
Abstract
In China, rural areas are a weak link of HIV/AIDS prevention and control. From September 2011, an innovative “county-township-village” allied intervention was implemented in Longzhou County, Guangxi, which assigned the tasks of HIV/AIDS prevention and control to the county Centers for Disease Control and Prevention (CDC), township hospitals, and village clinics, respectively, instead of traditional intervention in which the county CDC undertook the entire work. A 6-year consecutive cross-sectional survey, including 3-year traditional intervention (2009–2011) and 3-year innovative intervention (2012–2014), was conducted to evaluate the effects of the new intervention. Compared to traditional intervention, the innovative intervention achieved positive effects in decreasing risky behaviors. Among female sex workers, condom use rate in the last month increased from 72.06% to 96.82% (p < 0.01). Among drug users, having commercial sex rate in the last year reduced from 17.20% to 5.94% and condom use rate increased from 14.06% to 76.09% (p < 0.01). The risk ratio of HIV infection during innovative intervention was 0.631 (95% confidence interval 0.549–0.726) compared with traditional one. Cost-effectiveness analysis indicates that innovative intervention restores each disability-adjusted life year costing an average of $124.26. Taken together, Longzhou's innovative intervention has achieved good effects on HIV/AIDS prevention and control and provides a good reference for rural China.
Introduction
I
China is an agricultural country where two-thirds of the people still depend on farming. In rural areas, the economic level is relatively low and healthcare is still imperfect. Rural populations are vulnerable to HIV infection. An important reason is that rural populations lack HIV-/AIDS-related knowledge and self-protection awareness, which also leads to late entry to HIV/AIDS care. 3 –6 The vast rural areas are still the weak link of the current AIDS prevention and control in China, which is a critical concern and needs more HIV/AIDS prevention efforts.
Currently, HIV/AIDS prevention efforts are mainly carried out by limited number of people from the Centers for Disease Control and Prevention (CDC), including national, provincial, cities', and counties' CDCs, which always conduct short-term, small-scale, and superficial activities. 7 The efforts proved to be effective in urban areas. 8 –10 However, the efforts seem to be less effective in rural areas.
Guangxi, a southwestern province in China, has the second highest number of reported HIV/AIDS infections in China, accounting for ∼10% of total national reported HIV cases. 11 From 2009 to 2011, among new HIV cases reported in Guangxi, 65.7% stemmed from the rural populations, 12 indicating that HIV prevention in rural Guangxi is still a big challenge to local government and healthy workers.
Community-based interventions are increasingly being advocated for HIV prevention. A number of studies have shown that community-based interventions are effective in improving knowledge, attitudes, and behavior (KAB) outcomes, as evidenced by increased knowledge scores for HIV/AIDS, protected sexual encounters, condom use, and decreased frequency of sexual intercourse. 13 –16 In rural China, the basic community unit is village. According to the principle of community-based interventions, an innovative village-level intervention focusing on the level of village, namely “county-township-village” allied intervention, was designed and implemented in Longzhou county since September, 2011.
Longzhou, a subtropical rural county in southern Guangxi, has 12 townships and 123 villages. Due to bordering to Vietnam, Longzhou county's residents could communicate with Vietnamese conveniently and frequently, which make the region become a hot spot for cross-border drug trafficking and also HIV/AIDS spread. The first case of AIDS in Longzhou county was reported in 1997, and then the epidemic continued to spread. 17 By the end of 2011, the number of HIV/AIDS patients in Longzhou reached 1070. The HIV prevalence rate was ∼0.41% in 2011, which was over seven times higher than contemporaneous national rate (0.058%) and ranked the fifth among all cities and counties in Guangxi. In Longzhou county, most of reported HIV/AIDS cases were related to two high risky populations, female sex workers (FSWs) and drug users (DUs).
In this study, we evaluated the effects of the innovative village-level intervention through a 6-year survey and surveillance, focusing on behavior changes among two high risky populations, FSWs and DUs, and the change of local HIV new cases (newly reported HIV/AIDS cases each year). We also analyzed the cost-effectiveness of the innovative village-level intervention.
