
Abstract
The prevalence of HIV pretreatment drug resistance (PDR) is increasing in sub-Saharan Africa. We sought to describe correlates of PDR and evaluate effects of PDR on clinical outcomes in rural Uganda. We analyzed data from the Uganda AIDS Rural Treatment Outcomes study, a cohort of antiretroviral therapy (ART)-naive adults with HIV (2005–2015). We performed resistance testing on pre-ART specimens. We defined PDR as any World Health Organization (WHO) 2009 surveillance drug resistance mutation and classified PDR level using the Stanford algorithm. We fit unadjusted and sex-stratified log binomial regression and Cox proportional hazard models to identify correlates of PDR and the impact of PDR on viral suppression, loss to follow-up (LTFU), and death. We analyzed data from 738 participants (median age 33 years, 69% female). Overall, prevalence of PDR was 3.5% (n = 26), owing mostly to resistance to non-nucleoside reverse transcriptase inhibitors. PDR increased over time in women (1.8% in those enrolling in clinic in 2001–2006, vs. 7.0% in 2007–2013; p = 0.006), but not in men (1.15% vs. 0.72%, p = 0.737). Lower pre-ART log10 HIV RNA was also associated with higher prevalence of PDR. We identified longer time to viral suppression among those with PDR compared with without PDR (0.5 and 0.3 years, respectively, p = 0.023), but there was no significant relationship with mortality or LTFU (p = 0.139). We observed increasing rates of PDR in women in southwestern Uganda. Implications of this trend, particularly to prevention of mother-to-child transmission programs in the region, require attention due to delayed viral suppression among those with PDR.
Introduction
W
Epidemiologic data on PDR are necessary in SSA to achieve multiple goals. First, because resistance testing is not typically included as part of recommended pre-ART evaluation in the region due to cost constraints and availability, local epidemiology can be used to help establish optimal empiric ART regimens. Second, correlates of PDR can potentially assist with identifying individuals at highest risk of resistance for alternate therapies or monitoring protocols. Finally, the epidemiology of PDR, including its relationship with treatment outcomes and mortality, is required to ensure that an adequate public health response to drug resistance can be planned. For example, areas with higher prevalence of resistance might prioritize altering empiric treatment guidelines, formularies, and diagnostic testing infrastructure.
In this study, we analyzed data from a 10-year longitudinal cohort of individuals living with HIV and initiating ART in rural Uganda. Our aims were (1) to describe the prevalence and patterns of PDR during 2005–2013, (2) to identify clinical correlates of PDR, and (3) to estimate the effect of PDR on clinical outcomes, including viral suppression, loss to follow-up (LTFU), and all-cause mortality.
Materials and Methods
Study design and population
We analyzed data collected as part of the Uganda AIDS Rural Treatment Outcomes (UARTO) cohort study (NCT01596322), which was conducted at the Mbarara Regional Referral Hospital Immune Suppression Syndrome (ISS) Clinic, a government-run, PEPFAR-supported facility in southwestern Uganda. UARTO enrolled ART-naive participants living with HIV who were >18 years of age, in care at ISS, initiating first-line ART, and living within 60 km of the clinic.
A detailed history regarding any previous ART exposure was recorded at the time of screening for entry into the study. Women who had previously received single-dose nevirapine for prevention of mother-to-child transmission (PMTCT) were not excluded. Participants were enrolled from 2005 to 2013 with follow-up through August 2015. Follow-up for each participant continued until death, study withdrawal, LTFU, or study end date. During the follow-up period, decisions to switch to second-line ART were determined by ISS Clinic staff based on clinical and immunological failure criteria. Pre-ART genotypic resistance testing was planned for all UARTO participants, and for this analysis, we included all participants for whom resistance testing was successfully completed.
Data collection
Study staff collected basic demographic information for participants at the time of study enrollment. In addition, information was collected regarding family members in the household, including number of living children. Reproductive health data were collected beginning in 2011, which included information regarding pregnancy within the year before enrollment.
