
Abstract
Ten years after the Centers for Disease Control and Prevention recommended universal HIV screening, rates remain low. Internal medicine residents are the front-line medical providers for large groups of patients. We evaluated the knowledge of internal medicine residents about HIV testing guidelines and examined adherence to universal HIV testing in an outpatient setting. A cross-sectional survey of internal medicine residents at four residency programs in Chicago was conducted from January to March 2016. Aggregate data on HIV screening were collected from 35 federally qualified community health centers in the Chicago area after inclusion of an HIV testing best practice alert in patients' electronic medical records. Of the 192 residents surveyed, 130 (68%) completed the survey. Only 58% were aware of universal HIV screening and 49% were aware that Illinois law allows for an opt-out HIV testing strategy. Most of the residents (64%) ordered no more than 10 HIV tests in 6 months. The most frequently reported barriers to HIV testing were deferral because of urgent care issues, lack of time, and the perception that patients were uncomfortable discussing HIV testing. From July 2015 to February 2016, the average HIV testing adherence rate in the 35 health centers was 18.2%. More effort is needed to change HIV testing practices among internal medicine residents so that they will adopt this approach in their future clinical practice. Improving knowledge about HIV testing and addressing other HIV testing barriers are essential for such a successful change.
Introduction
A
In September 2006, the Centers for Disease Control and Prevention (CDC) recommended routine HIV screening for all persons 13–64 years of age regardless of HIV-related risk factors and recommended annual HIV testing for persons at high risk for HIV acquisition 3 ; the American College of Physicians and the US Preventive Services Task Force followed with similar guidelines. 4,5 However, as of 2016, more than half of Americans have never been tested for HIV. What is most concerning is that 75% of persons at high risk for HIV had seen a provider in the past year, but were not offered a test. 1 Studies in other subpopulations, such as in pregnancy and the Emergency Department (ED), also reveal low rates of HIV testing. 6 A recent study showed that HIV retesting in the third trimester, as recommended by the CDC, was done only in 28% of pregnant women. 7 Likewise, data from the 2009 National Hospital Ambulatory Medical Care Survey showed that HIV testing was performed at only 0.2% of ED visits. 8
Internal medicine residents are an ideal population for studying the implementation and dissemination of best practices. They make up a substantial portion of the front-line medical providers for a large number of patients. The Accreditation Council for Graduate Medical Education requires internal medicine residency programs to devote a minimum of 130 half-day outpatient clinics to preventive and primary care. 9 Residents are also more likely to know and adopt evidence-based practices than are experienced healthcare providers. 10 However, research of knowledge and practices regarding HIV testing among internal medicine residents has been limited. In 2007, Jain et al. 11 conducted a survey on HIV testing-related knowledge among internal medicine residents in New York City. Other studies have included residents from different specialties or mixed practicing physicians and residents. These studies demonstrated that many providers were unaware of the updated recommendations for HIV screening, and few offered routine HIV testing. 12 –16 Although these findings are illuminating, most of these studies were either single-center studies or done shortly after the release of the CDC guidelines.
Based on prior studies demonstrating the lack of knowledge about HIV testing recommendations among healthcare providers, clinical reminders such as best practice alerts have been included in electronic medical records to remind physicians about recommended clinical services. Some studies demonstrated improved evidence-based practices, whereas clinicians in other studies described alert fatigue as they became desensitized to and less likely to accept alerts as they received increasing numbers of them. 17
Given the lack of information on HIV testing practices among internal medicine residents in the recent literature, we sought to evaluate the knowledge and practice of CDC HIV testing guidelines a decade after their release among internal medicine residents in different programs across Chicago. We also measured adherence to the guidelines in the outpatient setting after implementation of a best practice alert embedded within patients' electronic medical records reminding healthcare providers to order HIV tests.
Methods
Data collection
A cross-sectional survey of internal medicine residents at four programs in the Chicago area was conducted. The Illinois Northern Chapter of the American College of Physicians holds regular local meetings connecting internal medicine residents. During one such meeting, chief residents from 13 different programs were asked if they would like their programs to participate in a study about knowledge of HIV testing among internal medicine residents. Four residency programs agreed to participate and provided their residents' e-mail addresses so that they could receive the survey. Programs that did not participate cited lack of interest, lengthy IRB process, or participation in other studies.
