
Abstract
Youth perinatally HIV infected (PHIV) or HIV exposed, but uninfected (PHEU), are aging into adolescence and adulthood with multiple complex risk factors for mental health (MH) problems and poor MH treatment utilization. Our aims were to estimate prevalence of MH diagnoses, clinically significant symptoms, and MH treatment utilization among youth with PHIV and among PHEU youth, 10–22 years old. We also aimed to identify correlates of diagnoses and treatment utilization. Analyses of data from standardized interviews, behavioral assessments, and chart review of 551 youth revealed that 36% had a previous or current MH diagnosis, with no significant HIV status group differences. Prevalence of clinically significant symptoms was 15% for both groups, of whom a third had no diagnosis, and half were not receiving treatment. Among youth with a current MH diagnosis, those with PHIV had greater utilization of services than PHEU youth (67% vs. 51%; p = 0.04). Factors associated with MH diagnoses and/or treatment utilization included caregiver characteristics, age and sex of child, HIV status, and stressful life events. Prevalence of MH diagnoses was higher than in the general population, but lower than in similar perinatally HIV-exposed cohorts, with some unmet service needs, particularly in PHEU youth. Family characteristics warrant careful consideration in early diagnosis and treatment of MH problems among youth affected by HIV.
Introduction
C
Earlier investigations have identified a higher than expected prevalence of mental health (MH) problems among youth who are perinatally HIV exposed, regardless of infection status, as well as a constellation of associated biological, health, and psychosocial risk factors, of which HIV may not be primary. 5 –15 However, questions remain about the potential for changes to MH risk in the climate of life-long antiretroviral therapy (ART) exposure, accumulating stressful life events, and variable adherence to medications and healthcare as youth with HIV transition into adulthood. Adult and pediatric literature describe potential neurotoxic effects of HIV in those exposed or infected. 16,17 In addition, findings with regard to antiretroviral (ARV) exposure have been equivocal, with some exposures conveying a protective effect to the brain, and others being associated with neurocognitive or psychiatric risk. 18 –20
There is general agreement that youth perinatally exposed to HIV have elevated risk of MH problems, yet prevalence data across studies vary widely, due to methodological differences in outcome definitions, samples, measurement tools, and reporter. 21,22 The prevalence of MH diagnoses in the general population for youth 3–17 years of age ranged from 13% to 20%, 23 with even higher prevalence, up to 32%, observed in those studies limited to youth between 13 and 18 years of age. 24 Among youth with PHIV and PHEU, the prevalence of MH problems may be as high as 60–70%, 22 and include attention-deficit hyperactivity disorder (ADHD), conduct disorder, anxiety, and depression. 9,10,14,25,26
Risks associated with MH problems among youth with PHIV and PHEU youth are often accompanied by limited or inadequate MH treatment utilization. Among the general population, adolescents with MH problems are less likely to receive MH services than adults, and racial and ethnic minorities face additional barriers, and access MH treatment less frequently, than their white counterparts. 24,25 –28 In a US study of service utilization for lifetime mental disorders among a large nationally representative sample, 36% of 13- to 18-year-old youth with MH disorders received services. Half with severe disorders had never received MH treatment, and those who were Hispanic and non-Hispanic black, regardless of disease severity, were less likely than their white peers to receive MH care. 24
A number of unique HIV-associated barriers may moderate the utilization of services in the community of HIV-affected youth, including the additional perceived stigmatization of HIV. 29 Whiteley et al. surveyed a large cohort of 13- to 26-year-old youth with HIV infection and enrolled in the ATN (Adolescent Medicine Trials Network) for HIV/AIDS Interventions, regarding their utilization of MH care or psychotropic medications in the past 12 months. 30 Among 727 of 1706 (42.6%) youth who endorsed clinically significant MH symptoms, 39.7% reported utilization of MH care and 21.9% received psychotropic medications in the past year. 29