Methods
Study site and populations
The survey and HIV/AIDS surveillance were conducted in Longzhou county, Guangxi. Under the guidance of Guangxi Health and Family Planning Commission, a village-level innovative intervention, namely “county-township-village” allied intervention, has been jointly designed and implemented by Guangxi Medical University and Longzhou county CDC since September, 2011.
Two populations, FSWs and DUs, were selected for this survey; due to their information about demographic characteristics, HIV-/AIDS-related KAB is complete and available from databases of local CDC. Inclusion criteria were as follows: (1) having a fixed location in Longzhou county; (2) normal language (either mandarin or the local dialect); (3) willing to participate in this study; and (4) being recorded in CDC databases and their information about demographic characteristics being complete.
The FSWs and DUs who received the innovative village-level intervention during 2012–2014 were defined as the innovative intervention group. Those who received the traditional intervention during 2009–2011 were defined as the traditional intervention group. All participants provided written informed consent form. The study was approved by the Human Research Ethics Committee of Guangxi Medical University.
Traditional and village-level interventions
In traditional intervention, the county CDC undertook the entire work for the whole county, including epidemiological investigation, HIV Voluntary Counseling and Testing (VCT), methadone treatment, condom promotion program, needle exchange program, and public education campaigns (such as posters, distributing education brochures, and various campaigns on world AIDS Day).
The innovative village-level intervention was designed at the village level. In this model, the tasks of AIDS/HIV prevention and control were assigned reasonably to the county CDC, township hospitals, and village clinics, respectively. As shown in Fig. 1, the county CDC transformed its role to a leader, a guider, and a supervisor. Except its routine intervention work on downtown residents, the county CDC was in charge of innovative village-level intervention organization, provided training for the township hospitals and village clinics, and organized meetings quarterly to regard feedback and share work experiences. The county CDC was also responsible for improving the equipments such as refrigerators and centrifuges, and distributing materials such as the education brochures, posters, and condoms to township hospitals and village clinics.
