
Abstract
Black persons with HIV are less likely than white persons to experience viral control even while in treatment. We sought to understand whether patient characteristics and site of care explain these differences using a cross-sectional analysis of medical records. Our cohort included 8779 black and 7836 white patients in the Veterans Administration (VA) health system with HIV who received antiretroviral medication during 2013. Our primary outcome, viral control, was defined as HIV serum RNA <200 copies/mL. We examined the degree to which racial differences in viral control are related to site of care, patient characteristics (demographics, HIV treatment history, comorbid conditions, time in care, and medication adherence), retention in care, and combination antiretroviral therapy (cART) adherence, using multi-variable logistic regression models. Compared to whites, blacks were younger and had lower CD4 counts, more comorbidities, lower retention in care, and poorer medication adherence. The odds of uncontrolled viral load were 2.02 (p < 0.001) for black relative to white patients without risk adjustment (15% vs. 8% uncontrolled viral load, respectively). The odds decreased to 1.83 (p < 0.001), 1.65 (p < 0.001), 1.62 (p < 0.001), and 1.24 (p = 0.01) in models that sequentially controlled for site of care, age and clinical characteristics, care retention, and cART adherence, respectively. Overall, 51% of the viral control difference between blacks and whites was accounted for by adherence; 26% by site of care. We conclude that differences in the site of HIV care and cART adherence account for most of the difference in viral control between black and white persons receiving HIV care, although the exact pathway by which this relationship occurs is unknown. Targeting poorer performing sites for quality improvement and focusing on improving antiretroviral adherence in black patients may help alleviate disparities in viral control.
Introduction
E
To date, the lower rates of viral control in black compared to white patients are not fully understood. Possible explanations include initiation of cART later in the course of the disease, 13 lower retention in care, 4,14 or lower medication adherence for black populations. 10,15,16 In addition, studies of other conditions, such as cancer and cardiovascular disease, have found that disproportionate use of lower quality providers and care sites by black populations partly explained racial disparities in outcomes. 17 –19 The impact of the provider and care site quality on differences in outcomes for black and white persons with HIV has not been investigated.
The Veterans Health Administration (VHA) is a useful setting to examine racial disparities in HIV care and outcomes. First, it is the largest provider of HIV care in the United States, with ∼26,000 Veterans in care, 20 in over 100 facilities across the country. Second, VHA is an equal access healthcare system with few financial barriers to care in the form of co-pays, which have often been found to be a significant contributor to disparities. 21 Finally, VHA's integrated electronic health record and national data warehouses allow tracking of laboratory, medication, and quality measures among Veterans with HIV.
Racial disparities in HIV viral control have been documented in the VHA, despite its equal-access system. 22 We sought to identify factors related to racial disparities in viral control between white and black patients receiving HIV care in VHA, to guide interventions to reduce disparities. Specifically, we examined the degree to which racial differences in viral control are associated with differences in site of care, patient clinical characteristics (i.e., time in care, illness severity, and comorbidity), retention in care, and antiretroviral medication adherence.
Methods
Data sources and variables
We used national data extracted from VHA's Corporate Data Warehouse (CDW) to complete a cross-sectional study of Veterans in care for HIV infection in VHA between January 1, 2013 and December 31, 2013. CDW includes data elements extracted from VHA's integrated electronic health record and administrative files, including patient demographics and residential ZIP codes, inpatient and outpatient visits, laboratory results, pharmacy records, and vital signs.
The cross-sectional cohort was defined using a previously validated case finding algorithm, which required one inpatient or two outpatient International Classification of Diseases—Ninth Revision—Clinical Modification (ICD-9-CM) codes for HIV infection (i.e., V08 or 042) during 2013. 23 This method has sensitivity of 90% and specificity of 99% for identifying Veterans in care for HIV infection, compared to a method that includes manual chart review. 23
We included veterans with a single outpatient code for HIV infection and at least two medication fills anytime during 2013 for antiretroviral medications used only to treat HIV infection (Fig. 1), resulting in 24,788 initial patients. Of these, we limited the cohort to 21,955 veterans who were seen in a VA Infectious Disease (ID) specialty clinic at least once during 2013. We excluded patients not seen in ID clinics because many of these veterans receive HIV care outside of VA. 24 Moreover, since the 1980s, VA has concentrated care for Veterans with HIV in 113 geographically dispersed ID specialty clinics, 25 with 83% seen in an ID clinic at least once in 2012. 26 We further excluded 1584 patients who were seen in more than one ID clinic during 2013 and 2723 patients with no cART use or whose first cART fill was <180 days before the last viral load measurement. cART was defined as receipt of at least two antiretroviral medications from at least two classes (i.e., non-nucleoside reverse transcriptase inhibitors, nucleoside reverse transcriptase inhibitors, protease inhibitors, integrase inhibitors, and entry inhibitors) or co-formulated abacavir/zidovudine/lamivudine. Our primary outcome was viral control, defined as HIV serum RNA <200 copies/mL on the last viral load measurement date in 2013.

