
Abstract
Pre-exposure prophylaxis (PrEP) is one of the most important milestones in HIV prevention for high-risk HIV-negative people. The introduction of PrEP into the HIV prevention package has raised the question of possible risk compensation, and in particular, a reduction in condom use. Although open-label extension (OLE) studies have enabled investigators to examine risk compensation in more real-life settings, results to date have been inconclusive regarding PrEP-induced behavioral changes. We aimed to identify behavioral trajectories over time for PrEP and condom use, and to investigate the link between these trajectories. Group-based trajectory modeling using logistic specification was implemented. Data of the 332 individuals participating in the double-blind and OLE phases of ANRS IPERGAY were used. Four distinct group trajectories were identified: 49.7% of the participants had “systematic adherence to PrEP,” 19% had “high adherence to PrEP, 15.3% had “declining adherence to PrEP,” and 16% had “low adherence to PrEP.” Two condom trajectories were identified: 53% (n = 176) of the 332 participants were “low-level users” of condoms, and 47% were “high-level users.” Among the former, 24.4% also belonged to the “low adherence to PrEP” group. This most-at-risk group represented 13% of all the participants. The effectiveness of offering sexual activity-based PrEP as part of the French HIV prevention package in the ANRS IPERGAY clinical trial is demonstrated by the relatively small proportion of participants that offset their low-level condom use with PrEP adherence. The results from this work may help in the future development of tailored prevention programs for high-risk HIV-negative people.
Introduction
I
The introduction of PrEP into the HIV prevention package has led to a vast amount of related literature. A large proportion of these studies focus on barriers and levers to PrEP uptake. Individual barriers include patient-perceived potential side effects and psychosocial factors, including stigma, depressive symptoms, and unawareness of PrEP effectiveness. 7 –10 The few studies to evoke structural barriers have only done so indirectly, highlighting both costs and resource allocation. 11,12 With respect to levers for PrEP uptake, the most important are support services, including HIV testing/monitoring and counselling. 13 –15 Although some of the studies exploring PrEP uptake highlight the close positive relationship between uptake and adherence, 8,16 –18 they concentrate on early adherence with little evidence about long-term dynamics, and cover a relatively short follow-up period. 17,19
While adherence is often presented as the cornerstone of the effectiveness of PrEP in clinical trials, few studies to date have investigated associated factors and patterns. 18,20 Adherence is often assessed using either direct or indirect measures (i.e., pharmacokinetic measures on blood, plasma, and/or urine, hair, product return count, or medication event monitoring system), 16,19,21 –23 although some studies assess it using patients' self-reports, either as the principal measure or to compare it with objective measures. 13,17,24 –27 In the latter studies, self-reported measures are seen as much less useful than objective measures. 25,27
All the studies cited above concern daily PrEP and research into on-demand PrEP is practically inexistent. On-demand PrEP brings with it significant methodological challenges in terms of measuring and analyzing adherence. In the ANRS IPERGAY trial, self-reported adherence appeared to be globally concordant with objective measures, and sometimes more accurate than objective measures such as pill count, especially during the OLE phase (where some participants were reluctant to return unused pills). 6 More specifically, collecting samples for objective measures after each episode of sexual intercourse is not really feasible. Further, the efficacy of such measures could be compromised in the context of on-demand PrEP. Measuring the concentration of TDF-FTC in plasma (as in the ANRS IPERGAY trial) could underestimate adherence, as the reliability of the measure is dependent on the length of time between the sexual intercourse event and scheduled blood sampling (i.e., longer intervals mean lower concentrations). Indeed, as suggested by Anderson et al., 28 on-demand PrEP pharmacokinetic forgiveness would be lower than daily PrEP. Using self-reported adherence is therefore crucial for the study of behavioral patterns in this context.
The introduction of PrEP into the HIV prevention package also raises the question of possible risk compensation, and in particular, whether condom use might decrease. Evidence for this is limited, 29 –33 although some studies have highlighted risk compensation, especially among young MSM, 34 and the importance of addressing this issue from the healthcare provider's viewpoint. 35 It should be noted that the absence of risk compensation in most double-blind studies to date was associated with modified behaviors arising from participants' uncertainties about whether they were taking placebo or not. 36 Although OLE studies enable investigators to examine risk compensation in individuals taking PrEP in more “realistic” settings, results to date have been inconclusive about related behavioral changes. 37 Longitudinal data from cohorts are rarely exploited to investigate the dynamics of PrEP adherence within a tailored framework. Existing literature often uses descriptive statistics for each follow-up time point, which implies that observations from one point to another are assumed to be independent. Most of the studies cited above lacked suitable methods to account for behavioral similarities across individuals, and to account for the follow-up as a whole. We argue that PrEP adherence trajectories evolve differently according to individual characteristics and psychosocial factors, and that these trajectories may modify over time depending on sexual behavior and risk perception. In addition, we contend that PrEP adherence and condom use are interrelated and cannot be studied separately. This article provides a better understanding of the patterns of PrEP adherence and their link to condom use. It is an important contribution to the existent literature, as little is known about risk compensation in the context of on-demand PrEP.
We used data from the double-blind and OLE phases of the ANRS IPERGAY trial to identify behavioral trajectories over time for PrEP adherence and condom use, and to investigate the link between these trajectories. To do this, we implemented an existing methodological framework to model group-based trajectories. 38 –41 Although widely used in different fields to study developmental trajectories, 42 –44 this framework has only recently been used in the field of HIV. Indeed, of the three related studies that we found in the literature, none examined PrEP. 45 –47 We first identified individuals' PrEP adherence and condom use trajectories, and then adopted a mixed-method perspective to provide some qualitative insight, to obtain a greater insight of the different trajectories of individuals participating in the ANRS IPERGAY trial.
Methods
Protocol and study population
ANRS IPERGAY was a double-blind randomized trial testing the efficacy of sexual activity-based antiretroviral PrEP in MSM, as part of combined prevention. It was conducted in France and Canada. In brief, the trial included HIV-negative males and transgender women who had sex with men, were ≥18 years of age, and reported anal sex with at least two different partners over the previous 6 months (i.e., at high risk of HIV acquisition). Participants were assigned either to the TDF-FTC regimen or placebo arms, and the following dosage scheme was prescribed: two pills intake between 2 and 24 h preceding sexual intercourse, followed by one pill 24 h and another 48 h after the first drug intake. Regular testing for HIV and other sexually transmitted infections (STIs) and individual tailored risk-reduction counseling, condoms, and lubricants were offered during the trial. The double-blind phase concluded in November 2014 with the discontinuation of the placebo arm. As indicated in the protocol, enrollment in an OLE study was then offered to all participants to guarantee their continued access to PrEP until its approval. A comprehensive description of ANRS IPERGAY, including the methodology and results, is presented in Molina et al. 5,6
This article includes information for 332 participants in both the double-blind phase and OLE phases (out of the 400 initially included in the double-blind phase). Data on sociodemographic characteristics, alcohol and recreational drug use, sexual behavior (number of episodes of sexual intercourse in the previous 4 weeks and number of sexual partners in the previous 2 months), and PrEP adherence during the most recent episode of sexual intercourse were collected through an online questionnaire every 2 months. Analyses were performed on the longitudinal information of the 332 participants practicing anal sex at least once during follow-up: double-blind phase (M0–M24) and OLE (M0–M18) corresponding to a maximum of 23 time points. The data of participants who acquired HIV during the trial were censored.