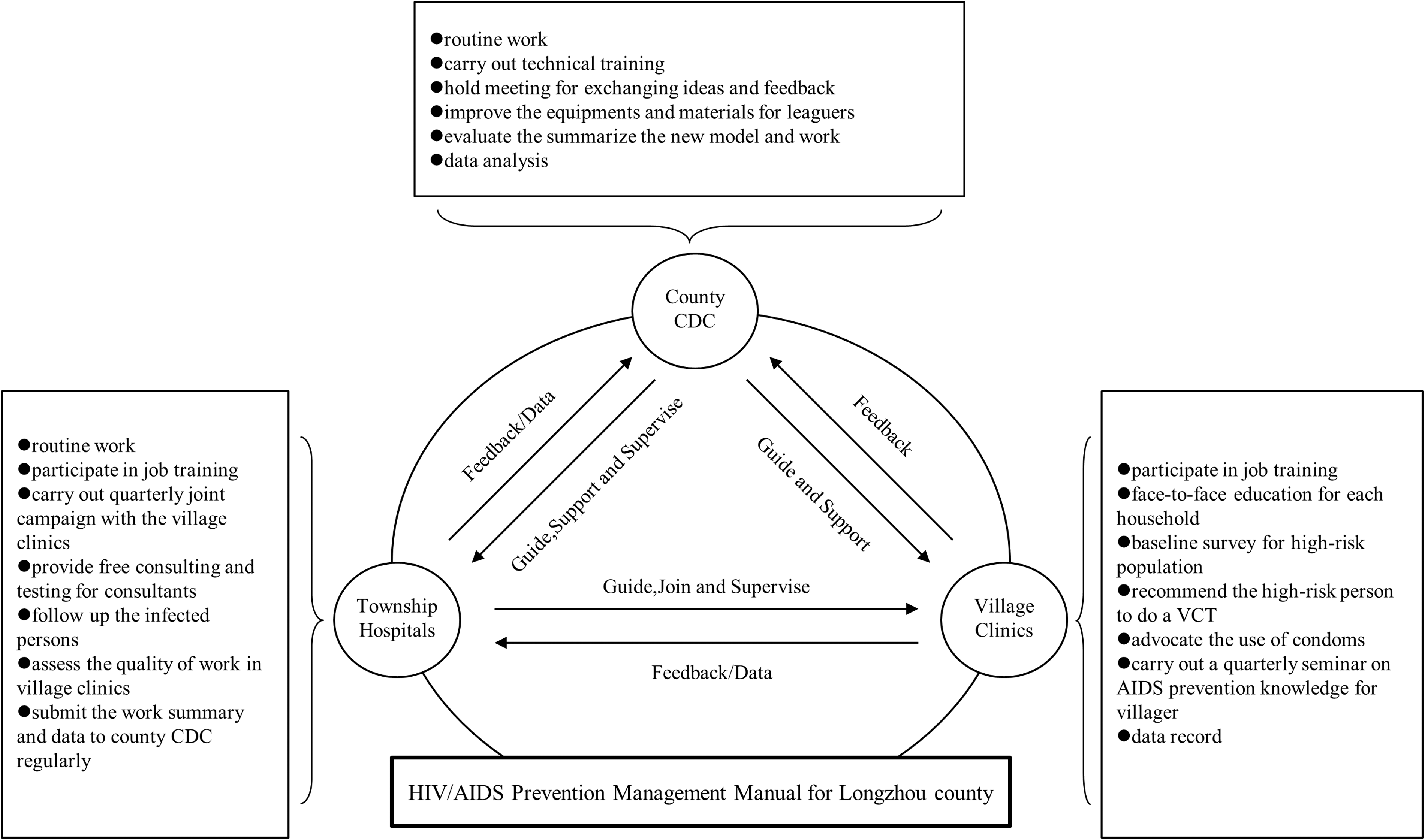
Diagram of the design of “county-township-village” allied intervention.
In the innovative village-level intervention, the role of the township hospitals is a kind of “mediator.” The township hospitals should carry out their routine work on township residents; on the other hand, they should organize village clinics to participate in training and quarterly joint HIV/AIDS education campaigns organized by county CDC. The township hospitals also acted as a supervisor for the village clinics. They needed to assess the quality of work in village clinics every half a year.
In the innovative village-level intervention, the routine work on village residents is carried out by village clinics. They needed to carry out household-based face-to-face HIV-/AIDS-related education for all villagers and finish baseline surveys for high-risk populations such as FSWs and DUs; they were in charge of free condom program and offered free condoms for all villagers. The village clinics needed to carry out HIV/AIDS education campaigns quarterly to popularize HIV/AIDS prevention knowledge and recommend the high-risky persons to do a VCT in township hospitals or county CDC.
Data collection
The questionnaire designed by China CDC 18 contains four sections: sociodemographic characteristics, the knowledge of HIV/AIDS, drug use behaviors, and sexual behaviors. The measure for HIV/AIDS basic knowledge and awareness was determined by correct responses to eight questions about HIV/AIDS. For example, “Can you judge an HIV-infected person only from his/her appearance?,” “Can mosquito bites bring HIV infection?,” “Can blood transfusion bring HIV infection?,” “Can having dinner together with HIV-infected people bring HIV infection?,” and “Can condom use reduce the spread of HIV infection?.” Being “aware” was defined as replying correctly to six or more questions. 18
Data of FSWs and DUs, including their information about demographic characteristics, HIV-/AIDS-related KAB, were collected from 2009 to 2014. Moreover, through the local CDC data system, we collected HIV annual new cases of Longzhou county during 2003–2014 to estimate the impact of innovative village-level intervention. Further, we collected financial statements and financial documents from Health Bureau of Longzhou county between January 1, 2009, and December 31, 2014, which contained governmental expenditures on local HIV/AIDS prevention and control, to analyze the cost-effectiveness of the innovative village-level intervention.