Cohort selection.
We limited the final sample to patients who were either black or white race (n = 16,615). Veteran race was defined as black or white based on the race recorded on VHA encounter data. If race was classified differently for a Veteran across encounters, we selected the race category the patient reported most often. If no difference existed in the number of times conflicting race categories were reported, we classified the patient's race as missing. This occurred for <0.5% of patients. In prior studies that compared data on race/ethnicity in VHA records to Medicare and Department of Defense data, the highest rates of concordance were for white and black patients (99% and 96%, respectively). 27
We created a series of variables representing patient characteristics that are known to be associated with viral control based on previous literature. These included patient demographics (age and sex), HIV treatment history (time in HIV care, time on cART, CD4 cell count nadir based on lowest CD4 cell count on record in VHA, and presence of AIDS defining illness), comorbid conditions (e.g., stroke, substance use, and coronary artery disease), treatment retention, and medication adherence. Time on cART was measured as days between the first cART fill in a VA pharmacy and the last viral load measurement date. Time in HIV care was defined as the number of days between the first HIV diagnostic code on record and the date of the last viral load measure in 2013 (for a small number of patients, the first cART fill occurred before the first HIV diagnostic code appearing in the medical record. For those patients, the date of first cART fill was used to define time in HIV care). Indicators for comorbid conditions were defined using algorithms that were previously validated by the Veterans Aging Cohort Study (VACS) and are based on ICD-9-CM diagnosis codes. 28
Following the measure tracked in VHA, retention in care was defined as having two or more visits in a VA ID clinic or primary care clinic at least 60 days apart during the 12 months before the last viral load test date in 2013. Finally, patient adherence to cART was defined using the proportion of days covered (PDC) algorithm 29 and reflect the proportion of days of cART eligibility on which the patient had at least two antiretroviral drugs in his or her possession, based on medication refill patterns. Adherence was measured during the 12 months preceding the last viral load measurement date during 2013 (for patients who initiated cART between 6 and 12 months before the last viral load date, adherence was measured from the date of cART initiation).
Analyses
Analyses of racial differences in viral control included three main steps. First, we compared characteristics of black and white patients with HIV. Continuous variables (e.g., age) were compared using analysis of variance, while categorical variables (e.g., presence of AIDS defining illness) were compared using a chi-squared statistic. Specific groups of variables included demographics (age and sex), HIV severity (time in HIV care, CD4 count nadir, or presence of AIDS defining illness), comorbidities (hypertension, substance abuse, depression, hepatitis C, coronary artery disease, diabetes, stroke, and chronic kidney disease), retention in care, and cART adherence.
Second, we examined correlates of racial differences in viral control using multi-variable logistic regression models in which the dependent variable represented whether the patient's most recent viral measure was >200 copies/mL (i.e., uncontrolled). The coefficient associated with black race was estimated in four models that sequentially controlled for clinic using fixed effects, patient demographic and clinical characteristics, retention in care, and cART adherence. As each group of variables was added, alternative specifications of specific variables were evaluated to provide the best fit (e.g., income as continuous or income as categorical). The difference between the black race coefficient derived from models that employed one, two, three, or all sets of variables was calculated. This modeling process was repeated 1000 times using samples bootstrapped with replacement, so that the impact of each potential set of correlates on the coefficient for black race could be quantified using statistical inference. Finally, we used the method of recycled predictions 30 to estimate the risk-adjusted likelihood of uncontrolled viral load for black and white patients, based on each set of mediators. In this method, predicted rates of unadjusted viral control for black and white patients are calculated for two sets of patients that are identical on all covariates except race. Models were fit using SAS Enterprise Guide v7.4. Copyright © 2014 by SAS Institute, Inc. (Cary, NC). All analyses were approved by the Institutional Review Board at Iowa City VA.