Outcomes
This analysis focuses on PrEP adherence and condom use during the most recent episode of anal intercourse (MRAI). Dichotomous variables were constructed for the 23 time points over the follow-up for the two outcomes. The first outcome indicated whether participants were adherent to PrEP ( = 1) or not ( = 0). More specifically, variables were equal to 0 when participants were not adherent (no pills taken within 48 h before and after sex), and equal to 1 for correct adherence to PrEP (at least one pill taken within 24 h before sex and one pill taken within 24 h after sex) or for suboptimal adherence (i.e., pills in a different time interval around the sexual encounter, or any other use). 5 The decision to group together “suboptimal” and “correct” adherence to construct our PrEP outcome was based on the fact that in the ANRS IPERGAY trial, no seroconverted person was categorized in the suboptimal adherence group 5,6 and that suboptimal adherence has been shown elsewhere to be effective. 48 The second outcome indicated whether participants used condoms ( = 1) during their MRAI or not ( = 0).
Covariates
The following sociodemographic and socioeconomic characteristics were considered in this analysis: age (specified as a continuous variable), education level (≤high school vs. >high school), and employment status (employed vs. unemployed). Sexual behavior variables included the following: (i) median number of episodes of sexual intercourse (in the previous 4 weeks); (ii) median number of sexual partners (in the previous 2 months) and awareness of most recent partner's HIV status (yes = 1/no = 0); (iii) risk perception during the MRAI (measured using a 0–10 scale indicating whether participants perceived no risk at all or very high risk), this variable was then dichotomized using the median of the sample (high = 1 when risk perception was ≥sample median; low = 0 otherwise); (iv) condomless most recent anal intercourse (CMRAI, yes = 1/no = 0); and (v) receptive position during the MRAI (yes = 1/no = 0). Variables concerning sexual behavior were specified as time-varying, as they were collected at each follow-up time point between M2 and M24 in the double-blind phase, and between M0 and M18 in the OLE.
Statistical analysis
Group-based trajectory modeling using logistic specification was implemented for two reasons: first, to identify behavioral trajectory patterns concerning PrEP adherence and condom use, and second, to investigate the link between these behaviors (i.e., dual trajectories). 39,41 One of the main advantages of this method is that it takes into account the presence of missing values, 40 and therefore, we were able to include participants with at least two observations available during the follow-up 49 (see Appendix 1 for more details about the identification of trajectories). The trajectories identified for each outcome were used to compare sociodemographic and behavioral characteristics of participants using either Khi-2 or Brown-Mood (median) tests. Analyses were carried out using SAS 9.4 software.
Qualitative data collection and analysis
The double-blind phase of the ANRS IPERGAY trial included optional participation in focus groups (FG), conducted and managed by community-based counselors. FG were conducted in the local premises of the NGO AIDES in five cities in France (Lille, Lyon, Nantes, Nice, and Paris) where ANRS-IPERGAY centers were established. These participative discussions fostered self-support and encouraged social sharing. They helped encourage participants to express their viewpoints on issues surrounding social identity through group debate, negotiation, and argumentation. 50,51 The study design ensured that the elicitation, observation, and analysis of representations 52 were particularly suitable to the ANRS IPERGAY trial, where sensitive issues such as sexual practices of MSM experiences were discussed.
Thirteen group interviews were analyzed, representing a sample of 45 participants (3–6 participants per FG). This qualitative approach 53,54 enabled us to understand and comprehensively analyze the daily life experience of participants, the meaning they gave to decision-making in terms of sexual life, and how they incorporated sexual activity-based PrEP uptake and adherence to PrEP into existing prevention strategies such as condom use. 55,56 The value of using this qualitative approach was therefore to understand more precisely—using explanations provided by participants —the different trajectories explored in a quantitative manner. Anonymous personal identifiers were used for each individual to investigate the PrEP adherence and condom use trajectories to which they belonged.
Results
Sample characteristics
Analyses were carried out using the data of the 332 individuals who participated in both the double-blind and OLE phases of ANRS IPERGAY. Over the follow-up, this corresponded to 2324 questionnaires with complete information on PrEP adherence, and 4223 with data on condom use. Participants were 36 [29–43] years old in median [interquartile range (IQR)], most had a high-school diploma or a higher qualification (73.9%), and most were employed (84.6%). The vast majority declared they were financially comfortable (93.3%) and only 23.2% declared experiencing stress related to PrEP side effects (Table 1). With regard to sexual behavior at baseline, the study sample reported a median [IQR] of 10 [5–17] sexual intercourse encounters in the previous 4 weeks, and eight sexual partners in the previous 2 months. Only 37.4% declared they knew their most recent partner's serology, 44.4% declared they used drugs, 58.0% had no main partner, and 50.8% perceived high risk during their MRAI.
Sample Characteristics of Participants in Both the Double-Blind Phase and Open-Label Extension (OLE)
Participants who declared anal intercourse at least once during follow-up (M1–M24).
Four missing values (at baseline, M0).
Six missing values (at baseline, M0).
Three missing values (at baseline, M0).
Four missing values (at baseline, M0).
Eight missing values (at baseline, M0).
Six missing values (at baseline, M0).
Eleven missing values (at baseline, M0).
Five missing values (at baseline, M0).
One missing values (at baseline, M0).
Included drugs are as follows: ecstasy, MDMA, cocaine, crack, GHB/GBL, speed, meta-amphetamine, crystal, and 14 missing values (at baseline, M0).
Six missing values (at baseline, M0).
GHB/GBL, gammahydroxybutyrate/gammabutyrolactone; IQR, interquartile range; MDMA, 3,4-methylenedioxymethamphetamine; MRAI, most recent episode of anal intercourse; OLE, open-label extension.
