
Abstract
Methamphetamine use is a key driver of HIV transmission among men who have sex with men (MSM). We evaluated trends in incident HIV diagnosis rates among methamphetamine using and nonusing MSM and assessed the relationship between methamphetamine use and demographic, behavioral, and clinical characteristics among MSM newly diagnosed with HIV. We analyzed several sources of HIV and behavioral surveillance data to estimate incident rates of HIV diagnoses and the population attributable risk percent corresponding to methamphetamine use among MSM in King County, Washington. Missing values were recovered through multiple imputation. We report descriptive statistics and adjusted odds ratios yielded from multivariable logistic regression models. Between 2010 and 2015, the HIV diagnosis rate among methamphetamine-using MSM declined from 31.2 to 11.5 per 1000 MSM (vs. 6.4–3.9 per 1000 MSM overall), and the percent of new diagnoses attributable to methamphetamine use declined from 25% to 13%. During the same period, methamphetamine use among HIV-negative MSM remained relatively stable. Among MSM newly diagnosed with HIV, methamphetamine-using MSM were more likely to be unstably housed (24% vs. 6%), to have engaged in transactional sex (19% vs. 4%), and to have had female partners (17% vs. 10%). Methamphetamine-using MSM were less likely to be virally suppressed at 6 (31% vs. 54%) and 12 (59% vs. 73%) months following an HIV diagnosis. The declining HIV diagnosis rate among methamphetamine-using MSM is encouraging, but this subgroup continues to have considerable HIV risk and health disparities.
Introduction
A
The contribution of methamphetamine to HIV transmission is geographically heterogeneous. Globally, methamphetamine plays a key role in HIV transmission in Eastern Europe and some Asian countries. 13 In the United States, methamphetamine use among urban MSM has traditionally been concentrated along the West Coast. 14 However, a recent report described a substantial increase among African American MSM in Washington, DC. 15 In our local jurisdiction, where MSM comprise over three-quarters of people living with diagnosed HIV (PLWDH), 54% of methamphetamine-injecting MSM who participated in the 2014 Seattle National HIV Behavioral Surveillance (NHBS)—MSM Cycle tested positive for HIV, considerably higher than the prevalence of 17% measured for the entire sample. 17 Longitudinal data from Seattle's STD Clinic suggest that methamphetamine use is the strongest predictor of future HIV acquisition. 16
Seattle-King County has excellent HIV care continuum outcomes relative to the national average. The percent of PLWDH who were virally suppressed increased from 45% in 2007 to 82% in 2016. In 2016, King County became one of the first jurisdictions to achieve the 90-90-90 goal (e.g., 90% diagnosed, 90% on treatment, 90% virally suppressed). The recent increases in viral suppression among those with HIV may influence the relationship between methamphetamine use and HIV acquisition. As early uptake of antiretroviral therapy (ART) has become widespread, it is plausible that the contribution of methamphetamine to HIV rates among MSM has decreased. On the contrary, if HIV-infected MSM who use methamphetamine have lower levels of viral suppression, the role of methamphetamine may have intensified. To our knowledge, population attributable risk (PAR) of HIV acquisition associated with methamphetamine use has only been measured in a research cohort. 19 Our HIV surveillance program uniquely captures data about methamphetamine use at time of HIV diagnosis, making it possible to estimate PAR using population-based data sources.
We triangulated Public Health—Seattle & King County HIV surveillance data to: (1) estimate the prevalence of methamphetamine use among HIV-negative and HIV-positive MSM in King County, (2) estimate the magnitude of excess risk of an incident HIV diagnosis among methamphetamine-using MSM, (3) compare key characteristics of methamphetamine-using and nonusing MSM who are newly diagnosed with HIV, and (4) compare time to viral suppression by methamphetamine use status at the time of HIV diagnosis.
