
Abstract
We examined care engagement and viral suppression (VS) over a 1- to 5-year period among persons re-engaged in HIV care using retrospective cohort study and longitudinal follow-up. The population comprised five cohorts of persons re-engaged in care from 2009 to 2013. We used surveillance data [CD4 T cell count or HIV viral load (VL) RNA] to measure four outcomes 1–5 years post-care engagement. Engagement-in-care indicated persons with laboratory reports in each follow-up year. Continuous engagement or sustained engagement, respectively, included persons with ≥1 or ≥2 (separated by 90 days) CD4 or VL reports in each follow-up year. VS indicated persons living with HIV (PLWH) re-engaged in care with VL ≤200 copies/mL in any follow-up year, and we measured re-engaged PLWH who subsequently became out of care (OOC) in each follow-up year. Overall, 84–86% PLWH were engaged in care in any follow-up year. The proportions of PLWH cohorts continuously engaged in care [86% (1 year), 77% (2 years), 72% (3 years), 67% (4 years), and 63% (5 years)] declined over time. Thirty-four percent of the PLWH who were re-engaged in care were subsequently OOC in the follow-up years. Most re-engaged PLWH became OOC in their first (40%) and second (30%) follow-up years. In follow-up years (1–5 years), fewer PLWH continuously engaged in care with ≥1 CD4 or VL reports in the registry had VS ≤200 copies/mL: 65%, 58%, 49%, 44%, and 42%, respectively. Encouragingly, higher proportions had VL ≤1500 copies/mL in follow-up years (1–5): (75%, 72%, 73%, 75%, and 70%), likely reflecting levels of HIV treatment. Our results support the use of surveillance data to identify and re-engage OOC PLWH in care. However, structures and programs are needed to support retention in care and reduce repeat OOC.
Introduction
U
Being out of HIV clinical care [out of care (OOC)] is a significant barrier to the treatment of persons living with HIV (PLWH) worldwide. 11 –13 HIV case management programs, including patient navigation and care coordination programs, designed to promote adherence to HIV care and treatment, have been shown to have moderate to profound effects on engaging and retaining PLWH in care. 14 –17 However, because these programs often operate within clinical settings, the benefits are conferred only to persons already known to clinical providers and current with HIV care.
In recent years, local health departments have implemented routine or demonstration projects known as “Data-to-Care.” Using the HIV surveillance registry to identify PLWH presumed to be OOC because they lack recent HIV-related laboratory reports (i.e., CD4 T cell count or VL ordered by clinical providers), public health case workers, or patient navigators trace the OOC-PLWH with the objective of facilitating their re-engagement in care once found. 18 –21 While these Data-to-Care programs have demonstrated varying degrees of success in locating and re-engaging PLWH previously OOC back to HIV care, little information is available about the levels of engagement and sustained engagement in the care of PLWH in the years post their re-engagement in care.
The NYC Department of Health and Mental Hygiene (DOHMH) implemented a Data-to-Care initiative in 2007. 19 The aim of our analyses was to use data from the NYC HIV Surveillance Registry to evaluate rates of engagement and continuous engagement in care, and VS of OOC-PLWH who were re-engaged in care as part of the Data-to-Care initiative. We also examined potential factors associated with continuous engagement in care and subsequently becoming OOC among our study population.
Methods
The NYC-DOHMH Data-to-Care program
As described in detail elsewhere, 19 NYC DOHMH Field Services Unit (FSU) case workers use the NYC HIV surveillance registry (hereafter, referred to as “the registry”) to identify PLWH presumed to be OOC for follow-up under the Data-to-Care initiative. A laboratory report of CD4 or VL in the registry is used as a proxy for receipt of clinical care. 22 PLWH are presumed OOC if they have no laboratory reports in the ≥9 months before selection for follow-up.
During the reporting period, two to three DOHMH public health case workers were designated to trace OOC-PLWH and facilitate their re-engagement in HIV care. Each case worker was assigned up to 20 PLWH presumed OOC each month. The case workers used an array of social service delivery and Internet-based subscription databases to confirm locating information (e.g., telephone number, residential address) found in the registry or obtained through provider report, or to identify alternate contact information. Contact attempts were made through letters, telephone calls, and field visits to PLWH presumed OOC. If contacted, PLWH were interviewed to confirm their care status and to identify reasons for being OOC (e.g., lacking health insurance coverage, feeling well and not seeing need for HIV care, or other personal or economic barriers). Based on the reasons identified for OOC, case workers worked with PLWH to identify and secure appointments with the most suitable HIV and social service providers.