In another study examining the prevalence of MH diagnoses and treatment utilization among youth with PHIV and youth who were PHEU, the prevalence of psychiatric symptoms was similar (61%) in both groups, but the prevalence of behavioral interventions (27% vs. 17%) or prescribed psychiatric medications (23% vs. 12%) was higher in the PHIV group than the exposed, but uninfected group, and higher than a US Medicaid-eligible population. 14 The health and well-being of youth with HIV infection are likely monitored more regularly and/or more closely compared with their HIV exposed, but uninfected counterparts, leading to greater opportunity for diagnosis and referral to treatment. 8
Diagnoses and treatment of MH problems are a national concern for all youth, especially those with a chronic health complication. For those families affected by HIV, diagnosis and treatment are critical steps to ensuring optimal physical and MH, successful ARV medication adherence, and prevention of HIV transmission for youth with PHIV, as well as secondary quality of life outcomes such as educational achievement, vocation acquisition, and positive social relationships. Knowledge of the disparities between prevalence of symptoms and diagnoses, and their treatment, as well as their associated predictors may help target those youth who experience barriers to mental healthcare and support better access to services. The purpose of this investigation was to examine the prevalence of MH symptoms, diagnoses, and MH treatment utilization among a large US cohort of youth affected by HIV, and to identify factors, including ARV and HIV exposures, associated with those outcomes.
Methods
Study participants
Youth included in these analyses were 10–22 years of age and enrolled in the Adolescent Master Protocol (AMP) of the Pediatric HIV/AIDS Cohort Study (PHACS), a longitudinal study of the effects of perinatal HIV and ARV therapy on youth living with PHIV and PHEU. There are 15 urban sites across the United States, including Puerto Rico. All youth enrolled in AMP were perinatally HIV exposed, 7 to <16 years of age at enrollment (during 2007–2009), and with documented history of ARV exposure.
Procedures
Institutional Review Boards (IRB) at all participating sites and the Harvard T. H. Chan School of Public Health approved the study; written informed consent was obtained for adult (caregiver) and youth participation, and assent or consent was obtained from age-appropriate youth according to local IRB guidelines. Caregivers' enrollment was requested, but not required.
AMP study visits occurred every 6 months post-enrollment, and then annually after 2010. Data collection was staggered across PHACS visits to decrease burden at each visit and included information from medical examination, medical chart review, structured demographic and psychosocial interviews, and neurodevelopmental evaluations. All PHACS measures for this analysis were administered by centrally trained psychologists (for psychometric assessments) or staff in English or Spanish (for those measures available in Spanish and when site psychologist was fluent in Spanish) at the time points indicated for each measure below.
Outcome measures
MH diagnoses
Information related to MH diagnoses was collected by medical record review/abstraction and caregiver interview. MH diagnoses from the participant's medical records were provided on the Diagnosis Report (DR), a modified record developed by the Adult AIDS Clinical Trials Groups and adapted by the Pediatric AIDS Clinical Trials Group (PACTG), to record medical and MH diagnoses, including name of diagnosis, dates of onset and resolution, and number of days hospitalized due to the diagnosis. Only diagnoses that could be verified with source documentation were recorded.
The Neuropsychological Diagnoses (NPD) interview, developed by PHACS investigators, was designed to collect information on all current MH diagnoses and treatments, including those that could not be recorded on the DR form due to inadequate source documentation. The NPD interview provides a record of primary caregiver responses during a confidential evaluation with the site psychologists. This interview was administered to older youth at the psychologists' discretion if a caregiver did not attend the study visit. Information collection with the NPD interview began in February of 2011 and includes the following: MH diagnosis, date of diagnosis, diagnosing clinician, relevant medications prescribed, and other types of treatments. Verification by a source document was attempted with caregiver consent, but not required. The DR used for this analysis was completed at every AMP study visit; the NPD interview was completed at the 2-, 2.5-, 3-, 4-, 5-, 6-, and 7-year post-enrollment study visits after February 2011.