Methods
Data sources
Table 1 summarizes the data sources analyzed, including how each data source assessed male-to-male sexual behavior and methamphetamine use. Our analysis relied heavily on King County HIV Surveillance and Partner Services data. Washington State law requires that healthcare providers report all new HIV and AIDS diagnoses by name and that laboratories report tests confirming HIV infection, HIV viral load (detectable and undetectable), and CD4+ T lymphocyte test results of any value by name. 20 These reports are matched against existing surveillance records to identify cases “new” to King County. Each “new” case is investigated to determine whether the case moved to King County after being diagnosed elsewhere or if the case was newly diagnosed in King County. This analysis is restricted to cases newly diagnosed in King County. Information about risk behaviors uncovered through case investigations, including male-to-male sexual behavior and methamphetamine use, is documented in surveillance records. King County reaches about 80% of newly diagnosed HIV cases to assist with linkage to care and discuss partner notification. During the partner services interview, cases are asked explicitly about methamphetamine use and gender of sex partners. For this analysis, information about sexual behavior with male partners and methamphetamine use in the past year was summarized across surveillance records and partner notification interview data. If the case did not participate in the partner services interview and surveillance records did not contain information about male-to-male sexual contact and/or methamphetamine use, they were assigned missing values for these behaviors.
Described in the Methods section.
MMP, Medical Monitoring Project; MSM, men who have sex with men; PS, Partner Services; STD, sexually transmitted disease.
In addition to HIV surveillance records and partner services interview data, we also examined methamphetamine use among MSM in four additional data sources (described in Table 1). We assessed data from the Medical Monitoring Project (MMP), a CDC-funded project designed to monitor health indicators in a sample representative of the HIV care patient population. 21 We used three data sources to estimate methamphetamine use among HIV-negative MSM: NHBS, annual Pride Surveys, and STD Clinic client intake forms. Every 3 years, NHBS uses venue-based sampling to recruit MSM to complete a one-time, 60-min, interviewer-administered survey and to undergo HIV testing. 22 The Pride Survey is a serial, cross-sectional, 10-min, self-administered survey conducted annually at the Seattle Pride Parade. 18 The STD Clinic intake form is a 10-min computer-assisted self-administered survey completed by patients attending the Public Health STD Clinic that is linked to HIV test results. 23 After restricting these data sources to MSM who had not been previously diagnosed with HIV (hereafter referred to as “HIV negative”), we estimated the annual prevalence of methamphetamine use in 2010–2015 among Pride Survey participants and STD Clinic patients and methamphetamine prevalence among MSM who participated in the 2011 and 2014 NHBS cycles.
Finally, to estimate the total number of MSM in King County during each year of the analysis, we obtained King County population estimates from the Washington State Office of Financial Management, which applied a model that uses iterative proportional fitting to allocate Census 2010-modified age–race–sex data at the county level to generate population estimates in postcensal years. 24 To estimate the number of MSM in King County, we multiplied the number of King County male residents by 5.7%, our estimate of the proportion of male King County residents who are MSM, derived from a population-based survey. 25
Analysis
Multiple imputation
After limiting the analytic data set to people assigned male at birth and triangulating data from HIV case reports and partner services interviews, 4% of newly diagnosed male cases were missing values for male-to-male sexual contact and 14% were missing values for methamphetamine use. We assumed that data were missing at random—that is, missingness was conditional only on the variables included in the imputation model: age at diagnosis, race, ethnicity, US or foreign born, year of diagnosis, facility at diagnosis, subregion of King County at diagnosis, risk transmission category, time between diagnosis and viral suppression, HIV-only or concurrent HIV/AIDS diagnosis, moved out of Washington since diagnosis, death following HIV diagnosis. We used IVEware version 0.2, an SAS-callable macro, to perform multiple imputation by chained equations (MICE; also called “sequential regression multivariate imputation”). 26 MICE formulates separate regression models for each variable with missing data and uses regression appropriate for the variable type (e.g., linear regression for continuous variables and logistic regression for dichotomous variables). We imputed 10 data sets and estimated the mean point estimates across the 10 imputed data sets. Standard error was calculated using Rubin's rules. All statistics describing MSM newly diagnosed with HIV were generated by the MICE models.
Estimated prevalence of past-year methamphetamine use
We estimated the prevalence of methamphetamine use, stratified by year, in five different data sources. The prevalence of methamphetamine use among MSM newly diagnosed with HIV was estimated through MICE models (as described above). The prevalence of methamphetamine use among MSM in HIV care who participated in the MMP in 2009–2015 was weighted for probability of selection and nonresponse.
