ART use. 23 As 80% of our cohort entered care before universal ART recommendations in 2012, our ART prescription rate is likely affected by CD4-based decision making about treatment initiation. Future studies should focus on whether disparities between adolescent and adult treatment rates have decreased in the post-universal treatment era. Lastly, our data represent observations from a single clinic and thus may not be generalizable to the larger US population of HIV-infected AYA. However, our patient population consisted predominately of African American men and transgender women who have sex with men, a demographic with one of the highest HIV incidence rates in the United States and, therefore, may be representative of the evolving face of the youth HIV epidemic.
In conclusion, we identified high virologic failure rates among youth living with behaviorally acquired HIV, with clinically significant failure rates occurring even after ≥2 years of sustained suppression. Our data suggest caution in applying the DHHS recommendation to reduce VL monitoring in adolescents and young adults with well-controlled HIV, as this strategy may miss a significant proportion of episodes of failure. Maintaining quarterly VL monitoring may allow for early recognition of virologic failure, which provides opportunities for interventions to improve adherence, and prevent resistance and secondary HIV transmission. In addition, future research should emphasize the development and evaluation of youth-focused interventions to improve HIV-related care outcomes, including designing adolescent-friendly clinical services, 28 and developing technology-based interventions, such as text messaging and mobile applications, to support ART adherence. 29 –31 Importantly, if we are to truly realize the benefits of treatment as prevention, given the dynamic nature of adherence demonstrated by our data, new interventions should also target prevention of virologic failure among virologically suppressed YLWH.
Footnotes
Acknowledgments
The authors wish to thank the research team for their valuable contributions: Paul Nguyen, Papia Paul, Avital Warburg, David Yusavitz, Derek Standlee, Isabella Lopez, Dr. Jennifer Culhane, Leny Mathew, and Felipe Garcia-Espana.
Funding
This research was directly supported by grants from F32 MH111341 (PI: S.M.W.), K23 MH102128 (PI: N.D.), and K23 MH095669 (PI: E.L.). This research was also made possible through core services and support from the Penn Center for AIDS Research (CFAR), an NIH-funded program (P30 AI 045008).
Author Disclosure Statement
No competing financial interests exist.