Results
Table 1 shows characteristics of 8779 black and 7836 white patients who met eligibility criteria. Black patients were somewhat younger, with 14% of black patients over the age of 65 compared to 23% of white patients. Black patients also had lower CD4 NADIR values, with 52% less than 200 cells/mm3 compared to 43% of white patients less than 200 cells/mm3. Blacks were more likely to have several comorbid conditions, including alcohol abuse, drug abuse, hepatitis C, hypertension, diabetes, and chronic kidney disease. They were less likely to have a history of coronary artery disease. Black patients had modestly lower likelihood of retention in care (89% vs. 92% for black and white patients, respectively). Finally, the mean PDC by two or more cART medications was significantly lower for black compared to white patients (71% vs. 81%; p < 0.001). Blacks tended to be concentrated in fewer ID clinics, with 50% of black patients receiving care in 37 ID clinics, while 50% of white patients received care in 58 ID clinics (not shown in Table 1).
cART, combination antiretroviral therapy; SD, standard deviation; VA, Veterans Administration.
Table 2 shows risk adjustment logistic regression models estimated using the full sample, for each model in the mediation analysis. The odds of uncontrolled viral load were 2.02 [95% confidence interval (CI), 1.82–2.23; p < 0.001] times higher for black versus white patients, before controlling for clinic and other factors (15% vs. 8% uncontrolled viral load, respectively). The relative odds decreased to 1.83 (p < 0.001) in a model that controlled for care site by including ID clinic as fixed effects (model 1) and decreased to 1.65 (p < 0.001), 1.62 (p < 0.001), and 1.24 (p = 0.01) in models that sequentially added variables controlling for clinic, age and clinical characteristics, care retention, and cART adherence, respectively (models 2–4).
cART, combination antiretroviral therapy; ID, infectious disease.