Data sources and study population
We used data from two sources for our analysis: the FSU database and the registry. The FSU database is a case management database for tracking the activities and outcomes of case workers' efforts to trace and re-engage OOC-PLWH to care. The activities tracked include but are not limited to: case assignment, contact attempts (e.g., telephone calls, field visits, care appointments, PLWH responses to case worker contact attempts and care appointments, dates of activities), and outcomes (e.g., linked to care, refused re-engagement in care).
The NYC population-based registry contains information on all persons diagnosed with AIDS in NYC since 1981 and HIV since 2000, and is continuously updated with incoming matched HIV-related laboratory results, which since 2005 have included CD4 T-cell counts, VL results, nucleotide sequences from HIV genotypes, and positive HIV detection tests. Vital status for PLWH in the registry is updated through quarterly matches with local vital records data, and annual matches to the National Death Index and Social Security Death Master File. A unique person-level identifier links PLWH across the FSU database and the registry.
Our study population included all PLWH ≥13 years of age, presumed OOC, and re-engaged in HIV care during January 1, 2009–December 31, 2013, who had any report of HIV CD4 or VL in the registry from the date they were re-engaged in care through December 31, 2015 (Fig. 1). PLWH re-engaged in care from January 2009 to December 2013 whose first CD4 or VL reports in the registry were performed after December 2013 were excluded from the analytic sample. Furthermore, persons who were reported to have died or moved out of NYC by December 31, 2013, as per the registry were excluded from the analyses of engagement, continuous engagement, and VS in the study follow-up year in which they were reported to have died or moved.