Laboratory procedures
Study participants underwent phlebotomy at the time of enrollment (before initiating ART), every 3 months during study observation from 2005 to 2011, and every 4 months from 2011 to 2015. HIV RNA was measured using the Roche Amplicor HIV-1 Monitor System (Branchburg, NJ) from 2005 to 2012 and COBAS TaqMan System (Branchburg, NJ) from 2012 to 2015.
Sanger sequencing of the reverse transcriptase gene was attempted for all pre-ART specimens. Total nucleic acid was extracted from 500 μL plasma samples using NucliSENS easyMag (bioMérieux). Reverse transcription and cDNA synthesis was performed with SuperScript® III One-Step RT-PCR System (Invitrogen) followed by “nested” second-round PCR. Primers: first-round PCR forward 5′-GAAGGGCACACAGCCAGAAATTGCAGGG3′ (5CP1), reverse 5′-GCTCCTACTATGGGTTCTTTCTCTAACTGG3′ (RT3.1); second-round PCR forward 5′-CCTAGGAAAAAGGGCTGTTGGAAATGTGG3′ (2.5), reverse 5′-CAAACTCCCACTCAGGAATCCA3′ (RT3798R). Thermocycler setting: 2 min @ 94°C, 10 cycles (15 sec @ 94°C, 30 sec @ 55°C, 1 min 30 sec @ 72°C), 25 cycles (15 sec @ 94°C, 30 sec @ 55°C, 1 min 30 sec @ 72°C*) *adds 5 sec/cycle, and 7 mins @ 72°C. Bulk sequencing was performed on ABI 3730 DNA Sequencer using the BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems). Resulting chromatograms were aligned with HXB2 and base-called using in-house software RECall. 10 Resulting sequences correspond to HXB2 pol 2253–3269 or 2253–3749. Genotypic resistance tests were not performed in real-time and thus were not available to care providers for clinical use.
Genotypic resistance test interpretation
Raw unaligned sequences were input into the Stanford Calibrated Population Resistance tool version 6.0 to align sequences and identify PDR mutations from the 2009 WHO list of surveillance drug resistance mutations. 11 We defined PDR as the presence of any mutation from this list. We also used the Stanford HIVdb Genotypic Resistance Interpretation Algorithm version 8.3 to classify resistance patterns as low (Stanford level 1–3), or intermediate to high-level resistance (Stanford level 4–5) to the drugs comprising the participants' first prescribed ART regimen. 12
Statistical analysis
To summarize PDR patterns in this cohort, we calculated the frequency of drug resistance mutations, categorized by both drug class and specific mutation. We then fit unadjusted log binomial regression models using sex, age, period of clinic enrollment, ART start year, pretreatment CD4 count, and pretreatment log10 HIV RNA as correlates of interest and PDR as the outcome of interest. These clinical correlates of interest were chosen based on prior studies and results of the 2017 WHO Drug Resistance Report. 4,13 –17 We also evaluated the association between period of clinic enrollment and PDR prevalence in Chi square tests, stratified by sex. In subanalyses among women, we explored PMTCT history, history of recent pregnancy, and number of living children (as a proxy for prior pregnancies) as predictors of interest.
In a separate analysis, we fit unadjusted Cox proportional hazards models and produced Kaplan–Meier curves, for both the entire study population and stratified by sex, with intermediate/high-level PDR to the initial ART regimen as the primary predictor of interest and time to (1) viral suppression, (2) LTFU, and (3) death as outcomes of interest. The entry date for each participant was defined as the date of the pretreatment genotypic resistance test. In the model with viral suppression as the outcome of interest, we defined suppression as an HIV-1 RNA viral load <400 copies/mL. Participants were censored at the date of the first suppressed viral load measurement, date of last contact, or date of death. In the model with LTFU as the outcome of interest, participants were defined as LTFU if they ceased attending the ISS clinic before study conclusion and had unconfirmed vital status despite phone calls and tracking at their home for over 12 months. Participants were censored on the date of the last known visit. In the model with death as the outcome of interest, participants were censored at the date of death. In a secondary analysis, we treated death or LTFU as a composite outcome of interest, and participants were censored at the date of death or last known visit. Surviving participants who remained in care were right censored at their last study visit (approximately August 2015). In another secondary analysis, we evaluated the effect of regimen type (NVP vs. EFV-based) on the relationship between PDR and time to viral suppression in a Cox proportional hazards model, inclusive of an interaction term. The assumption of proportional hazards was tested using models inclusive of time varying covariates. All statistical analyses were conducted with Stata version 14 (Stata Corp, College Station, TX).
