
Abstract
Innovative empirical frameworks to evaluate progress in efforts addressing HIV treatment and prevention barriers in resource-limited areas are sorely needed to achieve the UNAIDS 90-90-90 goal (90% diagnosed, 90% on treatment, and 90% virally suppressed). A triadic implementation framework (TIF) is a comprehensive conceptual tool for (1) monitoring attrition, (2) evaluating operational programs, and (3) measuring the impact of specific implementation goals within the care continuum. TIF will assess the effects of enhanced programs on adherence and virologic suppression within the HIV care continuum at a regional clinic in the Dominican Republic (Clínica de Familia La Romana [CFLR]) and its program serving high-risk, migratory batey (sugarcane cultivation) communities. A retrospective cohort study completed during 2015 collected deidentified data from a CFLR chart review of adult HIV patients diagnosed in 2013. The results were quantitatively analyzed and compared to 2011 cohort data. In 2013, 310 patients were diagnosed HIV positive. The results demonstrated 73% enrolling in care, 28% adhering to care, and 16% achieving viral load suppression. Engagement increased across all steps of the care continuum compared to a 2011 cohort, culminating in a significant increase in undetectable viral load from 4% to 16% (p < 0.001). The batey program showed significant increases in patient enrollment compared to the 2011 cohort (p < 0.001). Meeting the UNAIDS 90-90-90 goal requires enhanced services in high-burden, resource-limited regions. CFLR employs TIF to assess progress and programmatic areas in need of strengthening. Data suggest enhanced CFLR services improve outcomes. Given improvements, maintenance and expansion of similar programs are warranted to achieve the 90-90-90 goal.
Introduction
W
The Caribbean has the highest adult HIV prevalence in the world after sub-Saharan Africa, at 1% in 2015. 6 The island of Hispaniola, shared by the Dominican Republic (DR) and Haiti, is a resource-poor setting in the Caribbean. 7,8 The adult prevalence rate of HIV in the DR is 0.8%, with key populations at considerably higher risk. 6,9 –11 Clínica de Familia La Romana (CFLR) is a non-profit organization licensed by the Dominican Ministry of Health to provide outpatient and community-based healthcare, with a particular focus on HIV care. 12 CFLR uses a multi-disciplinary approach to family-centered care, including free, comprehensive, and HIV-specialized care. 13 –15 As the largest HIV clinic in the DR located outside of the capital, CFLR is considered a national model, addressing prevention, care, and treatment needs through evidence-based programming, including male circumcision and prevention of vertical transmission programs. 16 –21
One of the key populations in La Romana and surrounding provinces are migratory batey workers. 7 Bateyes are communities of sugarcane workers and their families comprised primarily Haitians and Haitian Dominicans with substantial barriers to education and accessing healthcare services, with HIV prevalence rates ranging from 3.0% to 9.0%. 22 –25
Batey populations are at an increased need for HIV program implementation to curb HIV incidence and prevalence by overcoming barriers, including access to care and stigma. 26 –29 CFLR strived to overcome these barriers with a batey outreach program that sent community healthcare workers to conduct free HIV testing, linking those diagnosed with HIV to care at CFLR.
CFLR utilizes the HIV care continuum framework to assess structural-, social-, and individual-level barriers for patients. The HIV care continuum (Fig. 1) quantitatively depicts goals and barriers for testing, linkage to care, retention, and virologic suppression. 14,30,31 Effective HIV treatment as prevention depends on reducing attrition consistently throughout the diagnosis and treatment process. 32,33 Separated into seven steps, CFLR monitors patient attrition from (1) HIV diagnosis through (2) enrollment in clinic services, (3) CD4 testing, (4) becoming eligible to start ART according to national guidelines, (5) initiating ART, (6) adhering to treatment, and finally (7) achieving a suppressed viral load.