Methamphetamine use among HIV-negative MSM was assessed in three data sources: NHBS, STD Clinic Intake Forms, and the Pride Survey. To improve the comparability across data sources, we estimated the age-standardized prevalence of methamphetamine use, with the underlying age distribution of the male King County population serving as the standard population.
Measures of excess risk
To estimate the number of MSM who are not diagnosed with HIV, we subtracted the number of prevalent MSM diagnosed with HIV and presumed living in King County from the estimated number of MSM in King County (estimated to be 5.7% of the male population 25 ). After estimating the prevalence of methamphetamine use in the three data sources of HIV-undiagnosed MSM (described above), we discovered that methamphetamine use in this population was fairly constant in 2010–2015, and it was highest in the NHBS sample and lowest in the Pride Survey Sample. Ultimately, we decided to apply the midpoint estimate of methamphetamine prevalence generated by the three data samples of HIV-undiagnosed MSM (e.g., MSM who completed an STD Clinic intake form), averaged across 2010–2015, to the number of HIV-undiagnosed MSM in King County; these estimates served as the denominator for the annual incident rates for methamphetamine using and nonusing MSM in King County.
We report three measures of excess risk associated with methamphetamine use:
The RR describes the HIV incidence rate among methamphetamine using MSM relative to nonmethamphetamine using MSM. The AR percent describes the proportion of HIV incidence among methamphetamine-using MSM, attributable to methamphetamine use. The PAR percent describes the proportion of HIV incidence among all MSM, attributable to methamphetamine use.
Correlates of methamphetamine use among newly HIV-diagnosed MSM
We assessed correlates of methamphetamine use among MSM newly diagnosed with HIV using IVEware's “Impute-Describe” procedure, which generated row and column percentages, and “Impute-Regress” procedure. This procedure implements logistic regression on imputed data sets; the exponentiated mean β-coefficient across the ten data sets serves as the odds ratio and the corresponding standard error (and thus confidence intervals) is estimated using Rubin's rules. Variables available for all new cases (e.g., age at diagnosis, race/ethnicity, year of diagnosis, facility of diagnosis, and whether concurrently diagnosed with AIDS) were assessed using the entire data set of newly diagnosed cases. Variables only assessed for cases who completed a partner notification interview (e.g., housing status at time of diagnosis, any recent female sex partners, number of recent male partners, ever engaged in transactional sex, ever injected drugs, and recent use of crack, cocaine, heroin, erectile dysfunction drugs, and amyl nitrates) were assessed in a data set limited to cases who completed a partner notification interview. Odds ratios were adjusted for age, sex, race/ethnicity, and year of diagnosis. We also report the percent of methamphetamine using and nonusing MSM newly diagnosed with HIV who achieved HIV viral suppression within 6, 9, and 12 months of diagnosis.
All analyses were undertaken as a public health surveillance activity and therefore did not require institutional review board review.
Results
Prevalence of past-year methamphetamine use among King County MSM
Between 2010 and 2015, 1280 men were diagnosed with HIV in King County, of whom 1149 (90%) were MSM. The prevalence of methamphetamine use among MSM newly diagnosed with HIV declined from 30% in 2010 to 18% in 2015. In all other data sources, the prevalence of methamphetamine use was more stable over time among MSM (Fig. 1). In this 5-year period, the prevalence of methamphetamine use in the past 12 months among MSM in HIV care ranged between 14% and 19%. Among HIV-negative MSM, the 5-year average age-standardized prevalence of methamphetamine use was 11% among MSM who participated in NHBS, 6% among MSM who completed an STD Clinic intake form, and 4% among MSM who completed a Pride Survey.