MH diagnoses were classified as follows: (1) behavior disorder, including oppositional defiant disorder, disruptive behavior disorder, impulse control disorder, conduct disorder, and intermittent explosive disorder; (2) mood disorder, including depression, dysthymia, and bipolar disorder; (3) anxiety disorder, including generalized anxiety disorder, social anxiety, selective mutism, and panic disorder; (4) trauma disorder, including post-traumatic stress disorder and adjustment syndrome; (5) pervasive developmental disorder, including autism and Asperger's disorder; (6) ADHD; and (7) other disorders, including obsessive compulsive disorder, psychosis, personality disorder, eating disorder, and substance use disorder.
Emotional/behavioral functioning
The Behavior Assessment System for Children, Second Edition (BASC-2), 31 is a psychometrically reliable tool used to assess emotional and behavioral functioning of youth, and is available in both English and Spanish. 32 The youth and caregiver versions were collected using the BASC-2 Self-Report of Personality form and the Parent Rating Scale, respectively. Normalized scores are reported as T-scores, with higher scores indicating more problems. “Clinically significant” scores (T-score ≥70) represent highly maladaptive behavior and correspond to scores two standard deviations above the mean.
Youth-reported symptom indices included Internalizing Problems Composite and Inattention/Hyperactivity Composite. Parent-reported symptoms included Internalizing Problems, comprising scales measuring anxiety, depression, and somatization, and Externalizing Problems, comprising scales measuring hyperactivity, aggression, and conduct problems. A clinically significant BASC emotional/behavioral problem was defined as a T-score of ≥70 on any of those four youth- and/or parent-reported domains. The BASC-2 was completed at entry and 2-, 2.5-, 4-, and 6-year post-enrollment study visits.
Measurement of covariates
Youth factors
Demographic and health information were collected from the visit at or closest to the most recent NPD form, or from the visit at which an MH diagnosis was reported. Included in the analysis for all participants were the following: age at NPD evaluation (pre-adolescence: 10–13 years; adolescence: 14–17 years; and young adult: 18–22 years), demographics (sex, ethnicity, race, and primary language), full scale intelligence quotient (FSIQ) from the age-appropriate Wechsler Scales of Intelligence, 33 number of changes in caregiver, type of caregiver (biologic parent, other relative, and nonrelative), HIV status, history of any substance use (alcohol, marijuana, and cigarettes), number of stressful life events, and number of negative life events.
Stressful life events were measured by the Quality of Life Assessment, a tool modified from the General Health Assessment for Children interview by the PACTG. 34 Negative life events were defined as stressful life events from the Life Events Checklist that the child or caregiver rated as “bad” with regard to its effect on him/her. 35
HIV control
Covariates of interest for analyses restricted to PHIV participants included knowledge of HIV status, disease severity [peak and most recent HIV RNA viral load (VL), nadir and most recent absolute CD4 count and percent, and prior CDC AIDS diagnosis] 36 and HIV-related encephalopathy, age at peak VL, most recent ARV regimen [classified as combination antiretroviral therapy (cART) with protease inhibitor (PI) vs. cART without PI vs. non-cART vs. not on ARVs], and age at cART initiation.
Primary caregiver factors
Demographic information, including family income, education, marital status, and living arrangement (living with vs. not living with partner/spouse), was collected at the visit with the most recent DR or NPD interview or the most recent MH diagnosis. Functional health limitations were measured using a study-specific questionnaire of the impact of health-related symptoms on everyday functioning. Cognitive functioning was assessed with the Wechsler Abbreviated Intelligence Scale, 37 a brief, psychometric sound measure of cognition for 6- to 89-year-olds, which provides an FSIQ.