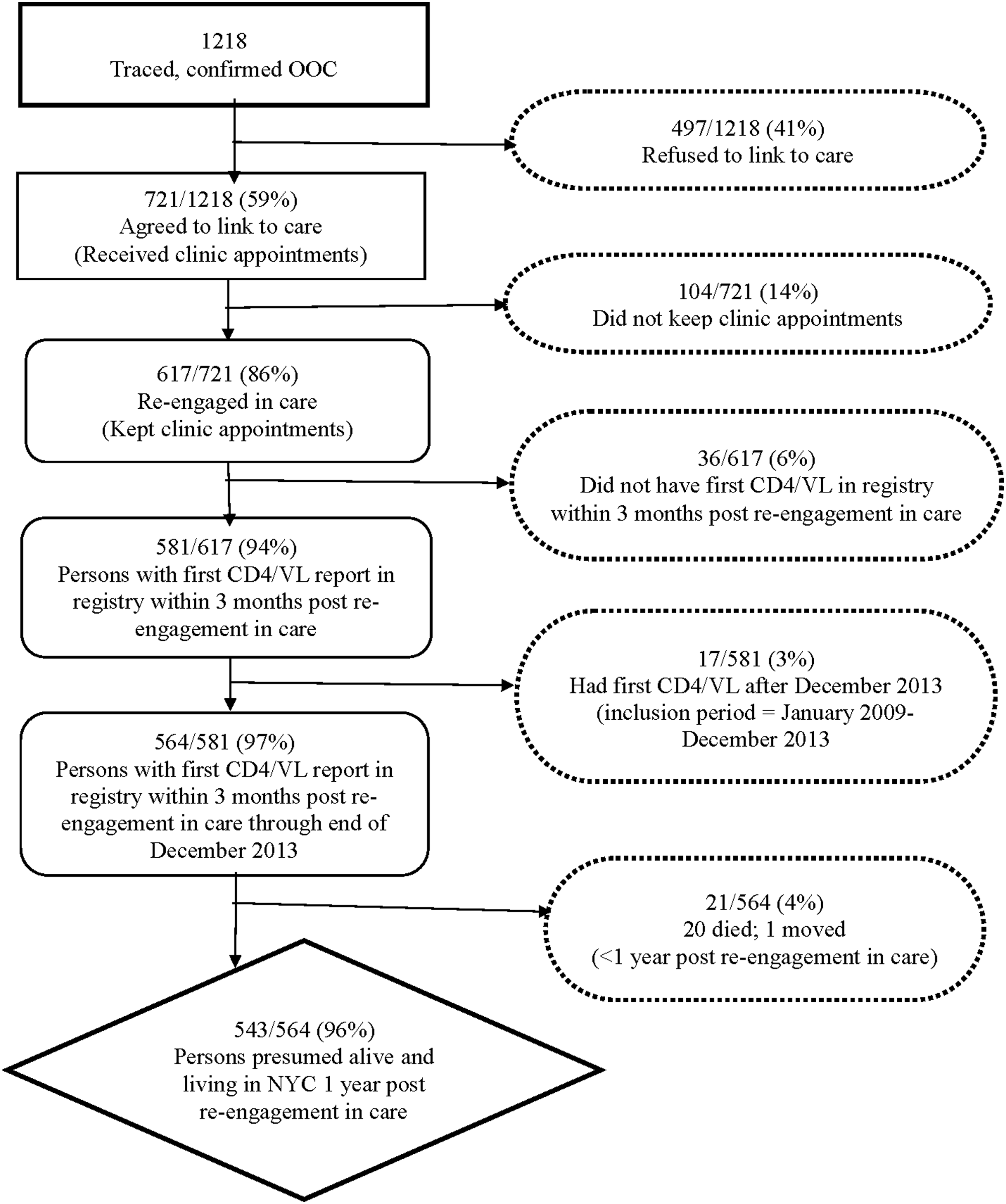
Flow chart of people living with HIV presumed and confirmed to be OOC after being traced in New York City, January 2009–December 2013. OOC, out of care; VL, viral load.
We created five subcohorts of our study population based on time since care re-engagement and the number of follow-up years (1–5 years) in which the OOC-PLWH re-engaged in care were eligible for observation (Fig. 2). For instance, the subcohort of PLWH re-engaged in care with a laboratory report in the registry from January 1 to December 31, 2009, was eligible for assessments of engagement, continuous engagement, or VS in follow-up years (January 1–December 31, 2010; 2011; 2012; 2013; and 2014). Persons re-engaged in care in 2009 were not assessed for engagement or continuous engagement in care and VS in 2015 (year 6) post re-engagement in care due to the small number of persons deemed to be alive and residing in NYC in 2015, after excluding persons presumed to have moved or died from 2009 to 2015.
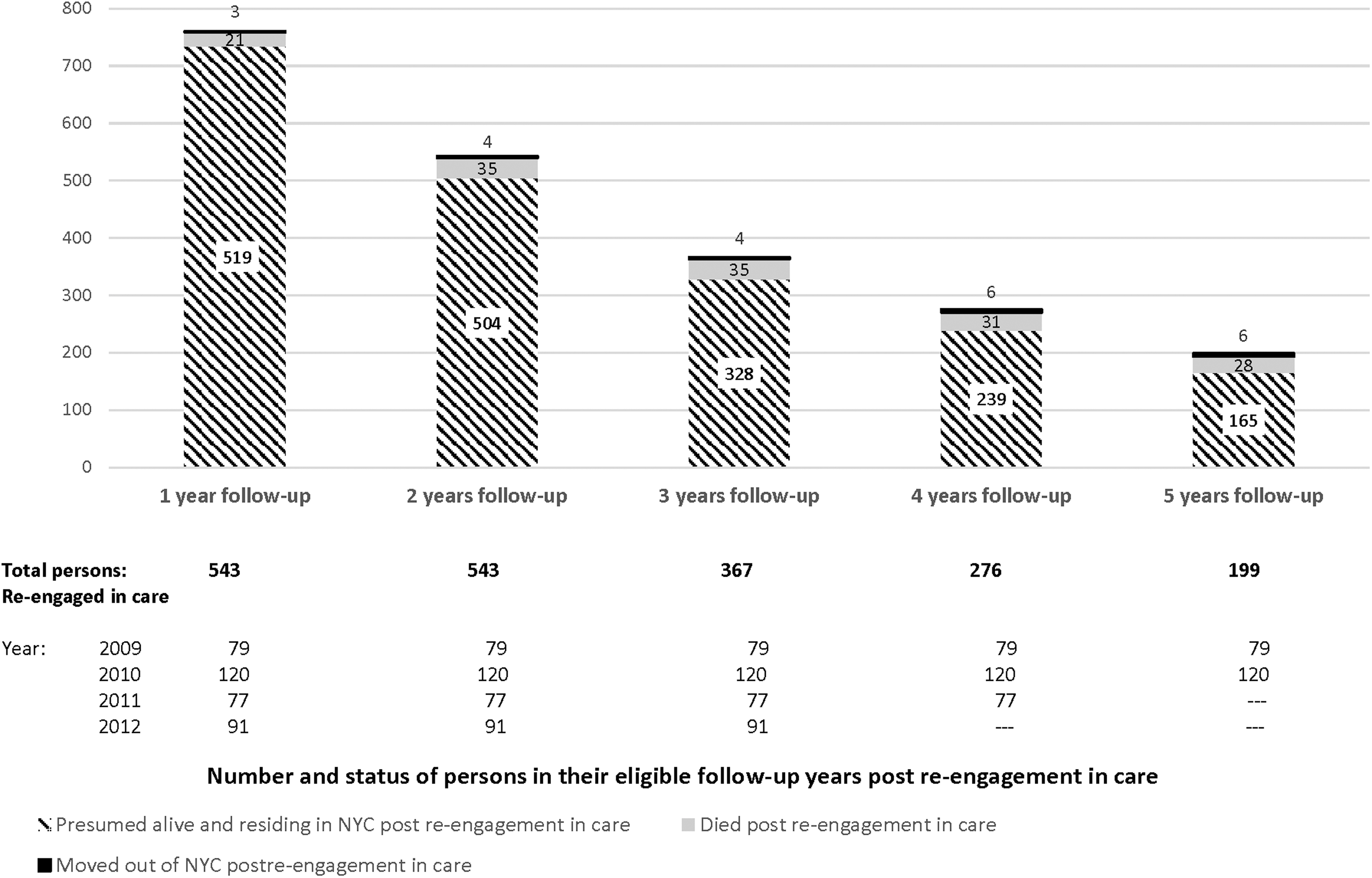
Persons re-engaged in care, January 2009–December 2013 and their living status in follow-up years.
Variables and outcomes
PLWH re-engaged in care were defined as OOC-PLWH who were traced and given an appointment with an HIV provider, who kept the appointment, and had at least one report of a CD4 and/or VL in the registry within 3 months of the appointment date. We examined four outcomes in the 1–5 follow-up years, specifically the number and percentage of the cohort of PLWH re-engaged in care in each follow-up year who: (1) engaged in care; (2) continuously engaged in care; (3) inconsistently engaged in care; and (4) achieved VS.