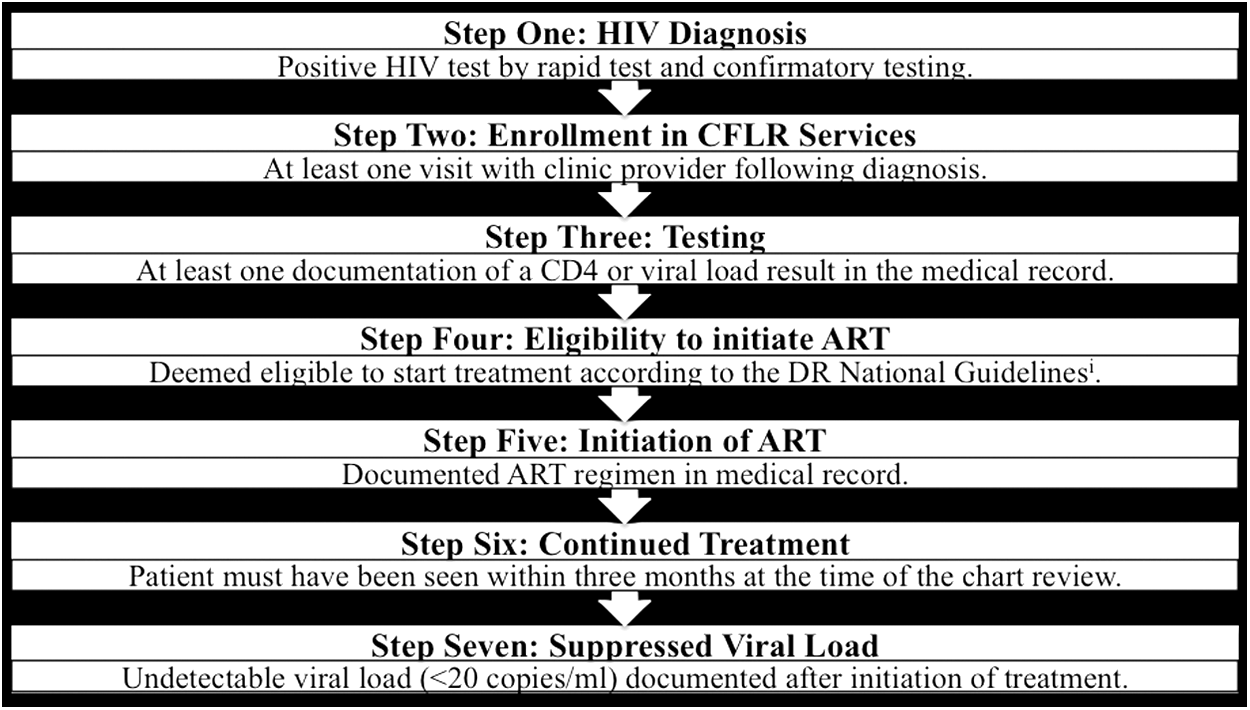
Visual representation of the HIV care continuum as defined by CFLR. The DR National Guidelines for ART are derived from the Dominican Ministry of Health. The 2013 Guidelines suggested treatment initiation when the CD4 count was at or below 350 cells/mL. 36 ART, antiretroviral therapy; CFLR, Clínica de Familia La Romana; DR, Dominican Republic.
Continued monitoring of existing HIV care structures is critical to application of the HIV care continuum and improvement of HIV treatment in the region. 5 Surveillance data can be used to identify patients lost to follow-up, alert providers, and promote reengagement of patients lost to follow-up. 34 Innovative empirical frameworks to evaluate progress in efforts addressing HIV treatment and prevention barriers in resource-limited areas are sorely needed to achieve the UNAIDS 90-90-90 goal and end the AIDS epidemic, as has been shown possible in other resource-limited nations. 35 To this end, this study adapts a triadic implementation science approach originally identified by PEPFAR that includes (1) monitoring and evaluation to track the performance of individual components of HIV treatment, (2) operations research that utilizes baseline data to assess the efficiency of program implementation, and (3) impact evaluation that explains the effect of specific implementation goals. 34 The adapted CFLR triadic implementation framework (TIF) (Fig. 2) and the HIV care continuum model to evaluate sustainable treatment, prevention, and care programs in the La Romana province.