Maternal psychiatric and substance use disorders were assessed using the Client Diagnostic Questionnaire, 38 a validated psychiatric screening tool developed for adults with HIV, and based on the PRIME-MD, 39 a well-validated screening instrument for primary care, using Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria. Diagnoses include major depressive disorder, mood disorder not otherwise specified (NOS), generalized anxiety, panic, post-traumatic stress disorder, substance abuse disorder, and psychosis NOS, with questions on psychiatric treatment history. Summary scores with excellent sensitivity and specificity include any psychiatric disorder, any substance use disorder, and any disorder (including both psychiatric and substance use disorders).
Statistical methods
The distributions of covariates by HIV infection status were summarized. The prevalence of current and ever MH disorders reported during the NPD interview and/or recorded on DRs by medical record review was compared between PHIV and PHEU participants and among age groups (10–13 vs. 14–17 vs. ≥18 years). The prevalence and type of MH treatment utilization were summarized by HIV status and age among the overall population, as well as among participants who had a current MH disorder. Diagnosis provider/clinician was summarized for participants who ever reported an MH disorder during the NPD interview. We also compared the prevalence of current MH disorders and treatment utilizations among participants with and without clinically significant BASC emotional/behavioral symptom, separately. Two-sample t-tests, chi-square tests, and Fisher's exact tests were used, as appropriate, for statistical comparisons.
Separate logistic regression models were used to evaluate the associations of the covariates with the presence of current MH diagnoses and with treatment utilization. Univariable analyses were first conducted to evaluate the association between each individual covariate and outcome. All covariates with p-value <0.1 from the univariable models were then retained in the final multivariable model, to estimate the adjusted associations between the covariates and the outcomes. Only disorders with a prevalence of ≥10% were included in the multivariable analyses. Unadjusted and adjusted odds ratios, 95% confidence intervals, and p-values were obtained from the regression models. Those analyses were conducted, separately, for the overall population, and for the youth with PHIV. Missing indicators were created for covariates with >5% missing data. Statistical significance was defined as a two-sided p-value <0.05. SAS 9.4 (SAS Institute, Inc., Cary, NC) was used for all analyses.
Results
Study population
As of October 2014, 569 AMP youth were considered eligible to be included in these analyses; 11 (2%) who had not completed the scheduled neuropsychological evaluation were excluded. Of the remaining 558 enrollees, 551 had completed DRs and NPD interviews, and 502 had NPD interviews and DRs completed at the same visit as the most recent BASC-2 evaluation. One BASC-2 was considered invalid based on validity indices; 501 were included in analyses involving the BASC-2. Reasons for the 11 missing NPD forms included caregiver refusal, caregiver not available, and problems with form access.
Table 1 summarizes youth, family, and health characteristics of the study cohort, stratified by HIV infection status. Ninety-three youth were in the 10- to 13-year age range, 249 were in the 14- to 17-year age range, and 209 were between 18 and 22 years of age. Of the 355 (64%) youth with PHIV and 196 (36%) who were PHEU, the majority were black (68%), 29% were Hispanic, and 52% were female. Table 2 summarizes characteristics of youth with PHIV, 34% had a detectable VL (HIV RNA >400 copies/mL), 26% had CD4% ≤ 25%, 26% had a CDC classification C, and 94% knew their HIV status.
Distributions of Background Characteristics At or Before the Most Recent Neuropsychological Evaluation by HIV Infection Status
The last available data at or before the most recent neuropsychological evaluation were used regardless of time interval for the following: child primary language, Tanner stage, child full scale IQ, primary caregiver identity, number of changes in caregivers, number of people living in household, household annual income, caregiver education, caregiver marital status, caregiver living arrangement, and caregiver number of functional limitations.
Caregiver psychiatric or substance use disorders were defined as EVER disorder by the time of the most recent neuropsychological evaluation.
Data measured at the time of the most recent neuropsychological evaluation or up to 1 year prior were used for the following: youth-reported substance use.