Engagement in care was defined as having ≥1 CD4 or ≥1 VL test result in any eligible follow-up year post re-engagement in care. Continuous engagement in care was defined as having ≥1 CD4 or ≥1 VL test result in each eligible follow-up year. Furthermore, the subset of persons continuously engaged in care with ≥2 laboratory test results, at least 3 months apart, were considered retained in care. Inconsistent engagement in care was indicated by persons who had no care in one or more of the follow-up years; these persons were excluded from the group considered to be continuously engaged in care in each follow-up year. VS was defined as VL ≤200 copies/mL in any follow-up year for persons continuously engaged in care. In addition, we assessed PLWH who were continuously engaged in care but had VL below or above 1500 copies/mL in any of the follow-up years post RTC. Previous studies have shown risk of HIV transmission at VL >1500 copies/mL. 23 –26
Study design and statistical analyses
This is a retrospective analysis of engagement in care and HIV care outcomes among cohorts of OOC-PLWH who had laboratory reports of CD4 or VL in the registry 1–5 years post-care re-engagement. We examined the composition of the PLWH with respect to gender, race/ethnicity, age group, transmission risk category, country of birth, time since HIV diagnosis, time from OOC to care re-engagement, whether the PLWH had active health insurance coverage at the time of care re-engagement, and the health insurance issuer. We assessed the overall frequencies and proportions of outcome measures: engagement and continuous engagement in care, inconsistent engagement in care, and VS.