Ethics
This study was approved by the Institutional Review Boards at Partners Healthcare, University of California San Francisco, Mbarara University of Science and Technology, and Uganda National Council for Science and Technology. All participants provided signed written consent for the study, including for storage and genotypic resistance testing of biological specimens.
Results
Of 762 participants in the UARTO cohort at pretreatment baseline, 24 (3%) participants did not have genotypic resistance test results available. Of these 24, 9 participants had failed resistance tests due to poor specimen quality; 8 had results excluded due to incorrect labeling; 4 had failed resistance tests due to low viral load <1000 copies/mL; and 4 had an undetectable viral load. Seven hundred thirty-eight participants (97%) had successful pre-ART genotypic resistance tests and were included in the analysis. Demographic characteristics of the study population are summarized in Table 1. Sixty-nine percent (510/738) of study participants were women, and median age was 33 years at the time of study enrollment. Forty-two percent (311/738) were enrolled in the clinic during 2001–2006, whereas the remainder were enrolled during 2007–2013. The most common initial ART regimens were lamivudine (3TC), zidovudine (AZT), and nevirapine (NVP) (48%, 355/738); 3TC or emtricitabine, tenofovir (TDF), and efavirenz (EFV) (24%, 179/738); 3TC, stavudine (d4T), and NVP (15%, 109/738); and 3TC, AZT, and EFV (11%, 81/738).
Categorical data are listed as count (%). Continuous variables are listed as median (IQR).
ART, antiretroviral therapy; PDR, pretreatment drug resistance.
Resistance patterns
We identified PDR in 3.5% of participants (26/738; 95% CI 2.4%–5.1%). Twenty out of 26 with PDR (77%) had intermediate to high-level resistance to their initial ART regimen. Of these 20, 10 participants were prescribed an initial regimen containing NVP, and 10 were prescribed an initial regimen containing EFV. Of those with any PDR, we identified NNRTI mutations in 81% (21/26) of participants, with K103N being most common. We identified NRTI mutations in 8/26 (31%) participants with PDR. Of those with NRTI resistance, only one participant was found to have K70E, and no participants were found to have K65R. The majority of participants with PDR had only single-class resistance, although 3/26 (12%) had two-class resistance (Fig. 1). Among participants with any PDR, only 5/26 (19%) had NRTI resistance exclusively, and of those, only one participant had intermediate to high-level resistance to their initial ART regimen.

Prevalence of pretreatment drug resistance mutations in resistant strains
Correlates of PDR
In unadjusted log binomial regression models, each log10 viral load was a strong negative correlate of PDR (PR 0.51, 95% CI 0.32–0.83, p = 0.006; Table 2). In addition, female sex was a significant correlate of PDR (PR 5.36, 95% CI 1.28–22.51, p = 0.022; Table 2). In a subanalysis of women, there was a nonsignificant trend toward reduced rates of PDR in women with living children versus those without living children (PR 0.44, 95% CI 0.19–1.02, p = 0.056). When adjusted for period of clinic enrollment, this trend was unchanged. Pregnancy within the 12 months before enrollment was also not predictive of PDR. Only four women in the study reported a history of single-dose NVP use for PMTCT, and none of those women was found to have PDR.
*p < 0.05; ** p < 0.01
PR, prevalence ratio; ART, antiretroviral therapy.
Participants with PDR who enrolled in the clinic during 2007–2013, as compared with 2001–2006 had triple the prevalence of PDR (PR 3.07, 95% CI 1.17–8.06, p = 0.022; Table 2). When stratified by sex, there was a statistically significant increase in PDR from earlier to later clinic enrollment periods in women (1.8% vs. 7.0%, respectively, p = 0.006), but not in men (p = 0.737). This difference was driven primarily by increasing resistance to NNRTIs (Fig. 2).