Data analysis
Chi-square analysis or Fisher test, when appropriate, was used to assess whether the demographic variables, including sex, age, education, and marital status, HIV/AIDS knowledge, and high-risk behaviors were different or significantly changed before and after the village-level intervention implementation. Mantel-Haenszel stratified analysis was used to calculate whether the different demographic variables affect the changes in HIV/AIDS knowledge and high-risk behaviors. Cochran-Armitage trend test was used to evaluate the trend of high-risk behaviors.
The Gray GM (1,1) Forecast Model was established to predict HIV new cases. Based on gray system theory, the GM model was established by Deng et al. 19 and developed to GM (1,1) model by other reseachers, 20,21 which directly deals original data and searches the intrinsic regularity of data. It is particularly suitable for analyzing the data with incomplete information or small sample. The GM (1,1) model has relatively high reliability and efficiency and its forecasting results are obtained without using any assumptions.
The health economics evaluation on innovative intervention was analyzed as follows: (1) averted infection numbers = expected incidence − actual incidence, the expected HIV incidence was predicted from the model fitted by 2003–2011 annual new cases through the Gray GM (1,1) model; (2) cost of each HIV infection case averted = total funding/the numbers of infection averted; (3) cost-effectiveness analysis (CEA) = cost/deaths averted and discounted years of life lost averted [reduced morbidity, deaths averted, and disability-adjusted life year (DALY) averted].
A two-sided p-value of 0.05 or less was regarded as statistically significant. Chi-square test and Mantel-Haenszel stratified analysis were carried out by SPSS version 16.0. Cochran-Armitage trend test and Gray GM (1,1) Forecast Model were carried out by using SAS version 9.3.
Results
Demographic characteristics
In this study, we totally enrolled 3365 FSW and DU subjects, including 880 FSWs and 819 DUs during traditional intervention, as well as 813 FSWs and 853 DUs during innovative intervention. Among them, 866 FSWs (98.4%) and 744 DUs (90.8%) during traditional intervention, as well as 785 FSWs (96.6%) and 775 DUs (90.9%) during innovative intervention, agreed to participate in this study and completed the survey. Totally 97.5% FSWs and 90.8% DUs agreed to participate in this study.
Demographic characteristics of FSWs
Table 1 shows the demographic characteristics of FSWs. The average age of FSWs who accepted traditional or innovative intervention was 35.7 ± 7.1 or 38.1 ± 7.6 years, respectively. In both FSW groups, the number of Han ethnic group was higher than the total number of other ethnic groups. Most of FSWs only had education level of junior middle school or lower. Almost all FSWs traded in street-based places, including barber shops and streetwalkers. More than 80% of FSWs had a regular sexual partner(s). Between the two intervention groups, there is no significant difference (p > 0.05) in age, education level, the grade of venues, and regular sexual partner among FSWs. However, significant difference (p < 0.05) existed in ethnic group and household registry between the two FSW groups.
Calculated by Fisher test.
Demographic characteristics of DUs
As shown in Table 2, the average age of DUs who accepted the traditional intervention or the innovative intervention was 30.0 ± 7.3 or 32.8 ± 7.7 years, respectively. In both DU groups, most of DUs were male (Table 2). More than 90% of DUs belonged to Zhuang ethnic nationality. Most of DUs only had the educational level of junior middle school or lower. More than 60% of DUs had no regular sexual partner(s) (Table 2). Between the two intervention groups, there is no significant difference (p > 0.05) in most demographic characteristics, including age, gender, ethnic group, household registry, and education level, except in regular sexual partner(s) (p < 0.05).
Calculated by Fisher test.
Basic knowledge and awareness of HIV/AIDS of FSWs and DUs during two intervention periods
During the period of traditional or innovative intervention, both FSW and DU populations had a high level of knowledge of HIV/AIDS. HIV knowledge was assessed with eight questions designed by Chinese CDC. 18 The correct rates of eight questions of the questionnaire were all higher than 90%. Definitely, 99.08% FSWs and 98.52% DUs got awareness level in traditional intervention period, and 98.73% FSWs and 99.10% DUs got awareness level in innovative intervention period. There is no significant difference (p > 0.05) in knowledge level between the two intervention groups, either in FSW or in DU population.