Data measured at the time of the most recent neuropsychological evaluation or up to 2 years prior were used for the following: caregiver/youth-reported stressful life events (caregiver reports were used for <12 years of age and youth reports were used for ≥12 years of age) and youth-reported life event checklist.
Variables with limited data are as follows: youth-reported substance use at 10 years of age or older; youth-reported stressful life events at 12 years of age or older; and youth-reported life event checklist at 8–15 years of age.
Covariates with >5% missing data are as follows: any substance use (n = 38, 7%), caregiver FSIQ (n = 157, 28%), caregiver ever MH disorder (n = 65, 12%), caregiver ever substance use disorder (n = 60, 11%), caregiver ever received treatment for psychiatric problems (n = 52, 9%), and number of illicit drugs caregiver used in life time (n = 59, 11%).
Variables considered, but not significantly different between HIV groups, and not shown in table include mean age at most recent neuropsychological evaluation, Tanner stage, number of changes in caregiver, number of people living in household, number of people living with partner/spouse, and number of caregiver functional limitations.
t-Test with equal variance for continuous variables; chi-square test for categorical variables.
FSIQ, full scale intelligence quotient; MH, mental health.
Associations with p values
Distributions of Background Characteristics At or Before the Most Recent Neuropsychological Evaluation for Perinatally HIV-Infected Youth (N = 355)
The last available data at or before the most recent neuropsychological evaluation were used regardless of time interval for the following: CDC classification and HIV-related encephalopathy.
Data measured at the time of the most recent neuropsychological evaluation or up to 1 year prior were used for the following: the most recent CD4 and RNA and the most recent ARV regimen.
ARV, antiretroviral; cART, combination antiretroviral therapy.
The PHIV and PHEU groups varied on a number of youth characteristics, including age, race, ethnicity, primary language, use of alcohol, marijuana, or cigarettes, number of negative life events, and relationship to caregiver. Differences were also observed in caregiver and psychosocial factors, including household income, caregiver marital status, presence of caregiver MH problems, caregiver substance use, and caregiver MH treatment.
Prevalence of MH diagnoses
Prevalence of any current or previous (ever) MH diagnoses did not differ by HIV infection status. Thirty-two percent of the entire cohort had a current diagnosis (Fig. 1); 36% had a current or prior diagnosis. ADHD was the most prevalent current disorder among all ages, and did not differ significantly by age group, although the youngest group experienced the greatest prevalence (28% vs. 25% vs. 19%; p = 0.16). Current mood disorder was reported among 10% of participants and was most prevalent in the young adult group compared to the adolescent and preadolescent groups (16% vs. 9% vs. 1%, p < 0.001). Current behavior disorders were more prevalent among adolescents than among younger or older age groups (6% vs. 4% vs. 1%, p = 0.03), while anxiety disorder was marginally more prevalent among young adults (7%; p = 0.06) than others. Trauma disorder, including post-traumatic stress disorder and adjustment disorder, was diagnosed in 1% of the younger age groups and in 3% of the young adult group (p = 0.44). Twelve percent of the young adult group and 9% of younger age groups reported more than one MH diagnosis (p = 0.83). The prevalence of MH comorbidity did not differ by HIV status.