The survey was e-mailed to the residents from January to March 2016, with two reminders to complete the survey sent to them monthly afterward. The SurveyMonkey software (San Mateo, CA) was used to collect the data. To ensure the respondents' anonymity, their e-mail addresses were replaced with study identification numbers. The SurveyMonkey program does not permit taking the survey more than once. If a residency program had a greater than 50% response rate, it received four $25 gift cards to be distributed to their residents using a raffle.
Measures
We adapted a survey on knowledge related to HIV testing and CDC HIV testing guidelines, which was developed in 2007, and distributed it to 1171 internal medicine residents in 42 residency programs across New York City. 11 Our survey consisted of 13 closed-ended questions.
Knowledge related to HIV testing and CDC HIV testing guidelines
Four survey questions assessed knowledge related to HIV testing and CDC HIV testing guidelines. The first question asked residents to identify the most common mode of HIV transmission in Chicago. The second one assessed awareness of a 2008 Illinois law allowing for opt-out HIV testing, in which a patient is informed that testing will occur unless he or she specifically declines it. The last two questions assessed their knowledge of CDC guidelines, specifically a question about the criteria for HIV testing (i.e., routine, based on prevalence of HIV infection in the practicing area, based on individual risk factors, and based on signs or symptoms of AIDS) and a question about the frequency of HIV testing in high-risk patients. Responses to each of these four questions were recoded as dichotomous variables (correct or incorrect). The overall knowledge score was defined as the number of correct answers (0–4).
Practice behaviors related to HIV testing
Three questions assessed practice behaviors: how often do residents obtain a patient's sexual history; personal experience in providing pretest counseling; and the number of HIV tests ordered over the past 6 months in a clinical setting, including inpatient, outpatient, and EDs. Responses regarding the number of HIV tests ordered were dichotomized into more than 10 versus 10 or fewer.
Other measures
Residents were asked if they had listened to formal lectures or received training about HIV screening. They were asked to check all answers that apply regarding potential barriers to offering HIV tests. Other questions concerned resident demographics, included age, sex, years since medical school graduation, and current postgraduate year (PGY). Each respondent's residency program setting (university-affiliated community hospital or university hospital) was verified by searching the American Medical Association Residency and Fellowship Database.
Best practice alert for HIV testing
Aggregate data on HIV tests ordered, by primary care providers and residents combined, at 35 federally qualified community health centers across the Chicago area from July 2015 to February 2016 were collected. All of the centers used electronic medical records. In July 2015, the centers introduced a best practice alert into their electronic medical records as a reminder for medical providers to offer HIV testing. The alert appeared if the medical record did not indicate that a prior HIV test had been resulted for that patient. Adherence to the testing recommendation was measured at the clinical level by dividing the number of patients who underwent HIV screening by the number of patients who should have undergone HIV tests according to the best practice alert generated at the time of each clinic visit.
Statistical analyses
Frequencies were used to describe and summarize the data. Bivariate analyses using Wald chi-square tests were used to examine the association of knowledge related to HIV testing and CDC guidelines with selected variables, including the residency program setting, years since medical school graduation, current PGY, and reported formal education or training in HIV testing. Separate bivariate analyses were used to examine the association of practice behaviors related to HIV testing with selected variables. P values less than 0.05 were considered significant. Statistical analysis was done using the SPSS software (version 24; IBM Corporation, Armonk, NY).
The survey included disclosures and statements necessary to serve as documentation of consent from the respondents by completing the survey. Aggregate data on HIV testing volume were gathered without any identifiers. This study was reviewed and approved by the institutional review board.