Trajectories of adherence to PrEP
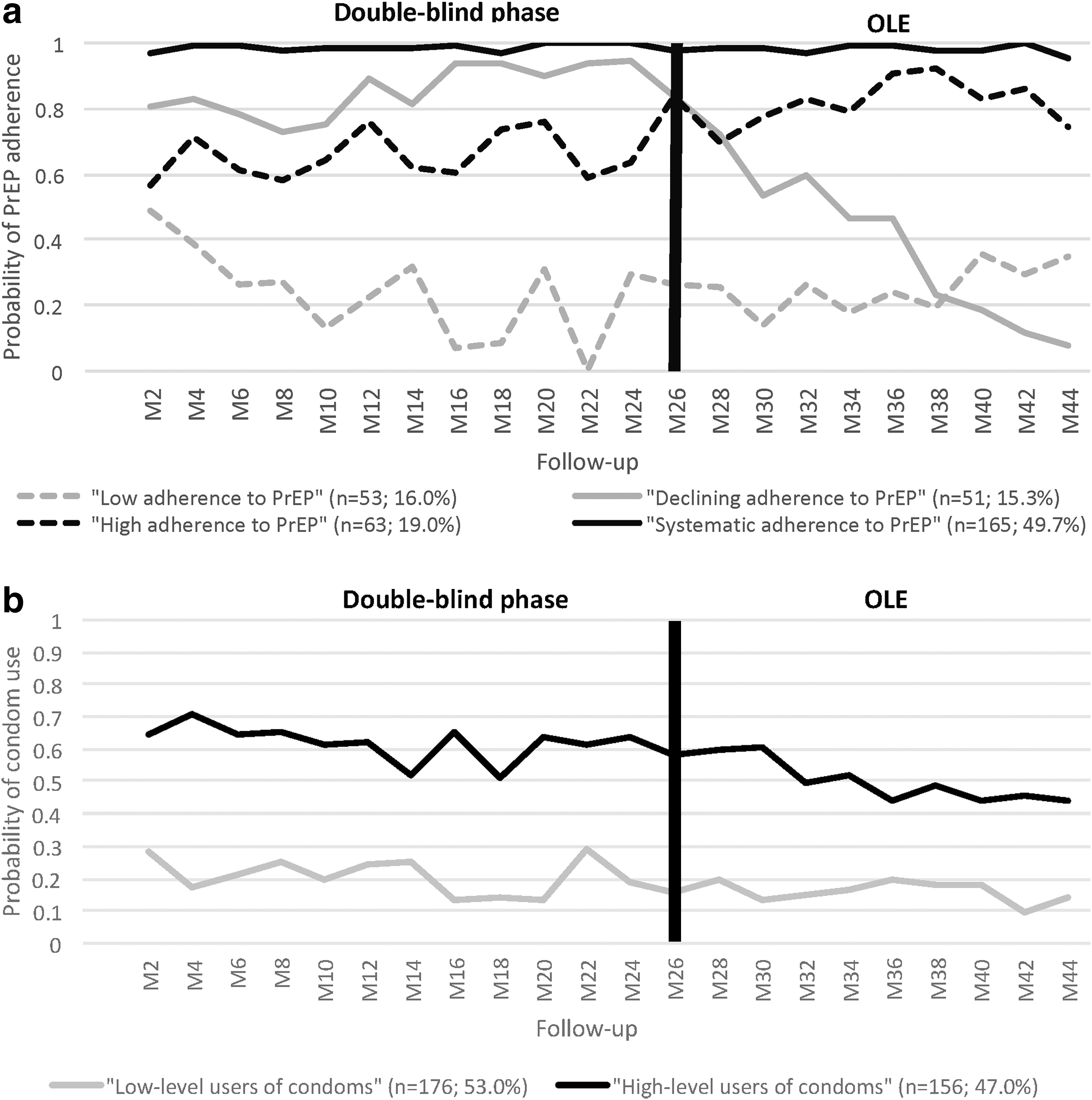
The best-fit model describing the patterns of PrEP adherence resulted in four distinct group trajectories (Fig. 1a) which we labeled as follows: “systematic adherence to PrEP” (accounting for 49.7% of the 332 participants), “high adherence to PrEP” (19%), “declining adherence to PrEP” (15.3%), and “low adherence to PrEP” (16%). Post-estimation characteristics (Table 2) showed a significant difference in terms of age (p < 0.001) between all four group trajectories, the low and systematic adherence groups being the youngest (median [IQR] age of 31 [25–37] years) and oldest (39 [31–46] years old) groups, respectively. In addition, most of the systematic adherence group were in active employment (p = 0.001, 88% vs. 77.4% and 68.6%, respectively, in the low and declining adherence groups) and declared the lowest number of sexual intercourse encounters at baseline (p = 0.012, median [IQR] of 8[5–15] vs. 10–15 for the other group trajectories). This group was also less likely to know their partners' HIV status (p = 0.024, 47.6% of total sexual intercourse encounters vs. 50.5%, 51.8%, and 53%, respectively, among the low, high, and declining adherence groups). However, those systematically adherent were the group most likely to declare perceived high risk at their MRAI (p < 0.001; 54.1% of total sexual intercourse encounters, vs. 38.3% among the low adherence group).
Post-Estimation Characteristics of Pre-Exposure Prophylaxis (PrEP) Adherence and Condom Use Trajectories (n = 332)
N = 332 participants (follow-up = M0).
N = 4728 questionnaires with complete information on condom use.
Among 298 participants reporting receptive anal intercourse: N = 2304 questionnaires with complete information on condom use.
N = 4667 questionnaires with complete information on risk perception.
Two missing values.
Three missing values.
Five missing values.
Seven missing values.
Chi-square test.
IQR, interquartile range; MRAI, most recent episode of anal intercourse; PrEP, pre-exposure prophylaxis.
Trajectories of condom use
Modeling trajectories for condom use resulted in two distinct groups (Fig. 1b) labeled “low-level users of condoms” and “high-level users of condoms,” reflecting 53% and 47%, respectively, of the 332 participants in the sample. Condoms were used in an average of 20% of the sexual intercourse episodes reported by low-level users of condoms, versus ∼60% in the group of high-level users of condoms. No significant differences were observed between these groups concerning individual characteristics, as shown by post-estimation characteristics (Table 2). Nevertheless, low-level users were more likely to know their most recent partner's HIV serology (57.1% vs. 41.8% among high-level users, p < 0.001), and more likely to perceive high risk during their MRAI (56.5% vs. 42.8 in high-level users p < 0.001). They also had the highest proportion of CMRAI (82% vs. 43.4% among participants in high-level users, p < 0.001).
The following section shows the factors associated with membership in a particular group trajectory and the factors explaining each trajectory's dynamics.