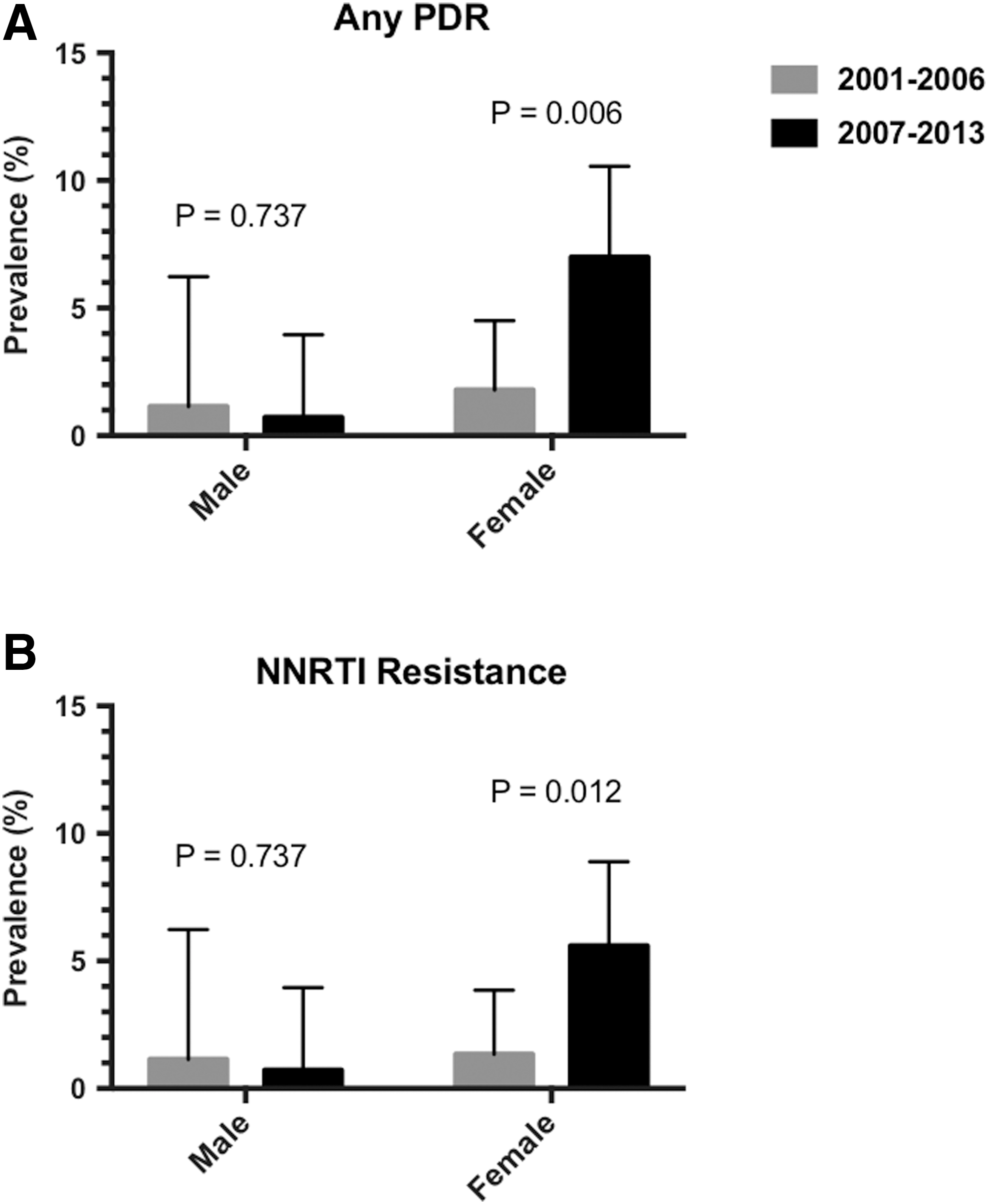
Disproportionate increase in any PDR (
Outcomes after PDR
Median time to initial viral suppression was 0.5 years (IQR 0.2–2.1 years) for participants with intermediate to high-level PDR to their initial ART regimen, as compared with 0.3 years (IQR 0.2–0.5 years) for participants without PDR to their initial regimen (p = 0.023), indicating a delay in virologic response in the setting of PDR (Fig. 3). Furthermore, 15% (3/20) of those with PDR never achieved virologic suppression, as compared with 10% (71/714) of those without PDR (p = 0.459). Among participants with PDR, 15% (3/20) were LTFU, vs. 6.7% (48/714) in the group without PDR (p = 0.151). No participants with intermediate to high-level PDR died during the study period (0/20, 0%). In those without intermediate to high-level PDR, there were 48 deaths (6.7%, p = 0.230).