Results
Study population
Four of 13 residency programs in the Chicago area took part in this study. Participating and nonparticipating programs were similar in respect to age and gender of residents. 18,19
Of the 192 residents surveyed, 130 completed the survey for a response rate of 68%. The majority of respondents were 25–34 years old (90%), training in university-affiliated community hospital residency programs (91%), and male (61%). Twenty-five residents (19%) had graduated from medical school at least 7 years before the survey, 47 (36%) had graduated 4–6 years prior, and 56 (43%) had graduated 1–3 years prior. Respondents were almost equally distributed in three PGY groups (Table 1). Three of the residents' hospitals were located in the inner city of Chicago, whereas the fourth was located in a northern suburb.
The number of responses varied as some residents skipped some questions.
PGY, postgraduate year.
Knowledge about HIV testing and CDC HIV testing guidelines
Most of the residents (82%) reported receiving some form of training or education about HIV screening guidelines in medical school or their residencies. Sixty-six percent knew that men having sex with men is the most common mode of HIV transmission in Chicago, 20% thought that heterosexual contact is the most common mode of transmission, and 14% believed intravenous drug use to be the most common mode. Only 58% of the residents were aware that the CDC recommended screening in patients regardless of their HIV risk factors, whereas 39% thought that the most recent CDC recommendation is to screen patients if they have any HIV risk factors. Similarly, only 73 residents (56%) knew that patients at high risk for HIV infection should be tested annually. Less than half of the respondents (49%) were aware that Illinois law allows an opt-out HIV testing strategy and 48% thought that a written or separate HIV consent is required before testing (Table 2).
The number of responses varied as some residents skipped some questions.
CDC, Centers for Disease Control and Prevention.
Regarding the four questions gauging respondents' knowledge of HIV testing, 11% of residents answered all four questions correctly, 32% answered three questions correctly, 36% answered two questions correctly, and 21% answered only one question or none of the questions correctly. In our bivariate analysis, we did not find any associations between the number of questions answered correctly and age, sex, year of medical school graduation, PGY, residency program setting, and the presence or absence of lectures or training about HIV screening.
Practice of and barriers to HIV testing
Eighty-three residents (64%) ordered 10 or fewer HIV screening tests over the previous 6 months. Of these, six residents (7%) did not order any HIV tests over that period. Residents in PGY1 were significantly less likely to order more than 10 HIV tests than were those in PGY2 or PGY3 (22%, 50%, and 35%, respectively; p = 0.03). No other variables were associated with the number of HIV tests ordered. Sixty-two respondents (48%) occasionally or never asked patients about their high-risk sexual behavior, including number of partners, sexual orientation, and use of condoms, whereas 66 (51%) always or most often asked patients about their sexual history.
We did not observe a correlation between overall knowledge score and number of HIV tests ordered. The most frequently reported barriers to ordering HIV testing were deferral because of urgent care issues (31%), lack of time (29%), and the perception that patients were uncomfortable discussing HIV testing (23%). Other barriers included lack of training in handling positive HIV test results (5%), unfamiliarity with the patient in the first encounter (15%), and language barriers (7%). Seven residents (5%) cited difficulty in finding a written consent form as a barrier.
Adherence to HIV testing guidelines in 35 federally qualified community health centers across Chicago
The data on the 35 federally qualified community health centers in Chicago that we analyzed demonstrated an average of 21,000 clinical encounters per month in which a best practice alert for HIV testing was recommended (Fig. 1). In July 2015, the first month after introduction of the best practice alert into electronic medical records to remind all medical providers about HIV testing, the percentage of HIV tests ordered per clinic visit was 20.6%. However, the percentage decreased to 16.6% in November 2015. The percentage of HIV tests per clinic increased slightly to 18.4% in February 2016. Overall, from July 2015 to February 2016, the average adherence rate was 18.2%.