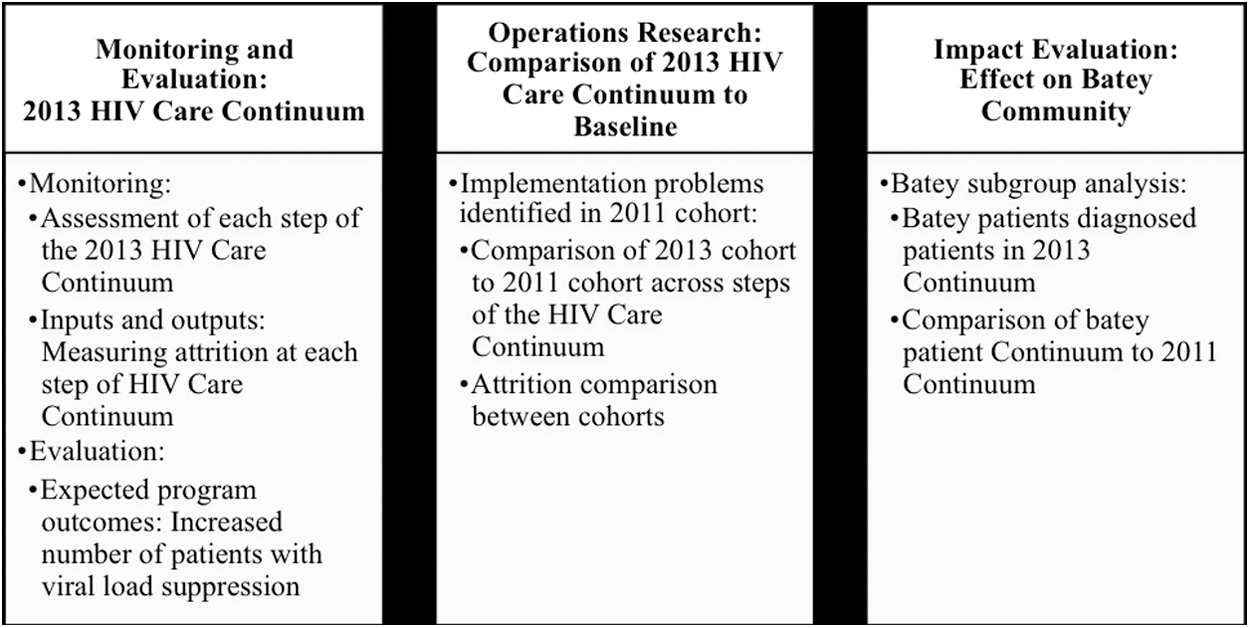
The CFLR Triadic Implementation Framework (TIF) Approach to HIV Care: The three constructs of the TIF are (1) monitoring and evaluation, (2) operations research, and (3) impact evaluation assess CFLR efforts. This diagram seeks to describe the specific focuses of each area as related to CFLR and its programmatic efforts. CFLR, Clínica de Familia La Romana.
This retrospective cohort study seeks to apply the TIF to assess the effects of enhanced programs on adherence and virologic suppression within the HIV care continuum at CFLR and its batey program. Specifically, this study will assess the CFLR and batey programs with the HIV care continuum through measuring attrition, adherence, and virologic suppression. The results can be used to ensure existing treatment programs are tailored to the needs of the region, with an additional focus on the batey community.
Methods
Theoretical framework: CFLR implementation science approach to HIV care
A TIF is a comprehensive conceptual tool for (1) monitoring attrition, (2) evaluating operational programs, and (3) measuring the impact of specific implementation goals within the care continuum. The TIF focuses on monitoring and evaluation through assessment of the 2013 HIV care continuum data in the retrospective study. This will be accomplished through describing attrition rates at each step of the continuum.
The TIF evaluates operations research by focusing on the programmatic aspects of the clinic and measuring their effectiveness in comparison to the 2011 cohort baseline HIV care continuum data. These data were derived from the same HIV care continuum criteria as this study and were published by Bowman et al. in one of the first studies to document the HIV care continuum in the region. 20 Specifically, this aims to depict the effectiveness of the solutions that the clinic's quality improvement committee (created in 2011) developed and implemented since the baseline study, including the implementation of an adherence-counseling program that requires two sessions before initiating ART. Patients who missed clinic visits were also referred to adherence counseling started in 2011. The difference in attrition rates between the HIV care continuum steps compared between cohorts will allow for an overall assessment of the success of these efforts.
Finally, the TIF seeks to describe the impact evaluation of the CFLR batey program. This will involve subgroup analysis from the 2013 continuum as well as comparison to the 2011 data to determine the impact of outreach for batey residents. Since the baseline data were collected, the CFLR batey program expanded to include staff members who explicitly worked on increasing enrollment, a barrier previously identified. 20 Attrition rates for the batey community in the HIV care continuum as well as comparison to baseline data will allow for an overall assessment of the CFLR batey program enhancements as well as the unmet needs of the batey community.