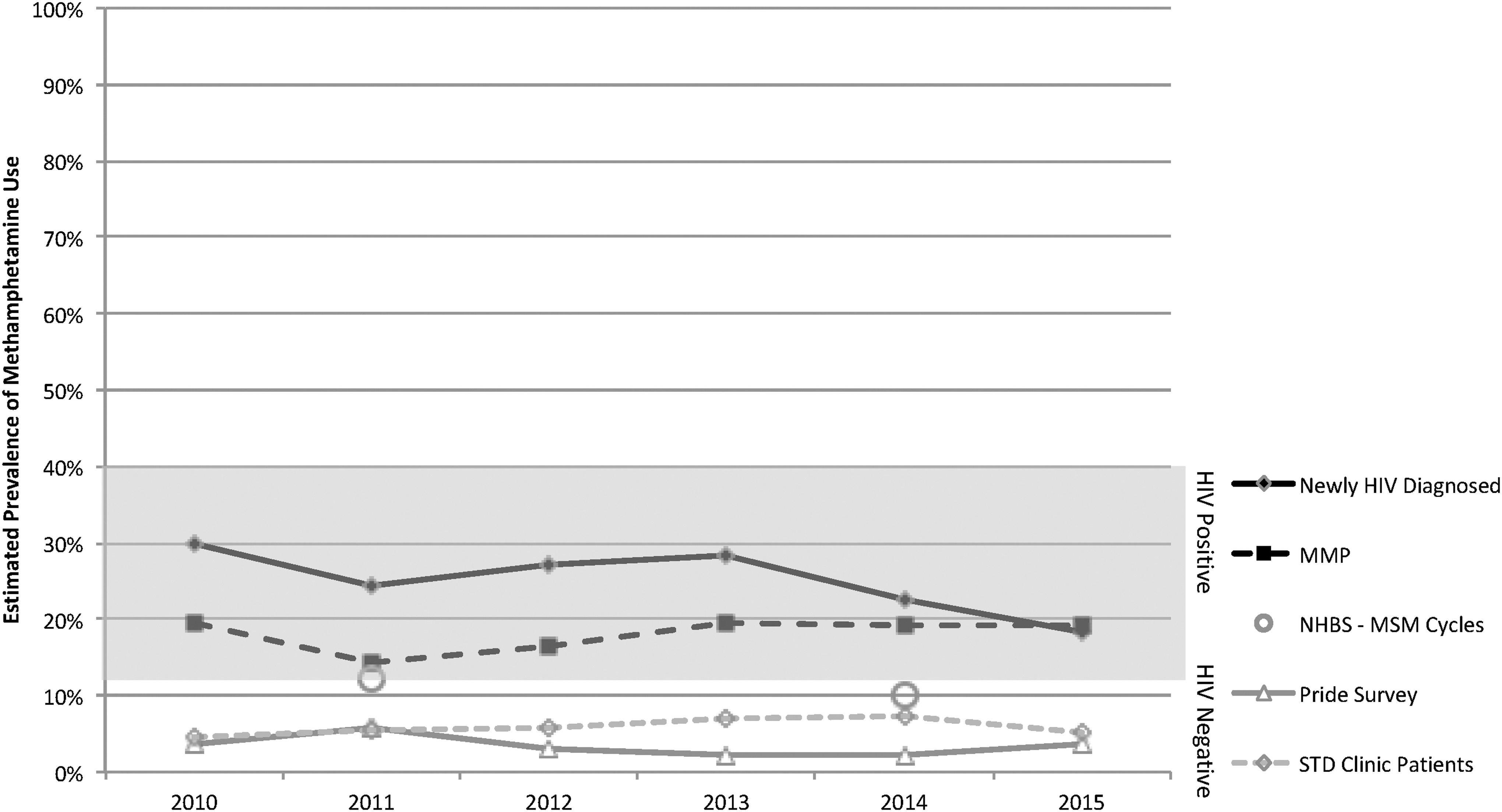
Estimated trends in methamphetamine use in HIV-positive and HIV-negative men who have sex with men in King County, WA. This figure summarizes data across five data sources, all restricted to MSM. The gray bar highlights trends in the estimated prevalence of methamphetamine use among people with diagnosed HIV: newly diagnosed with HIV (derived from Core Surveillance and Partner Services) and HIV care patients (derived from the Medical Monitoring Project). Estimates of methamphetamine use among HIV-negative MSM are presented with a white background and were obtained from the National HIV Behavioral Surveillance program, the Pride Survey, and STD Clinic Intake Forms. To facilitate comparison across these three sources and to improve their representativeness of the underlying population of HIV-negative MSM, we adjusted these estimates for age using direct standardization with the King County male population (derived from the US Census Bureau) serving as the standard population. MSM, men who have sex with men; STD, sexually transmitted disease.