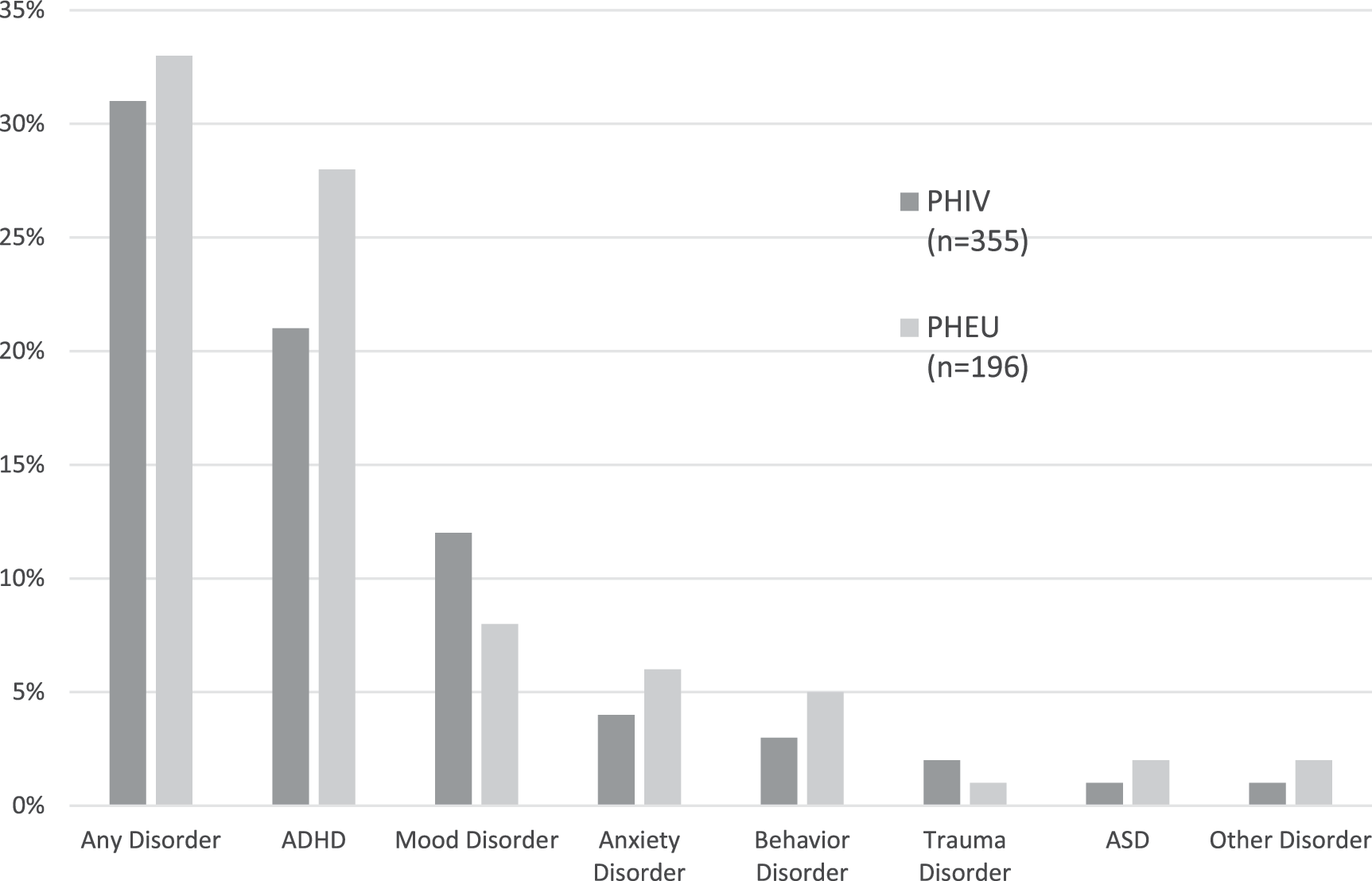
Prevalence of current MH diagnoses at most recent visit. p Values for all comparisons are >0.05. MH, mental health; PHEU, perinatally HIV exposed, but uninfected; PHIV, perinatally HIV-infected.
Overall, MH problems were typically diagnosed by a psychiatrist (54%) or by a psychologist (29%). PHEU youth were more likely than youth with PHIV to receive diagnoses from a pediatrician (30% vs. 17%). Psychiatric nurses were also a source of diagnostic services, more commonly in youth with PHIV than PHEU (11% vs. 3%).