Changes over time in trajectories of adherence to PrEP
The trajectory of the systematic adherence to PrEP group (49.7% of all 332 participants) remained stable during the whole follow-up, with probabilities of PrEP adherence oscillating between 95% and 100% (Fig. 1a). This variability was principally associated with the number of sexual partners in the previous 2 months (coeff.: 1.02, p < 0.001) and perceived high risk during the MRAI (coeff.: 4.14, p < 0.001), which were both positively related with adherence to PrEP in this group (Table 3). The stability of this trajectory during both the double-blind and OLE phases could be explained by the intrinsic motivation of participants to be adherent to PrEP, reflected in the qualitative interviews conducted during the double-blind phase. It seems that experience gained over time allowed participants to integrate the on-demand PrEP schedule more easily into their everyday lives in terms of their sexual behavior: Participant 69026: “… in the protocol schedule: if I know that I'm going to have sex, [I take] two pills two hours before, and then in the following two days, at the same time, one pill…” Participant 79070: “… No, I don't necessarily take it all the time. I take breaks now and then. Sometimes I take a break” Interviewer T79: “Afterwards, do you find it difficult to get back to the schedule or has it become natural for you?” Participant 79070: “It is natu… Let's say, it's become a reflex”
Factors Associated with Pattern Evolution and with Belonging to a Given Pre-Exposure Prophylaxis (PrEP) Adherence or Condom Use Trajectory
Thirty-two missing value.
Twenty-three missing value.
p ≤ 0.05, ** p ≤ 0.01, *** p ≤ 0.001.
BIC, Bayesian Information Criterion; CI, confidence interval; MRAI, most recent episode of anal intercourse; OR, odds ratio; PrEP, pre-exposure prophylaxis; SE, standard error.
The trajectory of high adherence to PrEP group (19% of all 332 participants) was also quite stable with probabilities oscillating between 71% at M2 (double-blind phase) and 74% at M18 (OLE). The highest probability was ∼83%, estimated at M14 (OLE) (Fig. 1a). This probability was positively associated with practicing receptive anal sex (coeff.: 1.13, p < 0.05) and perceiving high risk during their MRAI (coeff.: 1.21, p < 0.01). However, condom use at MRAI (coeff.: −1.28, p < 0.01) and an increased number of sexual partners (coeff.: −0.04, p < 0.05) were associated with a lower probability of PrEP adherence among this group, as indicated by the negative relationship of these factors (Table 3). This irregular pattern of PrEP adherence also seemed to be related to the presence of a placebo arm, as the probability of PrEP adherence among this group increased from 63% at M24 (i.e., last time point of the double-blind phase) to 92% at M38 (i.e., during the OLE phase) (Fig. 1a).
Qualitative data collected among participants in this group trajectory during the double-blind phase suggested some difficulties complying with PrEP adherence reflected in nonsystematic adherence to PrEP. Not fully respecting the required time interval between intake and exposure observed in the following interview excerpt could provide one explanation for the irregular adherence trajectory among participants in this group: Participant 30116: “… well me, I always do it on demand. I take it pretty much always at least two hours in advance, maybe sometimes a little less, but I know that now after an hour it can be quite effective…”
In addition, neglecting PrEP post-exposure intake appeared to be another important explanation for the pattern observed for the high adherence group's trajectory, as suggested by the following conversation: Interviewer N85: “… And the tablets after, do they give you any problems?” Participant 30116: “Sometimes the second just slips my mind” Interviewer N85: “Why?” Participant 30116: “Totally forget” Interviewer N85: “Too long after having sex?” Participant 30116: “No, really, it's just forgotten, I was doing other things and so I completely forgot”
With respect to the declining adherence to PrEP group (15.3% of all 332 participants), substantial changes were observed in their pattern of adherence (Fig. 1a). During the double-blind phase, the probability of PrEP adherence in this group oscillated between 83% and 94%, whereas during the OLE phase, it decreased from 84% at baseline (M0, OLE) to only 8% at the end of the follow-up (M18, OLE). The multivariate model (Table 3) shows that the shape of this trajectory was principally driven by the number of sexual partners (coeff.: 0.07, p < 0.001), the latter being positively associated with the probability of PrEP adherence. Unobservable factors may also have contributed, at least partly, to explain this pattern, as suggested by the qualitative data: Participant 54002: “… when I first started the trial, actually it was something that I had very regularly in my head, to take the drug, even though I didn't always have the right dosing schedule in mind, and now, for about two-three months or so, because of a lot of STI, I've gone back to using condoms much more that at the start. So, for the last three months, I haven't taken any treatment, either before or after sexual intercourses. So it's much less present now, also because of going back to using condoms”
Indeed, some participants experienced a certain amount of despondence caused by the difficulty to integrate on-demand PrEP into their everyday lives. However, the preceding excerpt also suggests that these participants returned to the use of other prevention tools adapted to their behavior, such as the use of condoms.
The trajectory of low adherence to PrEP group (16% of all 332 participants) included probabilities approaching 50% at M2 in the double-blind phase that subsequently decreased rapidly. The lowest level observed in the double-blind phase was <10%. With regard to the OLE, a slight increase was seen at the beginning, but the probability then remained stable for the rest of the study, hovering around 20% (Fig. 1a). The shape of this trajectory is associated with the level of perceived risk during their most recent sexual intercourse encounter (Table 3). More specifically, estimations suggest that perceiving a high risk of infection during their MRAI was associated positively with the probability of adherence to PrEP (coeff.: 1.56, p < 0.001).
Qualitative data provide more information about the low adherence to PrEP. It seems that the motivation for participating in the trial, at least for some of the participants, was not directly related to access to PrEP, but to the concomitant advantages offered, including monitoring and testing in a community-based setting: Participant 79032: “My motivation, essentially, is purely a selfish one, it is really for the medical support that that comes with it. It was the chance to do a lot of blood tests that I had never done, except for STI and company, but … and also, let's be honest, to take advantage of the support for these medical tests. That was what interested me. On the one hand, it was a way of finding out how I was doing physically, etc., it is always quite reassuring to have these kinds of tests. It is also to benefit from community support, which I know little about”
In other words, for some, PrEP would simply appear to be an entry point into care. This suggests that its integration into the prevention system should take into account specific identity-based issues of certain members of the MSM community.