Magnitude of excess risk of an incident HIV diagnosis among methamphetamine-using MSM
The incidence rate of a new HIV diagnosis declined from 6.4 per 1000 MSM to 3.9 per 1000 MSM between 2010 and 2015 (Table 2 and Fig. 2). Among methamphetamine-using MSM, HIV diagnosis incidence rate declined from 31.2 in 2010 to 11.5 per 1000 in 2015. The RR of an HIV diagnosis comparing methamphetamine using to nonmethamphetamine using MSM was 6.48 in 2010 and 3.39 in 2015. Among methamphetamine-using MSM newly diagnosed with HIV, the proportion of incidence attributable to methamphetamine use declined from 85% in 2010 to 71% in 2015. Between 2010 and 2015, the PAR percent (i.e., the percent of all new HIV diagnoses among MSM attributable to methamphetamine use) declined from 25% to 13%.
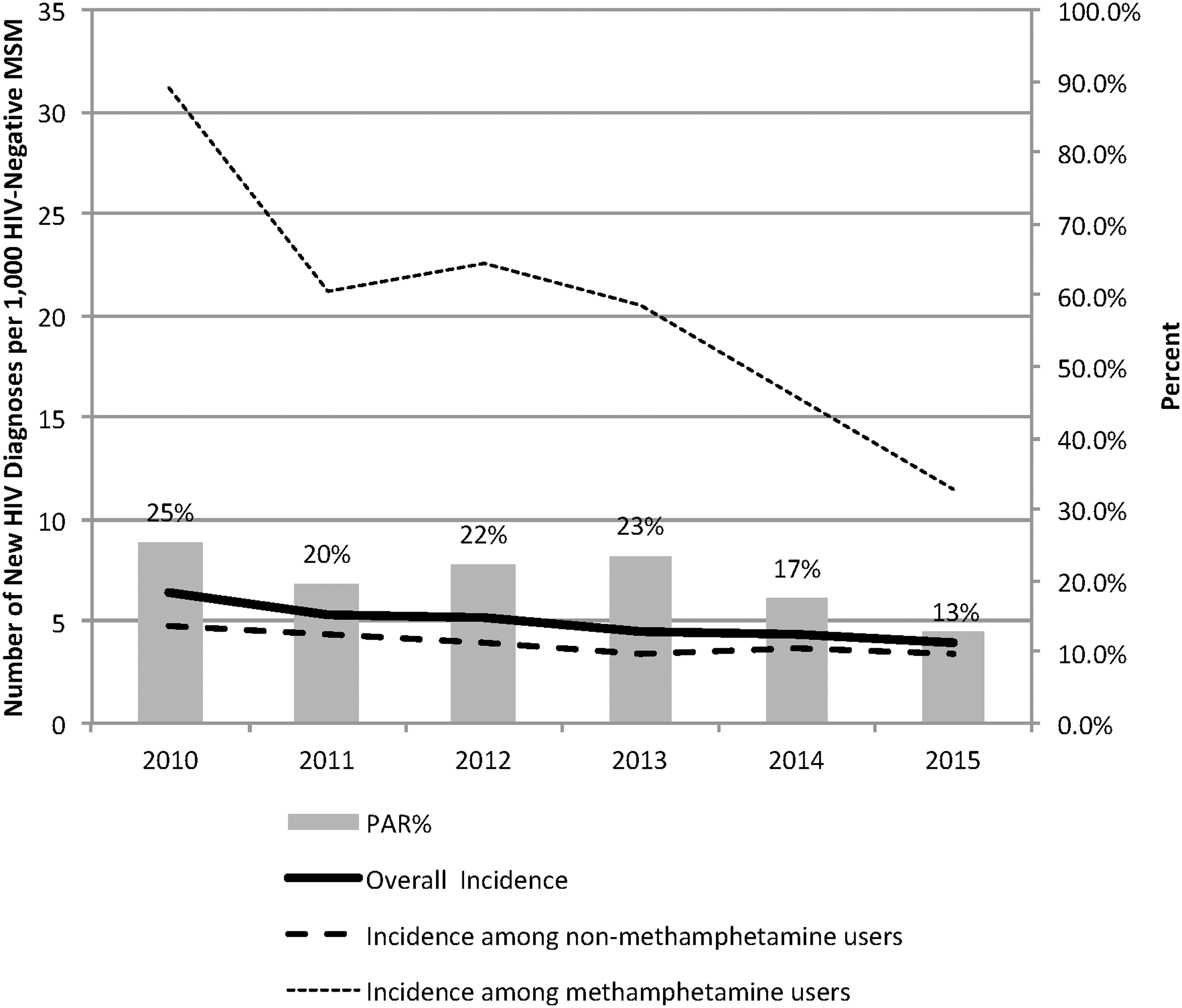
Estimated incidence of a new HIV diagnosis and percent of new HIV diagnoses attributable to methamphetamine use among men who have sex with men in King County, WA, 2010–2015.
Source: Behavioral Risk Factor Surveillance System Survey Data. 23
Source: PHSKC STD Clinic Intake Forms.
Refers to methamphetamine use in the last year.
AR, attributable risk; MSM, men who have sex with men; PAR, population attributable risk; STD, sexually transmitted disease.
Demographic, behavioral, and clinical characteristics of methamphetamine-using MSM newly diagnosed with HIV