We compared persons who were traced but refused to re-engage in care to persons who were traced and agreed to re-engage in care with regard to sociodemographic characteristics and duration of OOC. Furthermore, we compared persons continuously or inconsistently engaged in care with respect to sociodemographic and HIV-related characteristics. To assess engagement or continuous engagement in care and VS in the eligible follow-up years after care re-engagement, we calculated 365-day intervals from the first laboratory report date and created analytic subcohorts of the PLWH and eligible assessment years based on time since care re-engagement: year 1 (re-engaged = January 2009–December 2013); year 2 (re-engaged = January 2009–December 2013); year 3 (re-engaged = January 2009–December 2012); year 4 (re-engaged = January 2009–December 2011); and year 5 (re-engaged = January 2009–December 2010). We determined for each cohort of PLWH considered to be alive and residing in NYC (not known to be dead or have moved) in their eligible year(s) of observation (1–5) post-care re-engagement, to see if PLWH had at least one VL or CD4 report in the registry. It was possible for PLWH to be engaged in care for a number of years and subsequently become OOC.
We used the chi-square test of proportions and Fisher's exact test to evaluate the statistical significance of differences between groups. Multiple logistic regression was used to examine factors associated with continuous engagement in care and suppressed VL. All analyses were performed using SAS 9.3 software (SAS Institute, Cary, NC) and statistical significance was set at p < 0.05.
Results
From January 2009 to December 2013, case workers successfully contacted 1218 PLWH who were confirmed to be OOC, 41% (497) of whom refused to re-engage in care (Fig. 1). We found no significant differences between PLWH who accepted clinic appointments and those who refused to re-engage in care with regard to race/ethnicity, age groups, gender, HIV transmission risk, or having active health insurance coverage. However, there were significant differences (all p = < 0.0001) between PLWH who agreed or refused to re-engage in care. PLWH re-engaged in care were more likely than persons who refused care re-engagement (13% vs. 3%) to have been OOC for <1 year and conversely, PLWH who refused care re-engagement were more likely than those PLWH who re-engaged in care (66% vs. 52%) to have been OOC >3 years. Of the 721 PLWH who accepted clinic visit appointments, 86% (617) kept an appointment with an HIV provider, and 94% (581/617) of persons who kept appointments had ≥1 CD4 or VL report in the registry within 3 months of their re-engagement in care. Of these 581 re-engaged persons with CD4/VL reports in the registry, and 564 had CD4/VL reports in the registry within the analytic period (January 1, 2009–December 31, 2015). After excluding persons who died (n = 20) or had moved out of NYC (n = 1) <365 days after re-engagement in care, our analyses to assess engagement, continuous engagement in HIV care, and VS were based on the 543 persons presumed to be alive and residing in NYC at the start of their first follow-up year.
Characteristics of RTC-PLWH
Table 1 describes overall, the sociodemographic and HIV-related characteristics of the 543 PLWH in year 1 post-care re-engagement. Overall, the 543 PLWH re-engaged in care were mostly male (59%), 30–49 years of age (55%), non-Hispanic black (59%), were US born (82%), and had heterosexual HIV transmission risk at the time of diagnosis (40%). Fifty-eight percent of these 543 PLWH received their HIV diagnosis >10 years ago and 61% had been OOC for 1–3 years before selection for re-engagement efforts. Eighty-six percent (469) of the 543 PLWH had active health insurance coverage at the time of care re-engagement, with 84% (457/469) covered by public health insurance plans.
All persons returned to care with CD4 or VL in the registry on day 1 of their first eligible follow-up year. These include persons with inconsistent care or continuous engagement in care and exclude persons presumed to have moved or died post re-engagement in care.
Continuous care is defined as ≥care visit in each year post re-engagement in care.
Inconsistent care is defined as missing care visits in one or more years post re-engagement in care.
Care visit is defined as having a CD4 or VL test result, among persons returned to care in the follow-up years (2010–2015) post re-engagement in care.
IDU, injection drug use; MSM, men who have sex with men; OOC, out of care; US, United States.
Engagement and continuous engagement in care
In year 1 post-care re-engagement, 4% (24/543) of re-engaged PLWH had died or moved out of NYC, leaving 96% (519/543) of the PLWH who were deemed alive and residing in NYC to be assessed for engagement in care in the first follow-up year (Fig. 1). In the subsequent follow-up years (2–5) post re-engagement, 504 (year 2), 328 (year 3), 239 (year 4), and 165 (year 5) subcohorts of PLWH, respectively, were presumed to be alive and living in NYC, hence, eligible for assessment for continuous engagement in care in those follow-up years.