Prevalence of serious emotional/behavior symptoms
Overall, 15% of youth with parent or self-report BASC-2 evaluations had a clinically significant (T ≥ 70) score in at least one domain of functioning; this did not differ by HIV status. Of those, 39% did not have a concurrent MH diagnosis reported on the DR or NPD interview. Of those with a clinically significant BASC-2 score, 44% had a current diagnosis of ADHD, 24% with mood disorder, 15% with behavioral disorder, and 11% with anxiety disorder. Types of diagnoses for those with a clinically significant BASC-2 score did not differ by HIV status or age group.
Prevalence of treatment utilization
Figure 2 summarizes the prevalence of MH treatment among the entire cohort, and among those with an MH diagnosis. Twenty-three percent of the entire cohort was engaged in MH treatment at the time of the most recent evaluation. Among youth with PHIV and a current diagnosis (n = 109), 67% received treatment versus 51% of PHEU youth (n = 65; p = 0.04). For both PHIV and PHEU groups, combination treatment, including therapy/counseling plus medication, was the most common treatment option (31% and 28%, respectively), and therapy alone was least common for both groups (15% and 9%, respectively). Youth with PHIV utilized each treatment category (therapy only, medication only, and therapy and medication) at a higher prevalence than the PHEU group, although differences were not significant (p = 0.18). The prevalence of treatment was similar among all age groups (pre-adolescents = 62%; adolescents = 65%; and young adults = 56%); prevalence of different treatment options did not differ by age group.

Prevalence of current MH treatment in total cohort and among those with a diagnosis. p Values for all comparisons are >0.05. Dx, diagnosis; MH, mental health; PHEU, perinatally HIV exposed, but uninfected; PHIV, perinatally HIV-infected.
Among youth with a clinically significant BASC-2 score, 51% received treatment. Type of treatment varied by HIV status (p = 0.02); youth with PHIV were more likely than PHEU youth to receive therapy only (19% vs. 0%) or medication only (10% vs. 4%), and less likely to receive both (23% vs. 44%). In addition, 19% of youth whose BASC-2 scores were within normal limits were also receiving treatment (PHIV = 22%; PHEU = 15%; p = 0.10).
Factors associated with current MH diagnosis
In the analysis exploring the associations of covariates and current MH diagnosis, only mood/anxiety (combined categories) and ADHD disorders were considered due to low prevalence of other disorders. In multivariable models, among the entire AMP sample (Table 3), mood/anxiety disorders were associated with older age, caregiver with previous or current MH disorder, and four or more stressful life events, as reported by youth and/or caregiver. ADHD was associated with younger age, male sex, caregiver with previous or current MH disorder, caregiver- or youth-reported stressful life event, caregiver FSIQ ≥85, PHEU status, and caregiver who is a nonbiological parent.
Adjusted Associations of Covariates with Mental Health (MH) Disorders Reported on Neuropsychological and General Diagnoses Reports Among All Adolescent Master Protocol Participants (N = 551)
Adjusted OR of MH disorder for participant with a specific characteristic compared to the reference group. Final multivariable model included covariates with p < 0.1 in the univariable analysis. Missing indicators were created for covariates with >5% missing data (child any substance use, caregiver FSIQ, and caregiver previous or current MH and substance use disorder).
ADHD, attention-deficit hyperactivity disorder; CI, confidence interval; FSIQ, full scale intelligence quotient; MH, mental health; OR, odds ratio.
Associations with p values
Among youth with PHIV (Table 4), higher risk of mood/anxiety disorders was associated with older age, caregiver with previous or current MH disorder, and living with a caregiver who was married (vs. single, never married). Higher risk of ADHD diagnoses was associated with not being aware of one's HIV status, and having a nonbiological parent as caregiver.
Adjusted Associations of Covariates with Mental Health (MH) Disorders Reported on Neuropsychological and General Diagnoses Reports Among HIV-Infected Participants (N = 355)
Adjusted OR of MH disorder for participant with a specific characteristic compared to the reference group. Final multivariable model includes covariates with p < 0.1 in the univariable analysis. Missing indicators were created for covariates with >5% missing data (including child any substance use, caregiver FSIQ, and caregiver previous or current MH and substance use disorder).