Between 2010 and 2015, the percent of newly diagnosed MSM who used methamphetamine declined over time; by 2014, the odds of being a methamphetamine user were significantly less than what they had been in 2010 (Table 3). Compared with non-Hispanic white MSM, Hispanic MSM were significantly less likely to be methamphetamine users. MSM diagnosed at an emergency room or at the Public Health STD Clinic were more likely to be methamphetamine users than MSM diagnosed in other outpatient clinics. Neither age nor a concurrent AIDS diagnosis was significantly associated with methamphetamine use.
Methamphetamine use estimated with multiple imputation.
Odds ratios are adjusted for all of the variables included in this table.
Data not shown for “other” or “missing” categories.
AIDS diagnosis within 1 year of HIV diagnosis.
p ≤ 0.05; ** p ≤ 0.01.
aOR, adjusted odds ratio; CI, confidence interval; MSM, men who have sex with men; STD, sexually transmitted disease.
Among newly diagnosed MSM who participated in a partner notification interview, methamphetamine users were more significantly more likely to be unstably housed (24% vs. 6%), have ≥10 recent male sex partners (44% vs. 21%), have female partners (17% vs. 10%), engaged in transactional sex (19% vs. 4%), injected drugs (37% vs. 4%), and used other drugs besides methamphetamine (Table 4). Methamphetamine using MSM, especially those without stable housing, were less likely to be virally suppressed at 6, 9, and 12 months following an HIV diagnosis (Fig. 3).