The changes of behavior of condom use in FSWs between traditional and innovative interventions
As shown in Table 3, during traditional intervention, 96.88% FSWs used condoms in the last commercial sex and 72.06% FSWs used condoms for all commercial sex in the last month. During innovative intervention, the data increased to 99.49% and 96.82%, respectively. Statistical analysis shows that there are significant differences between traditional and innovative intervention groups (p < 0.05) (Table 3).
The changes of high-risk behaviors among DUs between traditional and innovative interventions
When comparing the innovative intervention with traditional intervention, the proportion of DUs who had injection use of drug in the last month dropped from 92.99% to 64.29%. The proportion of DUs who had commercial sex in the last year dropped from 17.20% to 5.94% (Table 4); among them, the rate of condom use all the time increased from 14.06% to 76.09% (Table 4). During innovative intervention, a downward trend was observed in proportion of DUs who injected drugs in the last month (Cochran-Armitage trend test, Z = −10.67, p < 0.01; data no show). In both interventions, almost all DUs who injected drugs did not share needles. However, about 90% of DUs who had regular sexual partner(s) did not use condom when they had sex with their partner (s). For these two high-risk behaviors, there is no significant change between the two interventions (p > 0.05) (Table 4).
Calculated by Fisher test.
For other high-risk behaviors, including injection use of drug in the last month, having commercial sex in the last year, and condom use in each commercial sex in last year, the changes were all significantly different between the two interventions (p < 0.05) (Table 4).
Stratification analysis
Because several demographic characteristics have a significant difference between traditional and innovative intervention groups (Tables 1 and 2), we utilized Mantel-Haensze stratification to analyze whether the differences affect the results about the changes of knowledge level and high-risk behaviors by innovative intervention.
After stratification, the differences in ethnic group and household registry no longer affected HIV/AIDS knowledge level (p > 0.05) among FSWs; however, they still significantly affected condom use in the last commercial sex and condom use in each commercial sex in the last month (p < 0.01) (Table 5). The difference in whether having a regular sex partner(s) did not affect HIV/AIDS knowledge level and needle sharing in the last month (p > 0.05) among DUs, but it still significantly affected injection use of drugs in the last month and having commercial sex in the last year (p < 0.01) (Table 5).
DUs, drug users; FSW, female sex worker.
Analysis of HIV epidemic by GM (1,1) model
We established a gray GM (1,1) model based on the number of new HIV cases in Longzhou county during 2003–∼2014 (Fig. 2). The residuals ratio C of the model is 0.5. The posteriori error ratio and small error probability test (Table 6) indicate that the fitting accuracy of the model reaches the level qualified and can be used for extrapolation forecast. By the model prediction, the predicted numbers of HIV/AIDS new cases were 233 for 2012, 272 for 2013, and 317 for 2014, respectively. However, the actual new HIV cases in Longzhou during 2012–2014 were significantly lower than predicted ones (Fig. 2).