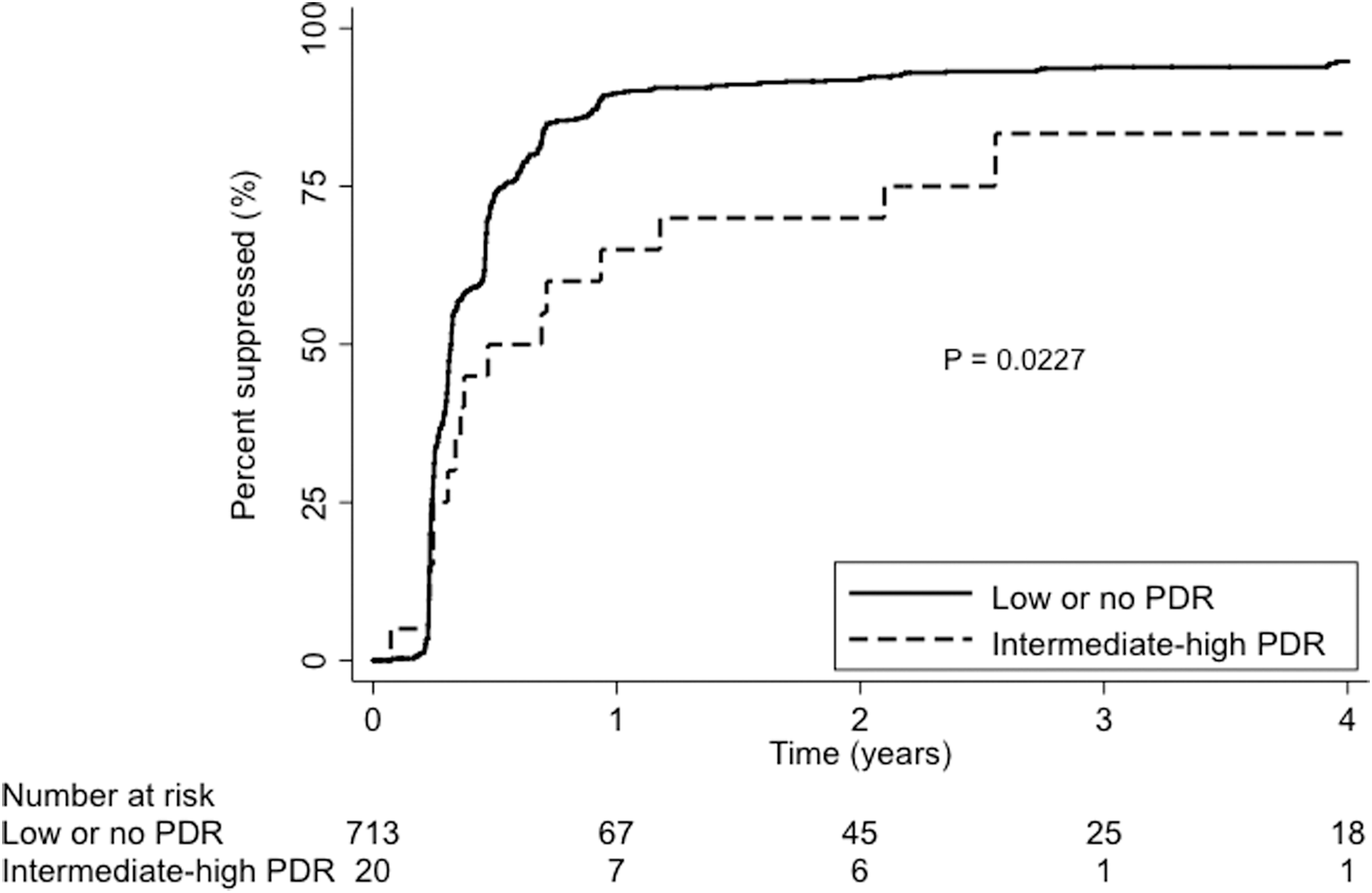
Viral suppression in participants with and without PDR. PDR, pretreatment drug resistance.