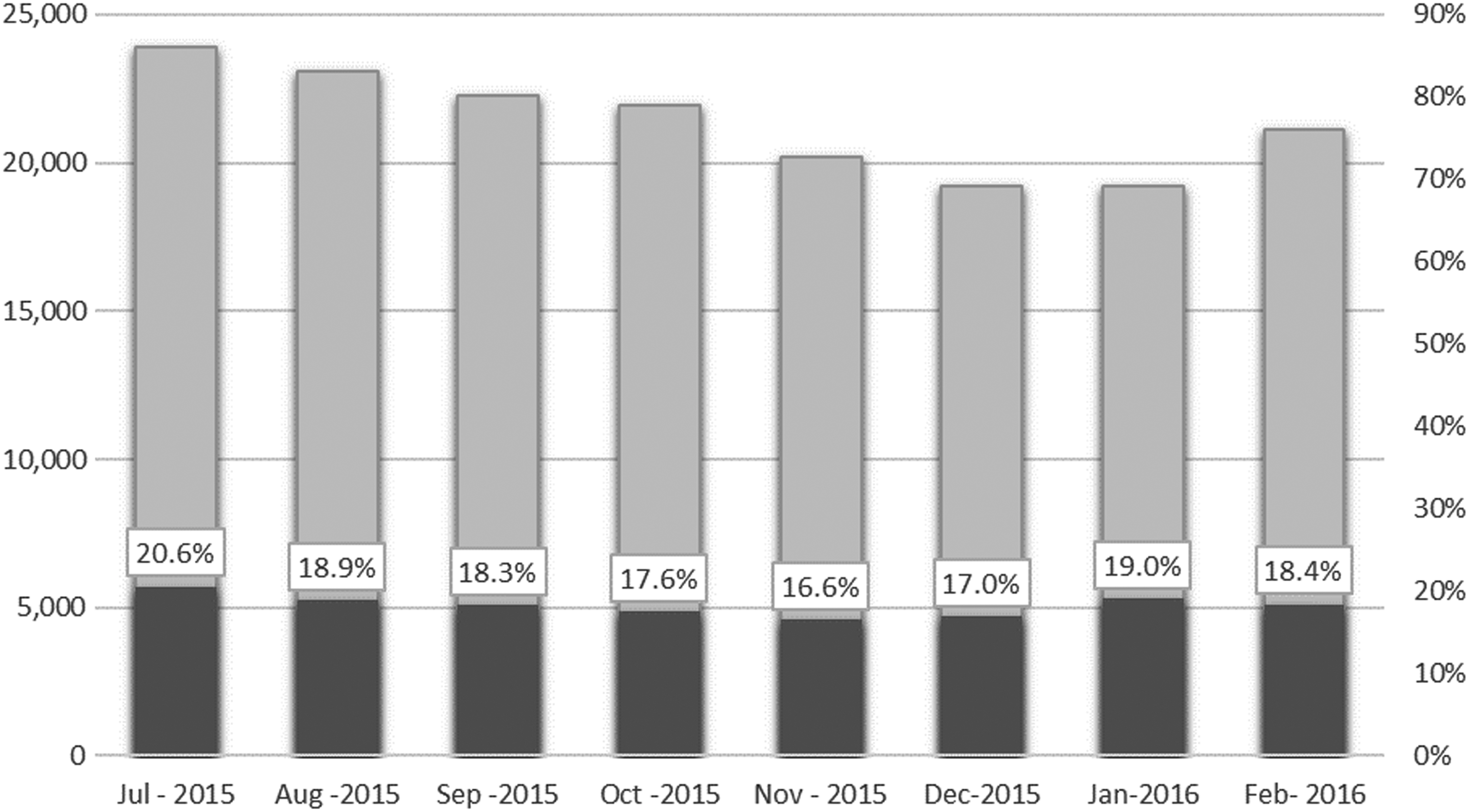
The numbers of clinical encounters in which a best practice alert for HIV testing was recommended at 35 federally qualified healthcare centers in the Chicago area (grey bar) and the numbers and percentages of HIV tests ordered (black bar) per month for the 8 months after the best practice alert was initiated.
Discussion
This study highlights a lack of knowledge regarding HIV screening among internal medicine residents and inadequate performance of routine HIV testing in the outpatient setting even after deployment of a best practice alert in the electronic medical record. Many residents were not aware of the CDC guidelines for HIV screening even though the survey was conducted 10 years after the release of these guidelines. Many residents also were not aware of the 2008 Illinois law allowing for opting out of HIV testing even though the law had been in effect for more than 8 years.