Changes over time in condom use trajectories
Table 3 shows that the pattern of both trajectories of condom use was shaped by the participants' awareness of their most recent partner's HIV status. This variable was significantly associated with decreased condom use in both trajectories, irrespective of whether the partner was HIV positive or not (coeff.: −1.27, p < 0.001 and coeff.: −1.13, p < 0.001 for low-level users of condoms and high-level users of condoms, respectively). In addition, the number of sexual intercourse encounters in the previous 4 weeks was negatively associated with condom use among this group (coeff.: −0.01, p = 0.01), whereas perceiving high risk during one's MRAI was negatively associated with condom use in both trajectories (coeff.: −1.95, p < 0.001 and coeff.: −1.95, p < 0.001 for low- and high-level users of condoms, respectively). Fixed-effects modeling showed that the probability of belonging to the low-level user trajectory was associated more with behavioral than individual characteristics (i.e., no significant association either with age or with education level). In addition, qualitative data showed continuity between condom-use behavior during the double-blind phase and before participation in the trial, both for low- and high-level users of condoms, respectively: Interviewer N85: “And how often do you use condoms today? Participant 30129: “Well, I don't use them, I never did, and I never will.” Interviewer W16: “and how does this increased attention show itself?” Participant 16035: “How does it show itself? Well, I'm more vigilant in the sense that … I put a condom on all the time since then, so there you have it. Participant 16019: Yes, I always have one on me. Always in the pocket …”
The link between adherence to PrEP and condom use trajectories
Dual group-based trajectory modeling enabled us to estimate the probability of PrEP use conditional on condom use. Among low-level users of condoms (n = 176), 71% offset their low use with high/systematic adherence to PrEP. Figure 2 shows that 40% and 31% of the 176 low-level users of condoms were systematically and highly adherent to PrEP, respectively. The remaining 29% were divided between declining adherence (16%) and low adherence (13%). The latter was therefore the most at-risk subgroup (i.e., constituting users who both used condoms less and had low adherence to PrEP). Among the 156 participants in the group of high-level users of condoms, 44% and 20% were systematically and highly adherent to PrEP, respectively. Accordingly, these two groups were the most protected. The breakdown of the remaining 36% was as follows: declining adherence to PrEP, 15%, and low adherence to PrEP, 21%.
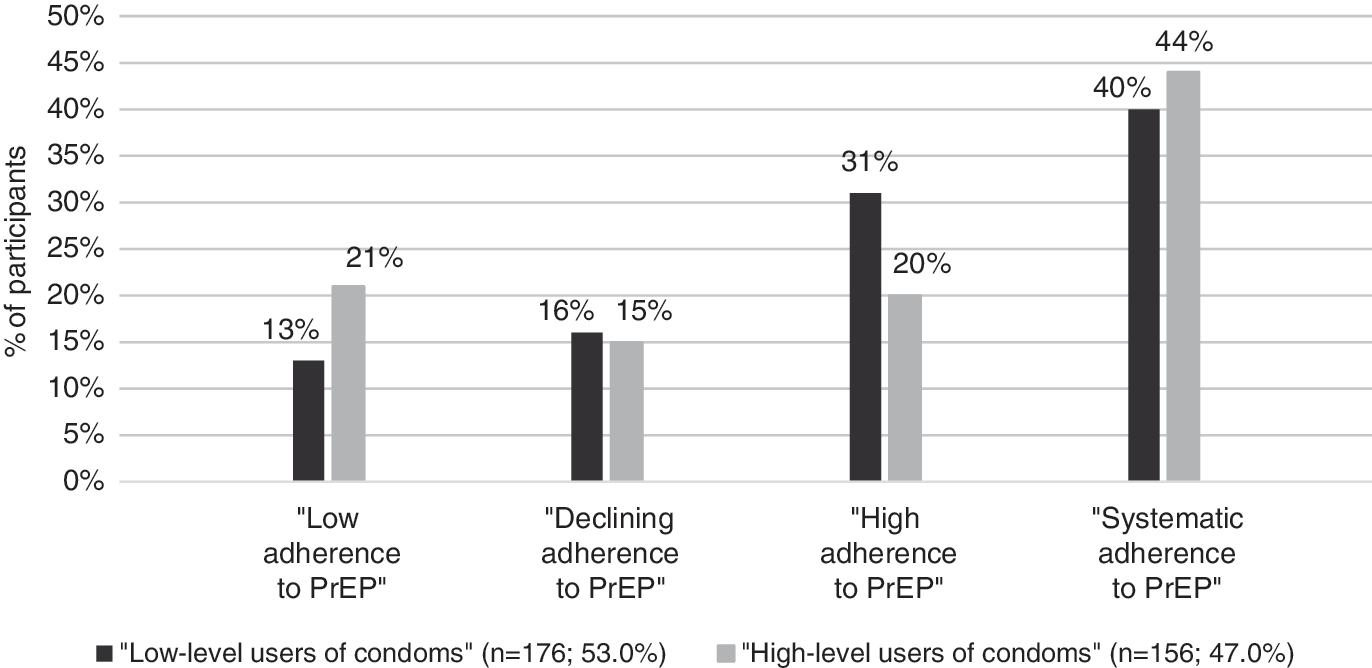
PrEP adherence according to condom use. (n = 176 in “low-level users of condoms”; n = 156 in “high-level users of condoms”). *Among the 156 participants in the high-level users of condoms group, 44% were in the systematic adherence group, 20% were in the high adherence group, 15% were in the declining adherence group, and 21% were in the low adherence group (the percentages by color total 100%). PrEP, pre-exposure prophylaxis.
The conditional probabilities estimated in the dual group-based model demonstrated that a large proportion of low-level users of condoms did not offset this use with increased adherence to PrEP. Further, a non-negligible proportion of low adherence to PrEP group were high-level users of condoms. In-depth information on PrEP adherence was obtained by stratifying the sample of participants according to their low- or high-level use of condoms, and reestimating the trajectories of PrEP use within these groups (Appendix 2).
Trajectories of adherence to PrEP among high-level users of condoms
Among high-level users of condoms (n = 156 participants), 71.8% were highly adherent to PrEP and were therefore the most protected of all trial participants (Fig. A2.1). For these individuals, PrEP seemed to be integrated as a complement to their other prevention strategies: Participant 30128: “I tell myself, combining the two, from … anyway, combining the percentage of the use of condoms and the treatment, yes. Then, combining one hundred percent condoms—for those who manage to do so—and the treatment, I don't really see the point. But yes, having both at the same time, that's a little like how I live it at the moment.”
Simultaneous high adherence to PrEP and high-level use of condoms did not appear to be a behavior produced by the uncertainty of being in the placebo arm, as it persisted during the OLE (i.e., stable trajectory during both the double-blind and OLE phases). The probability of PrEP adherence oscillated between 86% and 100% over both phases. Indeed, for some participants in this trajectory, participation in the trial seemed to have motivated increased condom use in their combination strategy: Participant 16019: “On the other hand, it [participation in the trial] might have improved the feeling. When we fuck, we're more at ease putting on a condom, so it's a little less constraining, actually. So maybe it improves it at that level. It certainly improves it at that level.”