Figure 2a shows risk-adjusted rates (and 95% CIs) of uncontrolled viral load in black and white patients with no risk adjustment and in models that control for clinic only, demographic and clinical characteristics only, retention in care only, and cART adherence only, based on 1000 bootstrap iterations and recycled predictions. Figure 2b shows the mean difference between black and white patient in viral control (and 95% CI for the difference) for the same models. Before any adjustment, there was a 6.9% absolute difference in uncontrolled viral load between black and white patients (14.9% vs. 8.0%). Controlling for only the clinic reduced the difference in viral control between black and white patients to 5.1% absolute difference—suggesting that site of care accounted for 26% of the difference in viral control between black and white patients. Retention in care accounted for only 3% of the racial difference in viral control. cART adherence was the strongest single mediator, accounting for 51% of the difference between black and white patients.
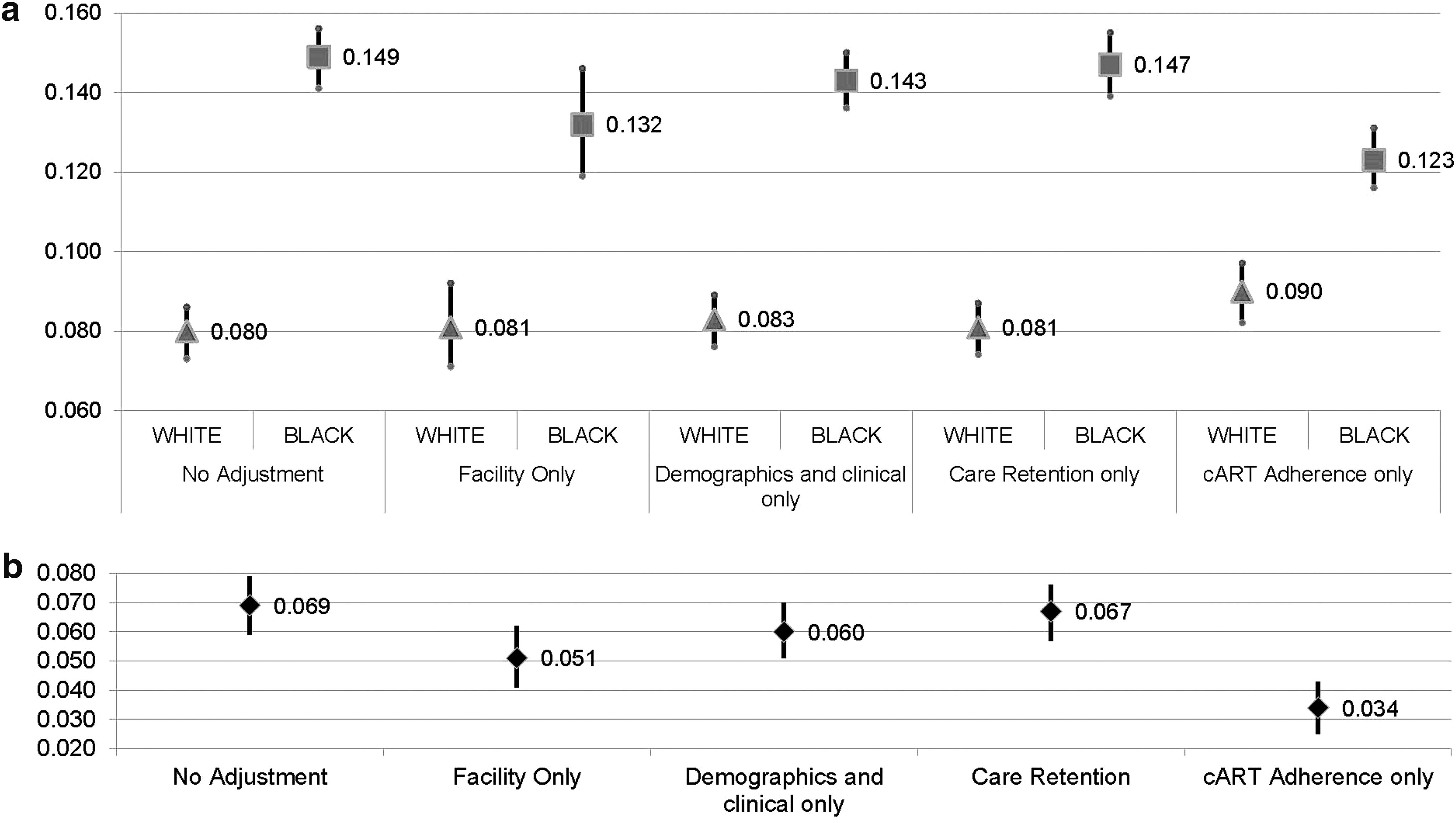
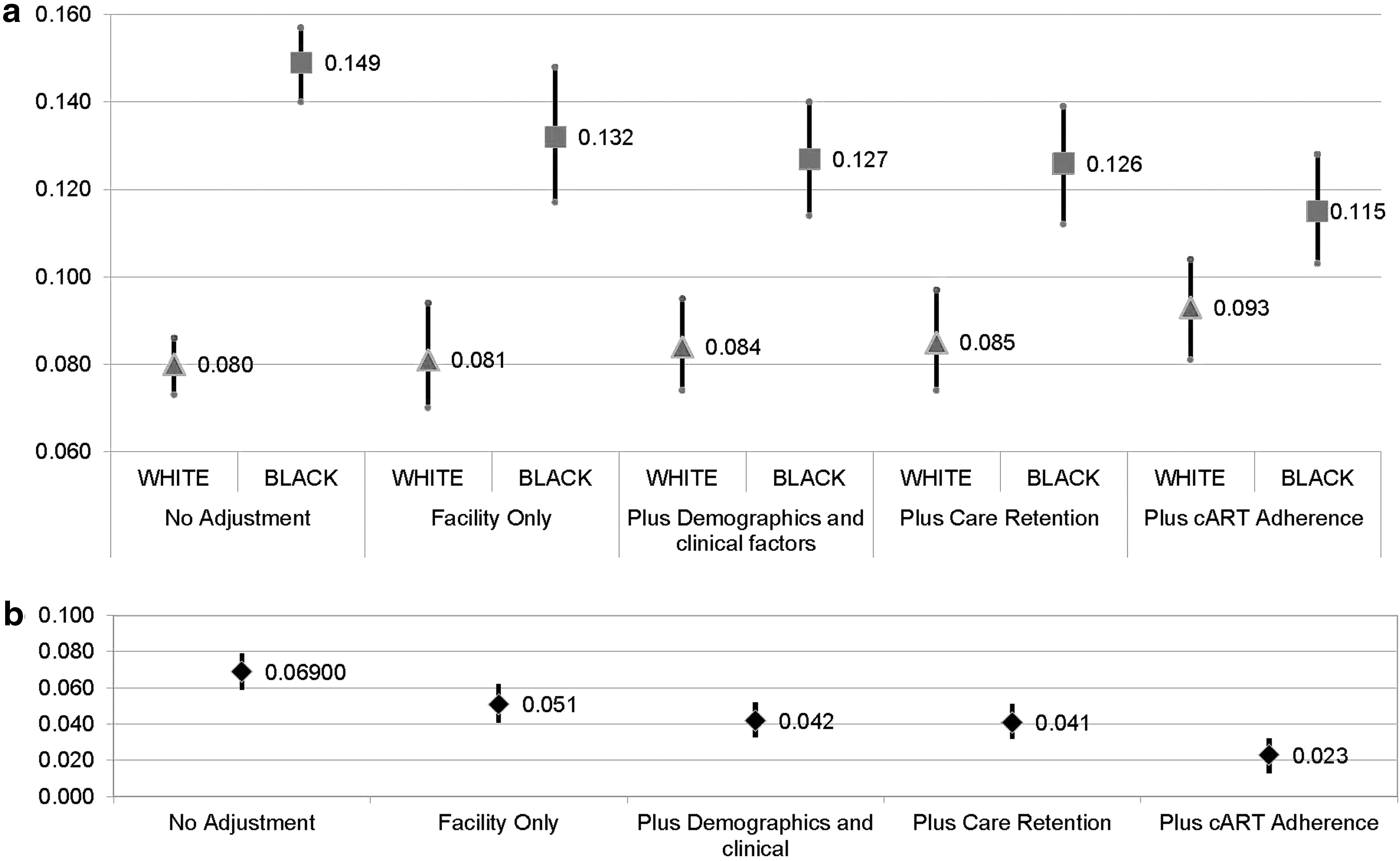
Figure 3a and b shows information that is similar to Fig. 2a and b, except that potential mediators are added sequentially to models. While Fig. 2a and b demonstrates that cART adherence alone accounted for 51% of the difference in viral control between black and white patients, Fig. 3a and b demonstrates that cART adherence, retention in care, demographic and clinical characteristics, and clinic combined account for 67% of the difference between black and white patients. In fact, after controlling for all potential mediators, a small statistically significant difference between black and white patients remains (3.4% absolute difference).
Discussion
Disparities in HIV care outcomes between black and white patients have been well documented. This study evaluated key correlates of racial disparities, to offer potential explanations of disparities and guide efforts to eliminate or reduce disparities. Using a national cohort of veterans in HIV care at the VHA, we found that differences in adherence to antiretroviral medications explained more than half of the difference in viral control between black and white persons in care for HIV. The clinic where HIV care occurred was also an important factor, explaining more than one-fourth of the disparity. Differences in retention in care, demographics, and clinical characteristics contributed less to racial disparities.