Setting
CFLR provides comprehensive healthcare to patients in the southeastern region of the DR. At the end of 2015, a total of 1798 active adult HIV-positive patients were being seen at the clinic, a 7% increase from 2014. 15 CFLR provides confidential HIV testing to the community. CFLR has a database of enrolled patients that it draws upon to contact patients who miss appointments and are not heard from in 3 months. Until March 2015, the clinic also oversaw a batey program in which community healthcare workers conducted daily HIV testing and education in the impoverished communities of sugarcane workers. For this study, batey residents are identified as independent from CFLR patients.
Data collection
A chart review collected demographic, testing, and follow-up data in summer 2015 for all adult patients diagnosed as HIV positive by CFLR in 2013. One limitation of this database is that it does not indicate mortality for those lost to follow-up. This paper also utilized aggregate data published by Bowman et al. 20
Statistical analysis
Statistical analysis was performed using STATA 14 software. Differences were compared using chi-square and Fisher's exact test with a significance level defined at 0.05.
Ethics and consent
As a retrospective study, all data were collected deidentified from patient records. Two ethics committees, Columbia University Medical Center IRB (study protocol AAAP5052) and the Dominican National Commission for Health Bioethics (DR CONABIOS, study protocol 026-2015) approved this study.
Results
Monitoring and evaluation: The 2013 HIV care continuum
In 2013, 310 patients were diagnosed HIV positive at CFLR and through the CFLR batey program. Of the 310 diagnosed, 225 patients were enrolled into care during 2013. Demographic data, shown in Table 1, were obtained at the time of enrollment for the 225 patients. The majority of patients enrolled were Dominican and non-batey residents.
Patients who are identified as Clinic patients are not residents of bateyes in this cohort.
Patients who were diagnosed at CFLR.
Patients who were diagnosed through the CFLR batey program.
ART, antiretroviral therapy; CFLR, Clínica de Familia La Romana.
Bold values indicate statistically significant findings at p < 0.05.
Of the 310 patients diagnosed as HIV positive, 225 (73%) patients were enrolled in the clinic, 206 (66%) of the patients had at least one CD4 or viral load documented, 173 (56%) were considered eligible for treatment, and 130 (42%) patients initiated antiretroviral treatment. At the time of chart review, 88 (28%) patients were active on treatment, including nine who were still ineligible for treatment, but regularly attended HIV monitoring appointments. A total of 166 patients had completed viral load testing after 1 year of treatment. Twelve months after initiation of treatment, 51 (16%) patients had a documented undetectable viral load.
The three steps with the highest attrition rates were: (1) of those who were diagnosed, 73% enrolled in care; (2) of those initiated ART, 68% remained active after 1 year; and (3) of those who remained active in care, 58% achieved an undetectable viral load.
Operations evaluation: HIV care continuum comparison
Figure 3 shows the HIV treatment continuum by year of diagnosis. Collected data were compared to 2011 cohort data published by Bowman et al. 20
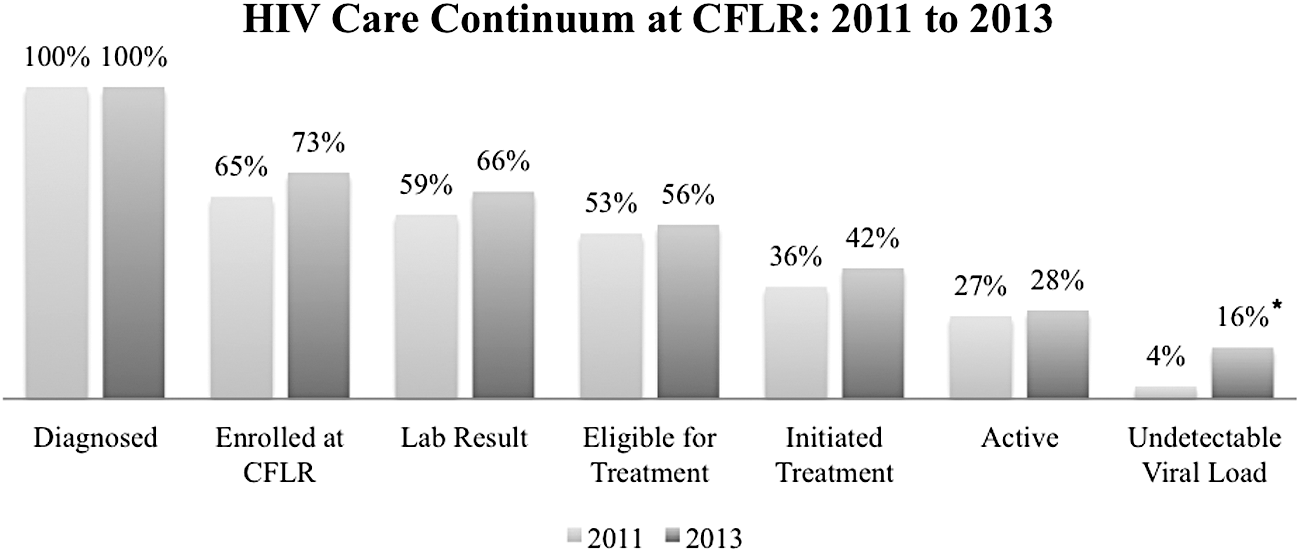
Represents the comparison of 2011 and 2013 data along steps of the cumulative HIV Care Continuum. Statistically significant difference represented with asterisk.