Among the respective PLWH subcohorts eligible for assessment for engagement in care, the proportions of PLWH subcohorts continuously engaged in care in their eligible years was highest in the first follow-up year (86%), and declined over time: 77% (2 years), 72% (3 years), 67% (4 years), and 63% (5 years) (Fig. 2). The proportions of PLWH retained in care with ≥2 CD4/VL reports (3 months apart) in their eligible follow-up years post-care re-engagement were markedly lower than the proportions continuously engaged with ≥1 CD4/VL reports, and progressively declined over time: 66% (1 year), 49% (2 years), 43% (3 years), 36% (4 years), and 26% (5 years), respectively (Fig. 3). The median number of laboratory reports for all persons continuously engaged in care in their eligible years ranged between 2 and 3 CD4/VL reports as per follow-up year.

Engagement and retention of persons re-engaged in care, January 2009–December 2013 in follow-up years. VL, viral load.
In multiple logistic regression analysis, HIV transmission risk factor was significantly associated with being continuously engaged in care. The odds of continuous engagement in care were 50% lower among PLWH re-engaged in care with heterosexual HIV transmission risk than those PLWH with MSM HIV transmission risk [adjusted odds ratio (aOR) = 0.50; 95% CI:0.30–0.90; p = 0.01]. We found no association between continuous engagement in care and sociodemographic characteristics, time since HIV diagnosis, duration of OOC before re-engagement in care, or health insurance status at the time of re-engagement.
Inconsistent engagement in care
Overall, only 29 PLWH re-engaged in care subsequently became OOC within 1 year and never re-engaged in care during the analytic period. Thirty-four percent (187) of PLWH re-engaged in care were inconsistently engaged in care in their eligible follow-up years (Table 1). These individuals may have re-engaged in and then exited care at various points during the five follow-up years. Most people became OOC again in their first (40%) and second (30%) follow-up years post-care re-engagement. We found no significant differences between persons continuously engaged in care and those with inconsistent care with regard to sociodemographic characteristics, time since HIV diagnosis, duration of OOC before care re-engagement, or health insurance coverage.