In unadjusted Cox proportional hazards regression models, time to initial viral suppression was significantly longer for participants with intermediate to high-level PDR, as compared with those without PDR (HR 0.57, 95% CI 0.35–0.93, p = 0.024; Table 3 and Fig. 3). In a secondary analysis, there was no statistically significant interaction between PDR and regimen type (NVP vs. EFV-containing; HR for the interaction term 0.51; p = 0.172) when evaluating the outcome of time to suppression. Although nonsignificant, there was a trend toward increased hazards of both LTFU and a composite of death or LTFU (Table 3). PDR was not predictive of death (p = 1.00).
No patients with TDR died during follow-up.
p < 0.05, ** p < 0.01.
NA, not applicable; PDR, pretreatment drug resistance.
In models restricted to women, PDR remained associated with longer time to viral suppression (HR 0.47, 95% CI 0.27–0.83, p = 0.008, Table 3) and was also significantly associated with LTFU (HR 3.31, 95% CI 1.01–10.89, p = 0.048). PDR was not predictive of death in this secondary analysis.
Discussion
In this analysis using data from a longitudinal cohort study of ART-naive adults initiating treatment in southwestern Uganda, we describe two important epidemiological phenomena: (1) higher prevalence of PDR in women than men and (2) increasing prevalence of PDR over time in women, but not men. A higher prevalence of PDR among women has also been described in the WHO 2017 HIV Drug Resistance Report, which found rates of PDR twice as high in women as compared with men. 4 Moreover, we found increased time to viral suppression (median 0.5 vs. 0.3 years, Fig. 3) and a trend toward increased loss from care among those with PDR as compared with those with no PDR. Taken together, these data support policy changes away from use of NNRTI-containing first-line regimens to prevent negative effects on the health of women in the region.
We hypothesized that prior ART exposure from prior PMTCT-related ART use might be responsible for higher rates of PDR in women. 7,18 To explore this hypothesis, we assessed for relationships between reported single-dose NVP use, prior pregnancies, number of living children, and PDR. We found no significant relationships between any of these and presence of PDR. However, our pregnancy history data were limited to 2011–2013, and our questionnaire did not include data collection on deceased children, so prior pregnancies might be underreported in our dataset. Women might also be more likely to have undisclosed prior ART use. For example, in a previous analysis, including a portion of this cohort, investigators identified detectable plasma NVP concentrations at the time of study enrollment in 3 of 14 female participants found to have PDR who underwent pharmacologic ART testing. However, none of these women reported recent pregnancy or NVP use. 19 Alternatively, increased rates of PDR in women could be more attributable to acquisition of virus from a partner with resistance, although we were unable to evaluate this hypothesis in our study.