Table A2.1 shows that participants with high adherence to PrEP, who were also high-level users of condoms, tended to be older (p = 0.085). They were more likely to be employed (p = 0.004) and report perceiving high risk during their MRAI (p < 0.001), but less likely to know the HIV status of their most recent partner (p = 0.028) than those in the group who were high-level users of condoms, but who had low adherence to PrEP (i.e., 28.2% of the 156 high-level users of condoms). The latter offset this low adherence with high-level use of condoms, and so remained protected. The onset of STI could be one of the possible explanations for the preference for the relatively higher level of condom use than PrEP adherence in this group: Participant 54002: “… So, the idea of having access to screening and treatment, like that, in a setting other than through the attending doctor, is quite convenient. And then, as I said, I use condoms a lot more, but I don't know if that's due to the trial … well, for sure it's due to the STIs that I caught. A little tired of getting STIs, so I probably would have used condoms more, even if I hadn't been in the trial, like, it's really the fact that I can have access to screening and treatment for STIs without going through an attending doctor[…] “So, in one of my last answers when I spoke about double protection, I realized, like an idiot, that since going back much more frequently to using condoms, I had stopped the treatment; so I say to myself: it's a bit stupid, because all you need is for the condom to burst or … so there you go, I don't know what can happen, but suddenly I say to myself: I myself stopped double protection, which is a bit dumb.”
This excerpt also reflects the difficulty for some participants to integrate PrEP as a prevention tool in a combined strategy when attention is diverted by exceptional events such as an STI. It was only during the focus group that the participant realized that excluding PrEP deprived him of the benefits of combined prevention, especially if a condom burst.
Trajectories of adherence to PrEP among low-level users of condoms
Among low-level users of condoms (n = 176), 75.6% were highly adherent to PrEP (Fig. A2.2). The qualitative data suggested that for some of these participants, condom use was not part of their routine risk-reduction strategy: Participant 54004: “…No, there has been no change, but I know I have risky practices, that is to say, I'm a bit fed up with condoms, so I almost tend to ask my partner not to use them. However, I do take the tablets regularly.”
For others, it seems that participation in the trial may have motivated them to abandon condoms for PrEP: Participant 20131: “Actually, I'm taking more risks since joining the IPERGAY trial. Even though I took them before, now I … well, for me condoms are … they don't exist for me anymore, like, I don't use them anymore, I take my Truvada.”
Table A2.1 shows that participants with a low-level use of condoms, but with high adherence to PrEP were older (p = 0.003). They were also more likely to be employed (p = 0.006), to have perceived high risk during their MRAI (p < 0.001), and to have a fewer number of sexual intercourse encounters (p = 0.034) than participants with low-level use of condoms, who also had low adherence to PrEP (i.e., 24.4% of the 176 participants). Indeed, the latter seemed to be at an ever greater risk of HIV infection as they progressed through follow-up, as their already low adherence to PrEP decreased further in both the double-blind and OLE phases (Fig. A2.2).
Discussion
The group-based model implemented on data from the double-blind and OLE phases of the ANRS IPERGAY trial confirmed our hypothesis that trajectories of PrEP adherence evolve differently over time according to sociodemographic and behavioral characteristics, and that these trajectories are linked to condom use patterns. Our study using quantitative data contributes to the existing literature by providing a greater understanding of sexual decision-making and a greater insight of how participants incorporate sexual activity-based PrEP into existing prevention strategies such as condom use. The complementary qualitative data we collected enabled us to better understand the sometimes atypical trajectories combining PrEP adherence and condom use, and showed how trajectories correspond to the real-life context of participants. The high level of protection against HIV infection in MSM demonstrated by sexual activity-based PrEP adherence in the ANRS IPERGAY trial 5 was confirmed by the fact that 68.7% of the participants belonged to prevention trajectories that encompassed either high or systematic PrEP adherence during the follow-up.
This study highlights the importance of distinguishing between different patterns, as doing so leads to a better understanding of participants' PrEP adherence behaviors. Our results, based on both the double-blind phase and OLE phases, demonstrated that behavior modification due to uncertainty about belonging to the trial's placebo arm, as suggested in some studies, 36,57 cannot be generalized. The discontinuation of the placebo arm in the ANRS IPERGAY trial highlighted the presence of a group of participants (49.7% among 332) for whom PrEP was fully integrated into their everyday lives, displaying a stable pattern of PrEP systematic adherence during the whole period of observation. In addition, some participants increased their adherence to PrEP after the double-blind phase of the study (i.e., once they knew that the placebo arm had ended). However, 15.3% of the total 332 participants considerably reduced their adherence to PrEP during OLE. This suggests the difficulty of integrating this prevention tool in their risk-reduction strategies. Although the existing literature highlights the perceived high risk of HIV infection as a facilitator of PrEP uptake and/or adherence, 10,30,58 our results demonstrated that its importance may vary across groups with different behavioral patterns. More specifically, risk perception played an important role in the decision to adhere systematically to PrEP, but did not concern participants for whom adherence to PrEP declined rapidly during the OLE phase. For the latter, the dynamics of PrEP adherence (stable during the double-blind phase and declining during the OLE phase) were explained—at least partly—by the modification of sexual practices, such as the reduction in the number of sexual partners. This contrasts with some studies that concluded there is no relationship between the willingness to use PrEP and the number of partners. 12
There was a strong suggestion that participants (n = 63, 19% of the sample) in the high adherence to PrEP group offset condom use with PrEP. In line with other studies, among this group, the higher the number of reported episodes of condomless anal intercourse, the higher was the probability of adherence. 12,31 The demonstrated efficacy of sexual activity-based PrEP and the subsequent discontinuation of the placebo arm at the end of double-blind phase would confirm this suggestion. The probability of PrEP adherence among participants in this highly adherent group increased at a faster pace from the beginning of OLE, especially for participants reporting condomless MRAI, practicing receptive anal sex, having perceived high risk during the MRAI, and having a reduced number of sexual partners in the previous 2 months. The less common use of condoms and the “less risky” characteristics of this group reflect the findings of Carlo Hojilla et al. 29 who assumed that an established level of trust existed between participants and their sexual partners.
Our results concerning the dynamics of PrEP adherence confirm the results of previous analyses using the same data, 33 carried out using descriptive statistics. However, our study, which used a suitable model, found that 53% of participants had a low-level use of condoms. This contrasts with results from those previous analyses, perhaps because they were often based on simple descriptive statistics. Our observed dynamics show that modifications in condom use behavior may occur even during the double-blind phase of a trial, contrary to what Alaei et al. 57 suggested, and may persist during OLE. One striking result in this article is the negative relationship between perceiving high risk during the MRAI and the likelihood of condom use in both low- and high-level condom use trajectories. The question that emerges from this is whether or not participants who perceived a high risk of HIV infection during their MRAI and who stopped using condoms, decided to protect themselves during sexual intercourse by adhering to PrEP. Our tailor-made dual group-based trajectory estimation method, which took into consideration information for the whole follow-up, is another important contribution to the existing literature, as it allowed us to look deeper into this issue, and provides further evidence about the link between PrEP adherence and condom use.