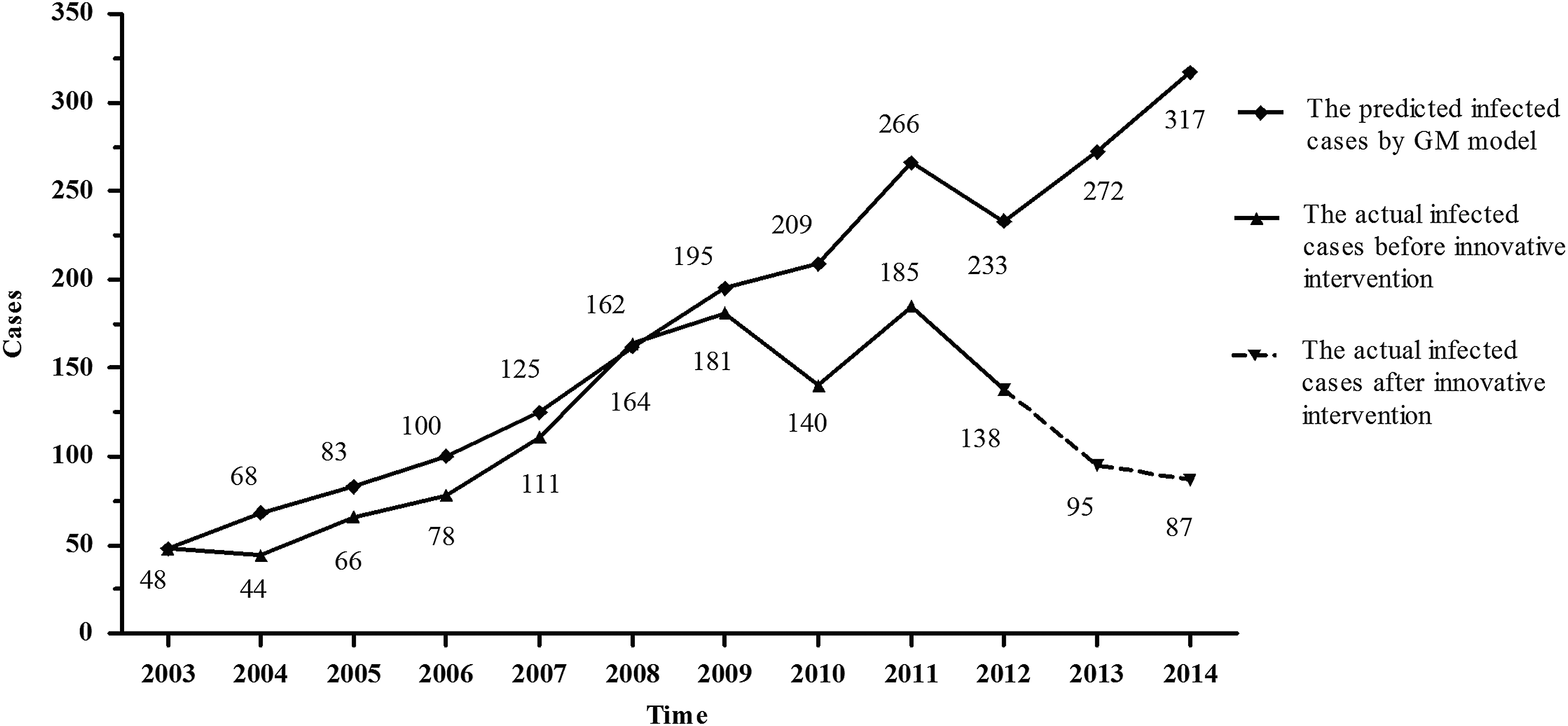
Comparison of the real values and fitting forecast values by GM (1,1) model for Longzhou county's new HIV infection cases.
Moreover, actually, the HIV incidence was 19.01/10,000 (506/266,100) for innovative intervention period and 12.01/10,000 (320/266,366) for traditional intervention period, respectively. The risk ratio of HIV acquisition in the innovative intervention group compared with the traditional intervention group was 0.631 (95% confidence interval 0.549–0.726), which corresponds to a reduction in the risk of acquiring an HIV infection in the traditional intervention group of 36.9% (27.4–45.1).
CEA of innovative intervention
During innovative intervention, a total of 1,295,000 US dollars (USD) were spend on HIV/AIDS prevention and control in Longzhou, including 223,000 USD for 2012, 680,000 USD for 2013, and 392,000 USD for 2014, respectively. Based on the gray GM (1,1) model (Fig. 2), the predicted numbers of HIV/AIDS new cases was 233 for 2012, 272 for 2013, and 317 for 2014, respectively. The total number is 822. However, actually, only 320 new cases of HIV/AIDS were reported during 2012–2014. Therefore, the avoided infection number is 502, and the cost of each avoided case is 2579.68 USD. Referenced by the domestic HIV/AIDS epidemic data 22,23 that each case HIV/AIDS DALYs loss is 20.76, the CEA is 124.26 USD/DALY loss, indicating that innovative intervention restores each DALY loss costing an average of 124.26 USD.