In addition, we reported an increasing prevalence of PDR over time driven by increasing resistance to NNRTIs, a finding supported by multiple studies, including a recent multinational surveillance report by the WHO. 2 –6,20 This increasing prevalence of PDR is believed to be due to accrual of population exposure to ART after rollout of national HIV treatment programs. Other studies have also reported increases in rates of PDR in Uganda. 20,21 However, the WHO recently reported a pretreatment drug resistance prevalence of 17.4% in 2016. 4 This a substantial increase from prevalence reported in Uganda from prior WHO surveys with <5% NNRTI resistance and between 5% and 15% NRTI resistance in 2009. 22 While our findings do show an increase in rates of PDR from 1.6% during an earlier clinic enrollment period (2001–2006) to 4.9% during a later period (2007–2013), rates in our study were markedly lower than the rate reported by WHO and do not meet the threshold of >10% to support widespread change in policy for first-line ART regimens. This wide discrepancy could be partially explained by a difference in calendar time, in that our latest data are from 2013, whereas the WHO survey was conducted 3 years later. However, other factors are important to consider as well. The WHO utilized clustered sampling methodology with a total sample of 296 ART-naive participants in Uganda, resulting in a very low sample size for individual districts. 4 In addition, weighted prevalence estimates were not calculated for Uganda; thus, geographic discrepancies in PDR prevalence would not have been accounted for. 4 This issue is an important consideration of the WHO survey, particularly because previous studies identified large differences in PDR prevalence between urban versus rural health centers, even in relatively close geographic proximity. 23 –25
PDR was not a significant predictor of death, a finding consistent with other studies. 7,8 However, we did identify a nonsignificant doubling in LTFU among those with PDR. This finding could represent a higher frequency of self-transfers to other clinics among participants with PDR, and could be consistent with a possible history of undisclosed ART use before enrollment at the MRRH ISS Clinic. 26 Larger datasets will be needed to further elucidate whether PDR predicts poorer outcomes. Finally, we found that participants with PDR in our cohort had a longer time to viral suppression than those without PDR (Fig. 3), a trend that was also seen in other studies conducted in SSA. 7,8 Notably, because increasing prevalence of PDR was only seen among women, relationships between PDR and delayed suppression could have particularly deleterious effects on PMTCT programs in the region. Although many countries have planned to introduce dolutegravir (DTG)-based first-line ART regimens to counter effects of rising PDR, there is currently a paucity of safety data for use of DTG in pregnancy, which may limit its use in pregnancy. 27 Preliminary data from Botswana have shown no difference in adverse birth outcomes when comparing DTG to EFV-containing regimens, although data are lacking for safety at conception and in early pregnancy. 28 Until more robust safety data are available, recent WHO guidelines suggest that a protease inhibitor-containing regimen would be the recommended alternative for use in pregnancy in the setting of high rates of PDR. 29 However, given the toxicities and drug interactions present with protease inhibitor-based regimens, alternative strategies, such as pretreatment resistance testing could be explored for pregnant women in areas of increasing PDR.
Our results should be interpreted with respect to our single-site study design. In addition, we acknowledge that first-line ART regimens have changed since this study began in 2005 and no longer include d4T, AZT, or NVP. Still, EFV remains a preferred first-line regimen in Uganda and in much of the region. This study was not powered to detect a difference in the effect of PDR on viral suppression by regimen type (NVP vs. EFV-containing). We also did not analyze PDR to protease inhibitors or integrase inhibitors in this study, and so cannot comment on the effect of PDR on activity of second- or third-line regimens. However, the impact of PDR on these regimens will be an important future step in light of recent data on failures to second-line regimens in the region. 30 Our study may also be underpowered to detect differences in death and LTFU due to low frequency of these events in our study population, as well as relatively low overall prevalence of PDR in the cohort. Finally, while prior ART exposure was an exclusion criterion for the UARTO study, this information was obtained through self-report and does not account for undisclosed prior ART use.
In conclusion, rates of PDR are increasing over time with women being disproportionately affected. Our study adds to literature by further highlighting the disproportionate risk of PDR in women, and also by providing outcome data in those initiating care with PDR over a long duration of observation. Given the association between PDR and delayed virologic suppression, higher prevalence of PDR could have a negative impact on PMTCT programs in SSA due to risks of virologic failure during pregnancy and risk of increased mother-to-child transmission. Increased data on the safety of DTG in pregnancy as well as other strategies to combat the effects of PDR among women are needed to ensure they and their children fully benefit from ART programs in the region.
Footnotes
Acknowledgments
This work was supported by the National Institutes of Health (4T32 AI007433–25 and 5T32 AI007387 to S.M.M; P30 AI027763 and UM1 CA181255 to J.N.M; K23 MH099916 to M.J.S., and R01 MH054907 to D.R.B.) and the Harvard Center for AIDS Research (P30AI060354 to M.J.S.).
Author Disclosure Statement
No competing financial interests exist.