More than a decade ago, Kilbourne et al. 31 provided a framework for addressing racial disparities that encompasses three distinct phases as follows: (1) detection and document (i.e., identify and measure disparities); (2) understand (i.e., identify factors that explain gaps in care and outcomes between patient groups); and (3) develop, implement, and evaluate interventions to reduce or eliminate disparities. Substantial prior studies have documented racial disparities in HIV-related outcomes, including RNA control. 5,9,13 This study addresses the second phase of the framework by improving our understanding of factors that create or exacerbate disparities in RNA control for HIV-infected individuals. To date, few studies have attempted to explain underlying causes of disparities in HIV care and outcomes. One prior study by Beer et al. 32 used data from the Medical Monitoring Project (MMP) and found that differences in ART use and adherence, demographics, and social determinants of health account for a significant portion of disparity in viral suppression between white and black men—roughly half the difference in their study. Our study builds on this prior work by addressing some of the limitations in the MMP. First, the MMP is derived from a sample of facilities providing HIV care in the United States, and only 50% of patients from the sampled facilities responded to invitations to participate in the MMP. In contrast, the current study includes all black and white patients with HIV receiving care in the VA health system who used cART. Second, the measure of cART use and adherence in the MMP is self-reported and only reflects the 3-day period before the MMP interview. Thus, patients are categorized either as adherent (i.e., all required cART doses taken during past 3 days) or not adherent. Our study measures cART adherence over an entire year before the viral load measurement and reflects actual cART refill patterns. The study by Beer et al. also did not evaluate the role of care sites in explaining racial disparities. Nevertheless, the fact that both studies demonstrated the primary importance of cART adherence in explaining racial differences in HIV outcomes is compelling.