Illinois ranked sixth among all 50 states in the number of new HIV diagnoses in 2015. Male-to-male sex is the most common mode of HIV transmission nationwide and in Chicago (73%). 1 A third of the residents thought HIV testing should be based on infection risk factors. However, only 66% of them correctly identified male-to-male sex as the most common risk factor for HIV transmission. In addition, only 56% chose the correct testing frequency for patients with high-risk factors for HIV infection, and only 51% always asked patients about HIV risk factors or did so most of the time.
Despite this lack of knowledge among the residents, the percentage of internal medicine residents who responded correctly to the HIV testing knowledge questions was higher than that in a New York City study done just 1 year after the release of the CDC guidelines described above (66% vs. 20% knew the most common mode of HIV transmission, and 58% vs. 32% were aware that HIV screening should be offered regardless of risk factors). However, HIV testing rates remain low. The percentages of internal medicine residents who ordered more than 10 HIV tests in Chicago and New York City were similar (35% vs. 36%). 11
Lack of awareness of the revised CDC guidelines may contribute to infrequent HIV testing. However, attending formal lectures on and undergoing training in HIV testing and high knowledge scores in our study group did not correlate with good practice behaviors. In fact, residents cited factors unrelated to knowledge of HIV testing guidelines as barriers to HIV testing (e.g., lack of time, need to address more urgent medical problems, and perception that patients are uncomfortable discussing HIV testing). Studies among practicing physicians revealed similar barriers. For example, many healthcare providers have misconceptions about patients' attitudes toward HIV testing. 20 Contrary to provider assumptions, though, studies have demonstrated high acceptance rates for HIV testing among patients. 21,22
Our survey results are consistent with the very low HIV screening rates at the 35 community health centers across Chicago that we examined. We found almost 20,000 missed opportunities for HIV testing at these centers every month despite inclusion of the best practice alert in electronic medical records. This indicates that clinical reminders alone may not be enough to improve HIV testing behavior among healthcare providers. Interventions may have to target patient, provider, and healthcare system factors that drive HIV testing. Some strategies have focused on empowering patients to undergo HIV testing through HIV education programs, prompting patients to request testing and promoting self-testing. 23 Other interventions targeting the healthcare system and structural factors include the implementation of an opt-out strategy across all healthcare settings and removal of written consent and pretest counseling requirements. 24 –26 These interventions have had variable success. Our study indicates that beyond healthcare provider familiarity about HIV testing, patient activation, and removal of systemic barriers, interventions must target provider attitudes about HIV testing, such as the misconception that it takes substantial time to obtain consent for testing or that patients do not want to undergo HIV testing and will be offended if providers order it.
Our study was limited, in that we performed it only in Chicago; our results may not reflect those at other training programs. However, we included 192 residents at four different training programs and had a high response rate, so the results are likely externally valid. Some questions asked the residents to recall prior lectures and training concerning HIV testing and practice behaviors such as the number of HIV tests ordered. Responses to these questions are subject to recall bias. However, bias typically results in more favorable responses. Thus, the low reported rate of HIV testing behaviors is concerning, and the true rate may be even lower. Last, regarding our HIV testing adherence measure, we did not review patients' medical records to identify valid reasons for not ordering HIV testing. Medical providers may have offered HIV tests, and patients may have refused or had recent HIV tests at different locations not linked with their electronic medical records. However, this would likely account for only a small percentage of HIV tests, and our results are consistent with those of other studies among primary care providers. 27
To realize the goal of universal HIV screening, more efforts are needed to change the HIV testing practices among internal medicine residents. Developing strategies to increase HIV testing behavior among residents is critical because they are the front-line medical providers at many academic institutions and hospitals, and behaviors adopted in training are likely to stick and impact their practice over their ensuing career. Addressing knowledge barriers in ways beyond best practice alerts is essential for successful changes in practice behavior.
Footnotes
Acknowledgments
The authors thank Don Norwood of the Department of Scientific Publications at The University of Texas MD Anderson Cancer Center for editorial assistance. The authors acknowledge the residents who participated in the survey as well as those who administered it, including chief residents, Alvaro Altamirano, Roshanak Habibi, and Kushal Naha.
Author Disclosure Statement
No competing financial interests exist.