We estimated that 133 (75.6% out of 176) participants in the low-level use of condoms group were also highly adherent to PrEP. The necessity to retain the benefits of condomless sex, such as intimacy and greater pleasure, may be one plausible explanation for this combined prevention strategy. Indeed, this strategy seems to correspond to a need to adhere to PrEP not simply as a pure HIV risk-reduction strategy but also for the additional benefits it brings, such as the reduction of the intimacy-inhibition effect of using condoms. 59 In addition, the relatively higher proportion of participants perceiving a high risk of HIV infection during their MRAI in this group suggests that PrEP adherence is a better strategy to reduce anxiety related to HIV infection than condoms. 60
In general, our results demonstrate that participants protected their sexual intercourse encounters using PrEP and/or condoms during both the double-blind and OLE phases. Most participants offset low adherence to PrEP with high-level use of condoms or vice versa during follow-up. However, our estimations of joint PrEP adherence and condom use trajectories highlighted the presence of a group of 43 participants who did not use either strategy during follow-up. This most-at-risk group represented 13% of all the participants in both the double-blind phase and OLE phase of the ANRS IPERGAY trial. With respect to participants with high adherence to PrEP and/or condom use (i.e., those most protected), these 43 participants were younger, less educated, less likely to be employed, had a higher number of sexual intercourse encounters, and perceived low risk of HIV infection during their MRAI (Table A2.1 in Appendix 2). Awareness of partners' HIV status was also a characteristic of this most at-risk group, which suggests that they adopted other health prevention strategies, including counseling, TasP, and/or seroadaptation, as suggested by the existing literature. 14,29,61
Our findings should be interpreted and utilized with caution, as there are study limitations. First, analyses are based on self-reported data and the possibility of social desirability bias cannot be excluded. One of the main consequences of this bias would be the overestimation of PrEP adherence and/or condom use. However, in the on-demand PrEP context of the ANRS IPERGAY trial, self-reported adherence could be more accurate than objective assessment methods to describe long-term behavioral patterns. More specifically, self-report eliminates possible underestimation by, for example, TDF-FTC measurement in plasma, resulting from a long-time interval between the most recent sexual intercourse encounter (i.e., the time of PrEP use) and the scheduled clinical visit. In this context, self-reported adherence through online questionnaires every 8 weeks not only provides cost-effective advantages 25 but also reduces both recall and social desirability bias. 62 Although some studies in different contexts have pointed out low concordance between self-reports and objective measures, 20,25,27,63 in the iPrEx OLE study, self-reporting recent PrEP use was a strong predictor of concentration in plasma. 24 This supports our decision to also use self-reported measures in the on-demand PrEP context, as they can be seen as a succession of multiple recent measures of PrEP use. In addition, overreporting of PrEP use associated with the youngest and least educated participants in the iPrEx OLE study, was less likely to occur in our study as participants were older (median age [IQR]: 36 [29–43] years in both phases in the ANRS IPERGAY trial vs. 29 [22–36] years in the iPrEx OLE study), and had a higher educational level (73.9% with post-secondary education vs. 47%).
The second limitation of this study is that our results cannot be extrapolated either to the whole population of MSM or to the general population, as the ANRS IPERGAY trial targeted specific MSM profiles (e.g., those most at risk and those most motivated to participate in an HIV prevention clinical trial). However, our results demonstrate that behavioral differences in terms of PrEP adherence may exist even among a specific population of MSM. Existing literature attributes differences in PrEP use to demographic characteristics such as race 64 and age. 65 This work contributes to this literature by demonstrating that patterns of PrEP adherence are related to sexual behavior (e.g., number of partners and number of sexual intercourse encounters) and/or to psychosocial aspects (especially risk perception of HIV infection), as well as to behavior concerning the use of other prevention methods such as condoms. Our findings are important for the development of novel evidence-based behavioral strategies for HIV prevention, especially in the on-demand PrEP context. In France, the role of general practitioners is very limited in terms of PrEP provision. They are only able to renew prescriptions made by HIV specialists. This limited role slows down PrEP scale-up 66 and harms medical credibility. 64,65 A greater understanding of both PrEP adherence patterns and the factors involved in people's decision to use PrEP or not, may help general practitioners catch up in terms of PrEP prescription, and lead to large scale-up of PrEP.
Despite these limitations, the effectiveness of the ANRS IPERGAY clinical trial in introducing the offer of sexual activity-based PrEP into the French package for HIV prevention is demonstrated by the relatively small proportion of participants who offset their low-level condom use with PrEP adherence, something that persisted even in the more real-life setting of the OLE study. Special attention must be paid to the most at-risk population (i.e., low-level use of condoms and low adherence to PrEP), which our analysis highlighted. Further research is needed to understand what motivated them to sign up for this risk-reduction trial (ANRS IPERGAY trial). The results from such research may help to develop tailored prevention programs for this population.
Footnotes
Acknowledgments
We would like to thank the study's participants for their time and dedication to this research to benefit their community. We also thank the AIDES community advocacy group and their community peer counselors who made this study possible through their availability and continuous interaction with the participants and study staff at study sites and, most importantly, between scheduled visits (J.M. Le Gall, S. Morel, V. Pechenot, S. Bagge, A. Djessima Taba, M. Danet, K. Moudachirou, B. Dos Santos, J. Lambec, S. Rouby, X. Teruin, N. Dumon, V. Coquelin, P. Brunet, L. Gilly, T. Cepitelli, R. Porion, D. Rojas Castro, and B. Spire). We thank our community advisory board for its continuous support during the study (S. Karon [secretary], D. Villard [Action Santé Alternative], J.M. Astor [Boucle Rouge], D. Ganaye [Federation LGBT], T. Craig [Act-Up], B. Brive [J'y suis j'y reste], R. Orioli [Les Flamands Roses], M. Vanhedde (Solidarite SIDA), H. Baudoin (Sida Info Service), H. Fisher [TRT-5], and the Gay communities in France and Canada [COQSIDA, REZO]), who supported this work, Drs. S. Becker, P.S. Sow, J. Presley, and M. Aikenhead at the Bill and Melinda Gates foundation for fruitful discussions and funding, Dr. J.F. Rooney, A. Cheng, H. Jaffe, C. Rabian, and P. Petour at Gilead Sciences for donating study drugs, and members of the Independent Data and Safety Monitoring Board for their expertise and guidance (Drs. D. Costagliola [Chair], Y. Yazdanpanah, V.-K. Nguyen, A.-M. Taburet, and C. Taéron).
The ANRS IPERGAY Study Group: J.-M. Molina (coordinator), C. Capitant, B. Spire, G. Pialoux, L. Cotte, I. Charreau, C. Tremblay, J.-M. Le Gall, E. Cua, A. Pasquet, F. Raffi, C. Pintado, C. Chidiac, J. Chas, P. Charbonneau, C. Delaugerre, M. Suzan-Monti, B. Loze, J. Fonsart, G. Peytavin, A. Cheret, J. Timsit, G. Girard, N. Lorente, M. Préau, J.F. Rooney, M.A. Wainberg, D. Thompson, W. Rozenbaum, V. Doré, L. Marchand, M.-C. Simon, N. Etien, J.-P. Aboulker, L. Meyer, and J.-F. Delfraissy.