Discussion
In this study, we investigated the effects of the village-level intervention model that was implemented in Longzhou county and found that this innovative intervention could effectively reduce the risky behaviors of FSWs and DUs. A downward trend in HIV incidences was observed during innovative intervention, indicating that the village-level intervention does produce a positive influence on the local HIV epidemic, which provides new evidence to support the effectiveness of community-based interventions.
Although “county-township-village” allied intervention implemented in Longzhou is not the first attempt in rural areas in China, 24,25 to our knowledge, this study is the first one to systematically analyze the effects of “county-township-village” allied intervention in rural China through the HIV-/AIDS-related KAB between two interventions, local HIV incidence, and CEAs of innovative intervention, and the first one to design village-level intervention in Guangxi, China.
From this study, first, the effectiveness of traditional intervention, namely CDC-based intervention, can be seen. At least, the knowledge of HIV/AIDS in both FSW and DU populations have reached a fairly high level, which were even very high compared to other places in China. 26 Some risky behaviors were also under good control as well, including the rate of condom use in last commercial sex among FSWs (Table 3) and the rates of needle sharing and having commercial sex in the last year among DUs (Table 4). However, other risky behaviors were still unsatisfying. In FSW population, the rate of condom use was still low (72.06%) (Table 3); in DU population, most people (92.99%) had injection use of drug; and most DUs did not use condom, either in commercial sex or in sex with their regular sexual partner (Table 4).
These results indicate that the traditional intervention had a certain impact on the level of HIV/AIDS knowledge and some risk behaviors, but it is insufficient. Although FSWs in China already had a relatively high level of HIV/AIDS basic knowledge, they are often in a relatively passive position in decision of condom use or not due to biological, cultural, economic, and judicial influences. 27
Moreover, Chinese FSWs might be reluctant to argue with their clients, fearing both income loss and violence. 28,29 The situation is more serious in mid-age FSWs and older FSWs, 30,31 who may experience more stigma and are socially isolated because of their low socioeconomic status, enduring structural inequities, and a disparate burden of familial support. The inconsistent HIV/AIDS knowledge level and risky behaviors reflect that the phenomenon of separation of knowledge and behaviors is somewhat popular among FSWs in China. 32
During the innovative intervention, the separation of knowledge and behaviors had been improved significantly. The rates of condom use in FSWs were significantly increased (Table 3). The incidence of injecting drug and commercial sex in DUs also decreased, and much more DUs used condoms when they had commercial sex (Table 4). Our results confirm that innovative intervention substantially reduces the risk of acquiring an HIV infection. Innovative intervention provided a 36.9% (27.4–45.1) protective effect against HIV acquisition compared with the traditional intervention. As a consequence, a downward trend was observed in HIV new cases during innovative intervention.
We consider that the biggest difference between traditional intervention and innovative intervention is that the latter has truly practiced various interventions, including HIV-/AIDS-related education, free condoms, regular HIV testing, and needle exchange for all residents, including high-risk populations, general population, and HIV-infected persons, which depends on village clinic doctors' participation.
As some previous studies indicated, village clinic doctors were more capable of effectively carrying out the public education campaigns and intervention programs because they knew each local villager very well in rural areas. 33,34 The well-trained staff from village clinics and township hospitals were more persuasive in education of HIV/AIDS prevention knowledge, as previous studies have shown that HIV/AIDS prevention knowledge from different sources will produce different results and people are most willing to accept the prevention knowledge from medical professionals. 35
In addition, the village-level intervention may reduce community stigma against HIV-infected persons and contribute to the increase of disclosure of HIV status and HIV care, because this intervention not only targets high-risk populations but also the whole population. As previously reported, 36 women living in China had significant lower levels of disclosure compared with those living in Western Europe/Canada, and community stigma severity was greater in China. However, this study could not address the effects of village-level intervention on community stigma and disclosure of HIV status, which is worthy of further research as a significant topic.