Improvements were made in every step of the continuum from 2011 to 2013. The greatest difference between the two cohorts was noted in patients achieving viral suppression (12.6% cumulative increase from 2011, p < 0.001). Additional, non-statistically significant improvements were observed in the other steps of the continuum, including an 8% increase in patient enrollment, a 7% increase in completing testing, and a 6% increase in initiating treatment. This statistically significant increase in virally suppressed patients is notable both for all patients (p < 0.001) as well as clinic diagnosed patients (p < 0.001), but not batey diagnosed patients (p = 0.604).
Moreover, in the 2011 cohort, 80% of patients had a 6-month or greater interval between testing and CD4 monitoring—a guideline for care in the DR—while at the time of this study, only 42% had an interval greater than 6 months. Similarly, 88% of patients had a 6-month or greater interval between viral load testing in the 2011 cohort, compared to 60% of patients who had greater than 6 months between testing during this study review.
Impact evaluation: bateyes
The quantity of batey patients who enrolled in care at CFLR increased by 2.7 times—46 in the 2013 batey cohort compared to 17 in the 2011 batey cohort. This resulted in a statistically significant increase in the number of patients diagnosed in the bateyes who then enrolled in clinic care (p < 0.001). As a result, the proportion of batey patients who initiated and completed subsequent steps of the continuum increased proportionally.
Discussion
This study utilized TIF to assess enhanced CFLR and batey programs with the HIV care continuum for all patients diagnosed HIV positive in 2013. Of all patients diagnosed, 16% achieved viral load suppression. The highest rates of patient attrition were noted at clinic enrollment, adherence to care, and achievement of undetectable viral load. Adherence to clinic appointments remains an issue in this cohort, with one-third of those who initiated treatment being lost to follow-up a year later. The results indicate that the clinic's enhanced programs, including the adherence-counseling program and batey outreach program, resulted in viral suppression improvements in the care continuum, but further efforts are required at all steps of the continuum in order for the clinic and the region to achieve the 90-90-90 target.
The number of batey patients enrolled in 2013 was significantly more than the 2011 cohort, thereby increasing the initiation of the HIV care continuum for the batey community in 2013. However, the lack of additional significant differences between the 2011 and 2013 batey cohorts signifies a need for additional efforts. Without significant improvements, the batey community data demonstrate continued barriers not impacted by diagnostic and enrollment efforts, such as stigma. 29 Limited efforts addressing the batey community should be remedied through interventions such as enrollment and adherence programs tailored for this vulnerable population. The discontinuation of CFLR's HIV testing program in bateyes in 2015, because of grant funding ending, has resulted in an interruption in vital services for this high-risk population. This program, while conservative in its outcomes, was a unique model addressing care for this population. This study highlights the need for an increase in funding and research specifically for this community and development of batey-specific outreach programs to help increase healthcare access and adherence. Important limitations to this study include that the sample population was restricted to adults enrolled at a singular clinic in the DR, which restrict the generalizability of the results.
Meeting the 90-90-90 goal requires enhanced services in high-burden, resource-limited regions. CFLR employs TIF to assess progress and programmatic areas in need of strengthening. Data suggest that enhanced CFLR services improve outcomes and virologic suppression. Given improvements, maintenance and expansion of similar programs are warranted to achieve the 90-90-90 goal.
Footnotes
Acknowledgments
Authors would like to thank all staff at the Clínica Familia La Romana and the Columbia University IFAP Global Health Program.
Author Disclosure Statement
No competing financial interests exist.