Viral suppression
Among the 543 PLWH re-engaged in care and presumed to be alive and living in NYC in the first follow-up year, 86% (444) had ≥1 HIV care visit in the first follow-up year (Fig. 4). Of these, 97% (431) had ≥1 VL test report in the registry; the remaining PLWH had only CD4 test reports. Of the 431 PLWH with VL reports, 65% (278) had a suppressed VL ≤200 copies/mL in the first follow-up year with a median of 44 days [interquartile range (IQR) = 158 days] from the date they were re-engaged in care.
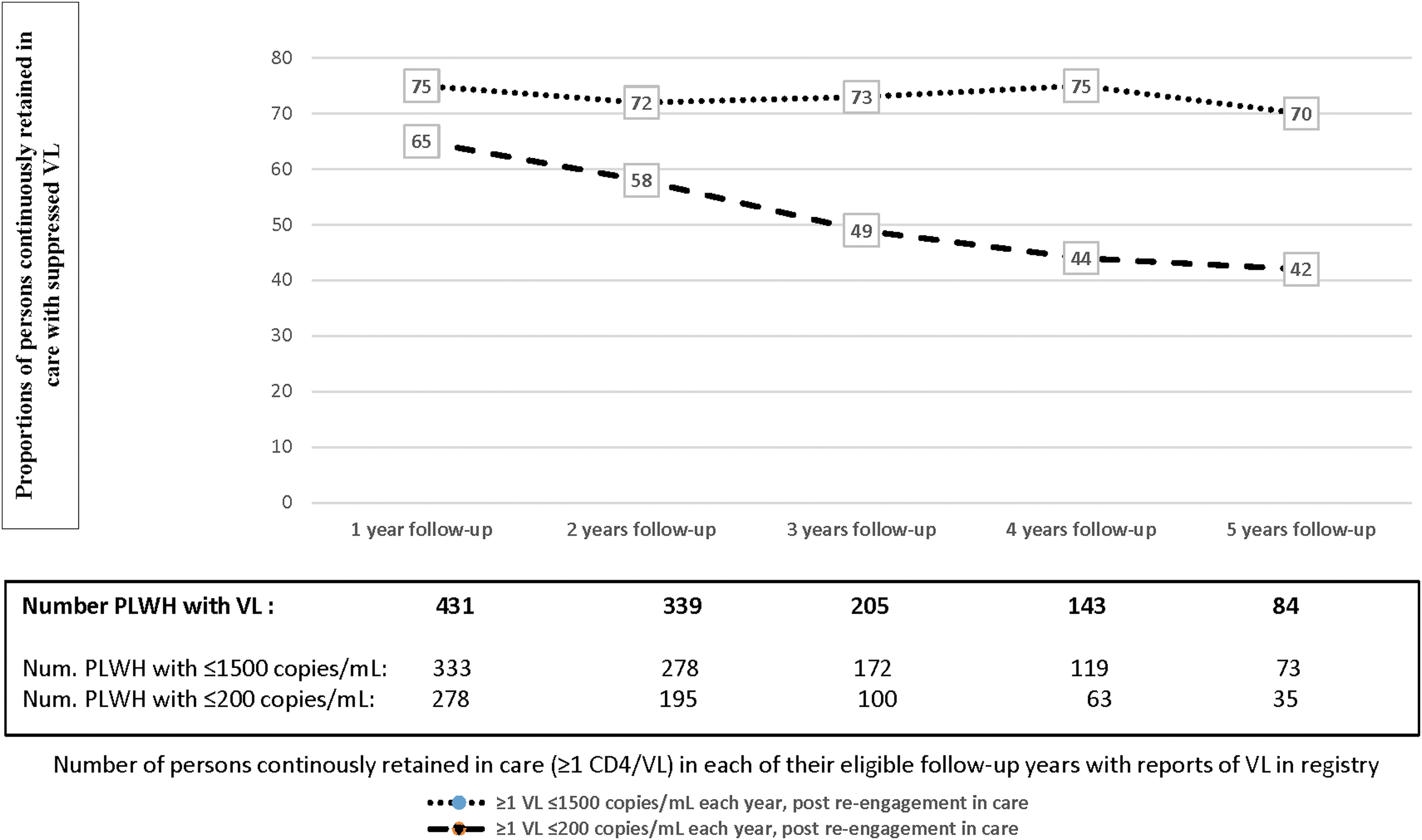
Proportion of persons living with HIV (PLWH) in continuous care in each eligible follow-up year with a registry report suppressed VL ≤200 copies/mL or VL below the transmissible threshold (≤1500 copies/mL). VL, viral load.
In successive follow-up years, fewer PLWH continuously engaged in care had VS (≤200 copies/mL) in each of their eligible follow-up years: 58% (2 years), 49% (3 years), 44% (4 years), and 42% (5 years). However, higher proportions of PLWH continuously engaged in care with ≥1 visits had VL ≤1500 copies/mL than VS in each of their eligible follow-up years: 75% (1 year), 72% (2 years), 73% (3 years), 75% (4 years), and 70% (5 years), thus indicating levels of HIV care and treatment in those years.
Discussion
To our knowledge, this is the first longitudinal assessment of engagement and sustained engagement in care of persons previously OOC and re-engaged in HIV clinical care by public health case workers. Prior studies have examined the engagement and retention in care (from 1 to 8 years) of cohorts of persons after their new HIV diagnosis using clinic visits and/or the surveillance registry. 12,27 –30 Our study provides 1- to 5-year longitudinal evaluation of cohorts of PLWH, regardless of the time since their HIV diagnosis, who had a history of engagement in care and OOC, then received assistance with re-engagement in care, and thus may be prone to repeat OOC.