Several demographic characteristics have a significant difference between traditional and innovative intervention groups (Tables 1 and 2). After stratification analysis, the difference in ethnic group still significantly affected condom use in FSW population (Table 5). This result reflects that FSW population in Longzhou has high mobility, which is believed to be related to the illegal nature of sex work in China. 27 Because the traditional intervention has been implemented nationwide in all ethnic groups for many years, including minority areas and minority ethnic groups, we believed that the difference in ethnic group in FSW population would not significantly affect the analysis results of this study.
Nevertheless, FSWs' geographical mobility is a big challenge to China's HIV/AIDS prevention and control. 37 It is difficult to maintain continuing education and counseling programs targeted at the individual level among this mobile population. It is necessary to develop special and effective intervention for this floating population. A similar situation was found in DU population. After stratification analysis, the difference in whether having a regular sex partner(s) significantly affected injection use of drugs (Table 5). We also believed that this difference would not significantly affect the analysis results, because all DUs are considered to have similar background of traditional intervention.
Our study demonstrates that the average cost to avoid one case of infection was 2579.68 USD and the average cost to restore one DALY was 124.26 USD, which were comparable to the cost of traditional intervention in China. A previous article showed that it cost 2502–2940 USD to avoid one case of infection and 120–142 USD to restore one DALY in Henan Province, China, by traditional intervention. 22 Another study showed that the average cost to avoid one case of HIV infection was 1566–4153 USD in Xinjiang Province where the traditional intervention was implemented. 38 Obviously, village-level model does not cost much, making it particularly useful for rural areas in China.
This study suffers from some limitations. First, as mentioned above, the demographic characteristics of Longzhou county's FSWs and DUs demonstrated some variations between the two periods when the traditional and innovative interventions were implemented.
Second, only the data of FSWs and DUs were available from the databases of local CDC. Therefore, we cannot assess the effects of innovative intervention on other high-risk populations and healthy people for their changes of HIV/AIDS KAB. Findings may not be generalizable for the entire county. However, sexual transmission and injection drug use were the two dominant routes for HIV transmission in Longzhou county.
Third, the long-term effects of the innovative intervention need further evaluation. After 3 years of intervention, the risky behaviors of FSWs and DUs were greatly improved, and a downward trend was observed in HIV incidences. Whether the behaviors change and the downward trend of HIV incidence could be maintained or improved for longer periods need to be verified in further follow-up study.
In summary, “county-township-village” allied intervention could effectively decrease rural FSW and DU populations' HIV-/AIDS-related risky behaviors and controlled local HIV incidence. This type of village-level intervention for HIV/AIDS prevention and control can serve as a model for other rural areas in China to curb the local HIV epidemic and provides a good reference for further research.
Footnotes
Acknowledgments
The study was supported by National Natural Science Foundation of China (NSFC, 81560326, 81271851, 31360033, 81460511, 81360259), Guangxi Scientific and Technological Key Project (Gui Ke Gong 14124003-1), Key Projects of Guangxi Universities Scientific Research (2013ZD012, 2013GXNSFCB019004), Guangxi University “100-Talent” Program, and Guangxi university innovation team and outstanding scholars program (Gui Jiao Ren 2014[7]). We would like to express our gratitude to all staffs from Longzhou County Center for Disease Control and Prevention (Guangxi, China) for collecting and providing epidemiological data of local HIV/AIDS, and this study was also supported by Guangxi Center for Disease Control and Prevention (Guangxi, China).
Authors' Contributions
H.L., L.Y., and W.G. conceived and designed the study. J.Y., Y.Z., and J.J. conducted the data analysis and literature review and drafted the article. J.Y., Y.Z., Q.L., D.L., K.F., and Y.H. were involved in the study supervision, data collection, and interpretation of the data. B.L., J.H., C.N., Y.L., J.L., W.W., and F.Q. assisted with data management and data analysis. All authors contributed to the revision of the article and approved the final version.
Author Disclosure Statement
No competing financial interests exist.