The finding that cART adherence is the primary mediator for differences in viral control by race has important implications for clinical care and for the third phase of the health disparity framework by Kilbourne et al. Multiple studies have shown that engagement in care and adherence are impacted by patients' experiences of racism, conspiracy beliefs, or mistrust of the provider or medical system. 33 This points to the importance of physician cultural competence in improving outcomes for black patients with HIV. Physicians may improve adherence among minorities by sharing decision-making with patients, discussing patients' beliefs and fears, and making treatment decisions transparent. Notably, interventions to improve patient–physician communication have shown promise in improving medication adherence, 34 although the effectiveness of these interventions within specific minority populations in not known. Other interventions that may be effective at improving adherence, particularly for individuals with known adherence challenges, include the use of memory aids, counseling support, and support group participation. 35
This study also documents the role that the treating clinic plays in racial disparities. Studies of other diseases, including cancer, 17 diabetes, 36 and cardiovascular disease, 18 have demonstrated that disproportionate use of low quality providers by black populations accounts for at least a portion of the disparity in health outcomes. Saha et al. 21 also concluded that, within the VA, differences in facilities attended by different racial groups at least partially explain disparities in outcomes. In our study, the use of different facilities by black and white patients is the second strongest mediator of racial differences in viral control, after controlling for differences in cART adherence. Some of this difference across facilities may reflect differences in neighborhoods surrounding facilities that are attended by black and white patients. 9 However, we did not find significant differences in mean patient income in ID clinics where black patients were treated compared to ID clinics where white patients were treated. Moreover, in previous analyses, neighborhood social disadvantage did not substantially explain racial disparities in viral control, after controlling for facility and patient clinical characteristics. 22 Other differences, such as differences in clinic resources and clinical team structures across ID clinics, may also contribute to racial disparities. For example, clinics with integrated social workers, mental health specialists, and substance use clinicians may be better able to address patient-level issues contributing to disparities. There may also be difference in attitudes and communication styles that are shared across providers in clinics with varying cultures of care, which can contribute to disparities. Efforts to standardize the quality of HIV care across care sites, including improving cART adherence across sites, may help to reduce racial disparities in care. Understanding the patterns of care, extent of cultural tailoring of care, and level of provider cultural competence at lower performing sites would provide greater insight into site level variation. Possible interventions to reduce site-level variation might include a peer-mentoring program joining higher and lower performing sites in an effort to improve HIV outcomes.
This study has limitations. First, the study includes few women due to the small numbers of women who receive care in the VA, possibly limiting generalizability of our results to patients outside the VA. Moreover, VA patients with HIV are significantly older than individuals with HIV in the general population. For example, 47% of white men and 40% of black men in the MMP data were over the age of 50, compared to 75% and 78% in our cohort, respectively. 32 Second, our measure of cART adherence is calculated based on cART refill patterns and may not reflect the actual use of medications when prescriptions are filled. Third, measurement of patient comorbidities is based on ICD-9-CM diagnosis codes which may be subject to incomplete or erroneous coding. Fourth, we used a measure of retention in care based on the constancy of completed visits. Other retention in care measures exists based on frequencies of completed and missed clinic visits and may have captured different information about the role of retention in care. 37 Fifth, there are known inaccuracies with respect to the capture of race and ethnicity in administrative data. VA collects information on patient race primarily from the VA enrollment form, which may be completed online, by mail, or in person, and therefore usually reflects the patient's identification. A previous study demonstrated a high level of concordance between VA race and race reported on Medicare enrollment files for white veterans (99% agreement) and African Americans (96% agreement). 27
Our findings suggest that even in an integrated healthcare system such as the VHA, where all patients have equal access to care, disparities persist and may be attributable to differences in the site of care, as well as patient adherence to cART. Efforts to reduce racial disparities in care should focus on interventions to improve antiretroviral adherence and target quality improvement efforts to reduce variation in viral control across care sites.
Footnotes
Acknowledgments
The work reported in this study was supported by the Department of Veterans Affairs, VHA, Health Services Research and Development (HSR&D) program (HSR&D IIR 12-285). Dr. Ohl is recipient of a career development award from VA HSR&D. All authors had access to the data and participated in the design and writing of the article.
Author Disclosure Statement
No competing financial interests exist.