High proportions of PLWH re-engaged in care remained in care at some points during their eligible follow-up years. The proportions of PLWH continuously engaged in care with ≥1 CD4/VL reports or retained in care with ≥2 CD4/VL reports (3 months apart) in each follow-up year decreased over time. The proportions of our study population engaged in care with ≥1 CD4/VL reports in each year (63–86%) approached or exceeded previous estimates (using the HIV surveillance registry) of newly diagnosed PLWH in NYC continuously engaged in care with ≥1 CD4/VL reports (82–83%) from 2006 to 2010 diagnoses years, but the proportions of our sample retained in care with ≥2 CD4/VL reports, at least 3 months apart (26–66%), are lower than those of citywide newly diagnosed PLWH (67–68%). 27
We found that 34% of PLWH re-engaged in care and deemed to be alive and residing in NYC in their follow-up years were subsequently OOC or had inconsistent care in one or more follow-up years. The highest dropout rates were observed in the first (40%) and second (30%) follow-up years. Although a standard definition of OOC is lacking, ranging from 6 to 12 months or longer with no HIV care visit, the 34% OOC rate in our study was comparable to the 34% reported for OOC after linkage in care following HIV diagnosis in NYC 30 and the rates (15–35%) reported by other studies. 12,31 –34 Our sole reliance on laboratory reports in the registry may have resulted in the inflation in our study sample of persons presumed OOC or with inconsistent care. 34,35
It may be expected that previously OOC-PLWH and re-engaged in care may subsequently become OOC after a few years of HIV care. Reports have shown that “feeling well” is among the primary reasons for disengaging from care given by PLWH previously OOC. 19,21,36 –40 Therefore, persons re-engaged in care following periods of OOC in which they had no significant health concerns may be prone to repeat disengagement from care. Upon care re-engagement, careful examination by HIV care providers of the potential sociobehavioral factors underlying prior OOC (e.g., stable housing, mental illness, substance abuse, disability and social obligations) is warranted to address and reduce ongoing barriers to retention in care. 41,42 Programs that involve active follow-up of patients (patient navigation, care coordination, case management) 14 –17 should be promptly initiated post-care re-engagement and tailored to individuals' needs of support services to mitigate individual barriers and facilitate adherence to care and treatment.
Our results suggest that most persons who were re-engaged in care had prompt initiation or re-initiation of ART, with two-thirds of persons with VL report after care re-engagement having VS within 2 months. At least 70% of our study sample had a VL ≤1500 copies/mL during each of their follow-up years, which indicates sustained engagement in HIV treatment. Nevertheless, in each follow-up year, 25–30% of our study cohorts who were otherwise continuously engaged in care had VL >1500 copies/ML and the proportions with VS ≤200 copies/mL were lower and progressively declined with each additional follow-up year. Prior studies have found associations between certain sociodemographic groups and structural factors and “blips” in VL above undetectable levels among persons current with HIV care or durably retained in HIV care. 23,43 –45 These findings underscore the continuing need for case management and HIV prevention interventions, including reinforcing condom use and HIV pre-exposure prophylaxis treatment for the HIV-uninfected partners of PLWH, especially those who have unsuppressed virus. 46 –49
Our analysis has several limitations. First, we assessed engagement in care using HIV-related laboratory test results. Surveillance may not always capture complete or up-to-date information on whether people move out of NYC, died, or are incarcerated. Previous studies have used varying criteria to measure engagement and retention in care. Overall, consistent with previous estimates, 12,28 lower proportions of our study cohorts were retained in care with ≥2 CD4/VL reports than continuously engaged in care with ≥1 CD4/VL reports within 1 year. It is possible that we underestimated the proportions of our study sample that were continuously engaged in care because of our reliance on surveillance reports alone. Studies have found that estimates, which combine laboratory test results and outpatient visits, are more reliable in capturing clinic care visits that were not accompanied with HIV-related laboratory results. 28,50
However, local validation work has shown that laboratory tests are a good proxy for HIV medical care visits. 22 Information was not available to determine if CD4 or VL tests were ordered during in-patient stay or emergency health department visits. Although our sample represents NYC PLWH, the vast majority of our study sample received care under public health insurance, and rates of care engagement and VS may differ from patients with private insurance plans.
In summary, we found that large proportions of persons previously OOC and re-engaged in HIV care by public healthcare workers remained engaged in care at some point in the 5 years post-care re-engagement. Almost two-thirds had at least one CD4/VL report in each of their follow-up years. Subsequent disengagement from care was highest in the first 2 years post re-engagement. Despite apparent continuous engagement in care, considerable proportions of PLWH had unsuppressed VL in each follow-up year, placing them at risk of potentially transmitting HIV to HIV-uninfected partners. Efforts to use surveillance data to identify, trace, and re-engage in care OOC-PLWH are worthwhile, however, structures and programs must be in place to help PLWH remain in care to reduce subsequent OOC.
Footnotes
Acknowledgments
The authors are grateful to the New York City HIV case workers for their dedication and hard work in locating and assisting HIV-diagnosed persons with linkage to care and partner services. Funding for this program was provided by Ryan White HIV Care program Part A, Grant No. 93.914.
Human Participant Protection
No institutional review board approval was necessary because this is a secondary analysis of data collected as part of the New York City DOHMH routine case and partner services program. For this type of study, no formal consent is necessary.
Author Disclosure Statement
No competing financial interests exist.