Participating Hospitals and Investigators: Paris St-Louis: C. Pintado, B. Loze, C. Delaugerre, P. Charbonneau, C. Gatey, D. Ponscarme, P. Penot, L. Niedbalski, R. Veron, J. Delgado, E. Dalle, S. Parlier, I. Madelaine, J. Fonsart, M. Danet, N. Mahjoub, N. Mezreb, K. Moudachirou, S. Morel, G. Conort, F. Lorho, M. Meunier, W. Rozenbaum, and J.M. Molina; Paris Tenon: J. Chas, C. Monfort, J. Foucoin, B. Boissavy, S. Cousseau, S. Huon, M. Danet, A. Djessima, V. Berrebi, A. Adda, S. le Nagat, L. Zarka, J. Berdougo, and G. Pialoux; Lyon: C. Chidiac, N. Mzoughi, F. Clement, A. Decouty, C. Chapolard, M. Godinot, C. Adouard-groslafeige, J. Koffi, A. Pansu, A. Becker, S. Pailhes, F. Bonnet, F. Jeanblanc, C. Brochier, X. Teruin, S. Rouby, and L. Gilly, and L. Cotte; Montréal: C. Beauvais, P. Arlotto, C. Fortin, A. Talbot, A. Chamberland, A. McKenzie, M. Blanchette, R. Rousseau, K. Montheuth, D. Thompson, M. Morin, M. Wainberg, and C. Tremblay; Nice: C. Etienne, F. Tolonin, S. Breaud, V. Péchenot, S. Bagge, T. Cepitelli, P.M. Roger, E. Rosenthal, and E. Cua; Tourcoing: A. Cheret, P. Cornavin, S. Vandamme, J. Lambec, N. Dumon, O. Leclanche, T. Huleux, R. Biekre, O. Robineau, H. Melliez, H. Bazus, and A. Pasquet; Nantes: C. Bernaud, M. Besnier, B. Bonnet, N. Hall, M. Cavellec, H. Hue, L. Larmet, M. Colas, R. Choquet, and F. Raffi. Finally, we would like to thank Bakridine M'madi Mrenda for statistical assistance and Jude Sweeney for revising and editing the article. This work was sponsored by the ANRS (France Recherche Nord and Sud Sida-HIV Hépatites) and funded by ANRS, the Canadian HIV Trials Network, the Fonds de dotation Pierre Bergé pour la Prévention—SIDACTION, and the Bill and Melinda Gates Foundation
Author Disclosure Statement
No competing financial interests exist.
Appendix 1
The optimal number of trajectories for each of the two outcomes [pre-exposure prophylaxis (PrEP) adherence and condom use] was identified based on the joint estimation of a polynomial regression—to define both the shape of the trajectory over time—and a multinomial function to estimate posterior probabilities of trajectory membership for each individual. The best-fit model was selected using a combination of: (i) the Bayesian Information Criterion (BIC) (i.e., the highest BIC indicates the best-fit model), (ii) a minimum mean posterior probability membership for each group around 0.7, and (iii) a minimum of 5% of participants in each category. 38,39,41 Covariates of interest were then included to identify time-varying factors associated with the shape of the trajectories, and the individual characteristics determining group membership. Given the estimation of the optimal number of trajectories for both PrEP adherence and condom use, dual group-based trajectory modeling was implemented to investigate the link between these behaviors. This dual group-based model enabled us to estimate the conditional probabilities of membership of a given PrEP-use trajectory group for participants who were already members of a specific condom-use trajectory group.
Appendix 2. Estimated Trajectories of PrEP Adherence According to Condom Use
Post-Estimation Characteristics of PrEP Adherence According to Condom Use Trajectories (n = 332)
| “Low-level users of condoms” (N = 176) | “High-level users of condoms” (N = 156) | |||||
|---|---|---|---|---|---|---|
| Median [IQR] or n (%) | “Low adherence to PrEP” (38.4%) | “High adherence to PrEP” (61.6%) | p† | “Low adherence to PrEP” (25.2%) | “High adherence to PrEP” (74.8%) | p† |
| Age 1 | 33 [27–41] | 39 [31–45] | 0.003 | 31 [23–40] | 35[30–43] | 0.085 |
| Educational level 1 | ||||||
| ≤High school | 11 (25.6) | 42 (32.1) | 0.423 | 10 (22.7) | 23 (20.7) | 0.783 |
| >High school | 32 (74.4) | 89 (67.9) | 34 (77.3) | 88 (79.3) | ||
| Active employment 1 | ||||||
| Yes | 31 (27.9) | 118 (89.4) | 0.006 | 31 (70.5) | 99 (89.2) | 0.004 |
| No | 12 (72.1) | 14 (10.6) | 13 (29.5) | 12 (10.8) | ||
| Stressed about side effects 1 | ||||||
| No | 29 (69.1) | 104 (79.4) | 32 (72.7) | 86 (78.2) | ||
| Yes | 13 (30.9) | 27 (20.6) | 0.167 | 12 (27.3) | 24 (21.8) | 0.470 |
| Behavioral characteristics | ||||||
| Median number of sexual intercourse encounters at M0 (previous 4 weeks) 1 | 15 [8–20] | 10 [5–18] | 0.034 | 10 [4–15] | 10 [5–15] | 0.820 |
| Median number of sexual partners at M0 (previous 2 months) 1 | 10 [5–20] | 8 [5–16] | 0.106 | 8 [5–15] | 8 [3–15] | 0.877 |
| Condomless anal intercourse at most recent encounter (insertive) or receptive) 2 | 461 (83.5) | 1516 (81.6) | 0.291 | 262 (43.0) | 740 (43.3) | 0.897 |
| Condomless receptive anal intercourse at most recent encounter 2 | 313 (88.7) | 830 (89.8) | 0.546 | 158 (57.5) | 415 (55.2) | 0.517 |
| Knew most recent partner's serostatus 2 | 353 (59.2) | 1099 (56.5) | 0.235 | 292 (45.5) | 725 (40.5) | 0.028 |
| Risk perception during MRAI 2 | ||||||
| Risk perception <median | 295 (54.4) | 740 (40.3) | 383 (64.0) | 928 (54.8) | ||
| Risk perception ≥ median | 247 (45.6) | 1095 (59.7) | <0.0001 | 215 (36.0) | 764 (45.2) | <0.0001 |
At baseline.
All available questionnaires (M0-M44).
Chi-square test.
IQR, interquartile range; MRAI, most recent episode of anal intercourse; PrEP, pre-exposure prophylaxis.