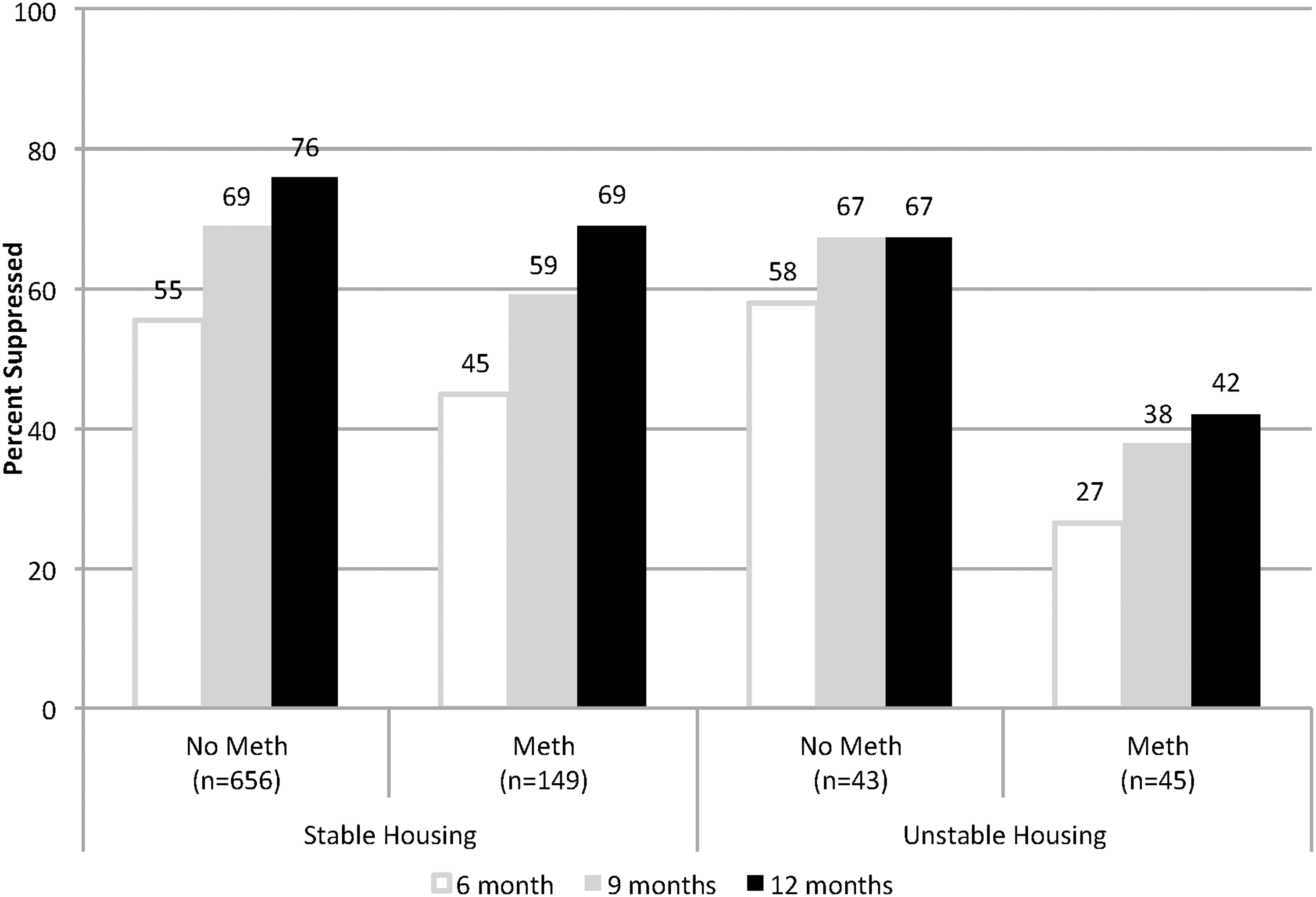
Percent of methamphetamine using and nonusing MSM (n = 1155) who achieved viral suppression within 6, 9, and 12 months of HIV diagnosis, King County, WA, 2010–2015. MSM, men who have sex with men.
Odds ratios are adjusted for age, race, year of HIV diagnosis, whether a concurrent HIV/AIDS diagnosis.
p ≤ 0.0001; † p ≤ 0.01; ‡ p ≤ 0.001.
aOR, adjusted odds ratio; CI, confidence interval.
Discussion
In this analysis of methamphetamine and HIV trends in King County, Washington, during 2010–2015, we found that methamphetamine use remained stable among MSM overall, but that the HIV diagnosis rate declined considerably among methamphetamine using MSM. Along with that decrease, the population attributable fraction of methamphetamine (the percent of new cases attributable to methamphetamine use) declined from 25% to 13%. This finding parallels the decline in new HIV diagnoses observed in the general population in King County, which occurred concomitant with increasing rates of viral suppression among people living with HIV (PLWH). 27 Without evidence that methamphetamine use is declining among King County-MSM, increases in viral suppression (and thus decreases in infectiousness) at the population level may be one of the drivers of the observed decline in HIV diagnosis rates among methamphetamine using MSM.
Even with the decline in incidence, methamphetamine using MSM were still more than three times as likely as nonmethamphetamine using MSM to be diagnosed with HIV in 2015. Similar to the existing literature, our findings highlight substantial ongoing risk for HIV among methamphetamine using MSM, and a social and structural context that might facilitate HIV acquisition and hinder HIV care engagement and treatment adherence among methamphetamine users. Among newly diagnosed MSM, methamphetamine users were three times as likely to be homeless or unstably housed and nearly four times as likely to have been involved in transactional sex. These factors almost certainly reflect a higher prevalence of many other factors such as untreated mental illness, criminal justice involvement, and a history of early life trauma that are not measured in surveillance data but significantly impact HIV care engagement and health outcomes. 9 Indeed, fewer methamphetamine using MSM relative to nonusing MSM attained viral suppression in the year following an HIV diagnosis.
Similar to national estimates from NHBS, the prevalence of methamphetamine use among King County MSM appeared to remain stable between 2010 and 2015 and was greater among HIV-positive than HIV-negative MSM. Our results confirm the well-known association between methamphetamine use and HIV risk, but provide a view of the change in risk over time. 5,19,28 –32 Our characterization of the social and structural context in which methamphetamine-using MSM acquired HIV is consistent with previous findings 9 and, in addition, quantifies the risk in the period immediately preceding an HIV diagnosis.
Ensuring that methamphetamine using MSM are linked to and retained in HIV medical care and appropriate supportive services is crucial for improving the health of individual methamphetamine-using MSM and their potential sexual and drug sharing partners. Interventions could include intensive efforts at the time of diagnosis to simultaneously connect persons with HIV medical care, medical case management, supportive housing services, and intensive ART initiation and adherence support. For HIV-diagnosed persons with extensive barriers to HIV care and medication adherence, alternative models for HIV care might be needed. For example, in King County, we established the MAX Clinic to serve patients who have not been able to stay engaged in traditional HIV care; this clinic offers walk-in visits and incentives to enrolled patients, the majority of whom use methamphetamine.
There are limitations to our analysis. It relied heavily on self-reported methamphetamine use—a variable susceptible to social desirability bias. The estimated prevalence of methamphetamine use among HIV-negative MSM was based on STD Clinic data, which served as a midpoint between two other samples considered to be disproportionately comprising high-risk (e.g., NHBS data) and low-risk (e.g., Pride Survey) MSM. We recognize that MSM attending the Public Health STD Clinic are not representative of the underlying MSM population; however, in the absence of truly population-based data, we considered this data source as the best option for approximating methamphetamine use among HIV-negative MSM. Much of our article focused on incident HIV diagnoses, since ascertaining incident HIV infections was infeasible. The denominator in these rates was estimated by applying the percent of men who engage in male-to-male sexual behavior (derived from the Washington State Behavioral Risk Surveillance Survey) to King County population estimates (derived from the census). Although this is an imperfect estimate of the denominator, any bias affecting the validity of the estimate was likely constant over time. The numerator (e.g., number of new diagnoses), however, could have been influenced by programmatic changes, such as testing initiatives and data collection procedures. We used MICE to recover missing values for methamphetamine use and male-to-male sexual behavior among people newly diagnosed with HIV. Although we included many demographic and clinical variables in our imputation models, it is unlikely that we fully accounted for all factors that would affect missingness, compromising the “missing at random” assumption that underlies this statistical approach.
In summary, we found that despite stable trends in methamphetamine use in the underlying MSM population, HIV diagnosis rates declined considerably among methamphetamine-using MSM 2010–2015. Nonetheless, HIV-diagnosis rates were considerably higher among methamphetamine users than nonusers in all years; and newly diagnosed methamphetamine using MSM experienced delays in attaining viral suppression. MSM who use methamphetamine may be benefitting from population-level increases in viral suppression among PLWH, but will also need additional tailored interventions to achieve full health equity.
Footnotes
Author Disclosure Statement
J.C.D. has conducted research supported by grants to the University of Washington from Hologic, Curatek, and Quidel.