ADHD, attention-deficit hyperactivity disorder; CI, confidence interval; FSIQ, full scale intelligence quotient; MH, mental health; OR, odds ratio.
Associations with p values
Factors associated with current MH treatment
Among all participants, regardless of report of an MH diagnosis, utilization of treatment was associated with caregiver FSIQ ≥85, caregiver with a previous or current MH disorder, and nonbiological parent as caregiver (Fig. 3). Among all youth with MH diagnoses, MH treatment was associated with annual household income greater than $40,000. Among youth with PHIV, regardless of presence of an MH diagnosis, MH treatment was associated with starting cART therapy at a younger age, caregiver FSIQ ≥85, caregiver with a previous or current MH disorder, and four or more stressful life events. Among youth with PHIV and an MH diagnosis, caregiver relationship status (living with spouse/partner) was associated with treatment utilization.

Adjusted associations of covariates with treatment utilization, by HIV status and MH diagnosis. Multivariable regression models were built separately for each group. Reference categories are as follows: HIV exposed, but uninfected, no stressful life event, per 1-year increase in age at initiating cART, CD4% <15%, household income <$20K, bioparent not primary caregiver, caregiver education >high school, caregiver FSIQ ≥85, no caregiver MH disorder, caregiver not living with spouse, and no drug use by caregiver. Other nonsignificant covariates that were not shown in plot are as follows: ethnicity, child language, caregiver marital status, and research site. cART, combination antiretroviral therapy; FSIQ, full scale intelligence quotient; MH, mental health.
Discussion
In one of the largest cohort studies of PHIV-affected youth from varied regions in the United States, the prevalence of MH diagnoses was greater than expected relative to the general population, 23,24 yet lower than earlier reports of MH diagnoses in cohorts of youth affected by HIV, including both PHIV and PHEU youth. 6,8,13 Overall, PHIV and PHEU youth, 10–22 years of age, had a comparable prevalence of MH diagnoses, although variability was observed in prevalence and correlates of specific disorders.
Differences in methodology may account, in part, for a lower reported prevalence of disorders (e.g., direct diagnostic assessment vs. interview/chart abstraction), but a number of other possibilities exist, such as the increased effectiveness of current ARV medication, which can mitigate neurotoxic effects of HIV and ultimately MH functioning. It is also possible that long-term enrollment in this longitudinal study heightened sensitivity to MH risk among these youth and/or provided preventive services that alleviated need for MH services, including better access to consistent care and medications.
The prevalence of serious emotional/behavioral symptoms, as reported by parents or youth in each group of HIV-affected children and adolescents, was similar. Despite youth/caregiver reports of significant emotional/behavioral issues, however, more than a third of symptomatic youth did not have an MH diagnosis, regardless of HIV status. Although this may represent youth whose caregivers deemed that symptoms did not warrant consultation with an MH professional, or had reduced motivation for or access to MH services, 40 it is also possible that services were accessed, but diagnostic criteria were not met.
Our findings indicate an unmet need for MH services for some youth, yet utilization of MH services in this cohort was higher than utilization data from other national survey studies with demographically similar, but non-HIV-affected populations. 24 –27 Among the entire cohort, with and without an MH diagnosis, youth with PHIV were more likely than PHEU youth to receive MH services; among those with an MH diagnosis, two-thirds of youth with PHIV received treatment compared to half of those PHEU youth.
Among youth with serious emotional/behavioral symptoms, half were receiving treatment. Extant literature suggests low-income and ethnic minority adolescents with MH disorders utilize MH services far less than what was identified in this cohort. 24 –27 Given the added stigma of HIV, one could surmise that HIV-affected youth might utilize services at an even lower rate. However, this study corroborates findings from previous studies demonstrating that youth with PHIV are more likely to utilize MH treatment of any kind, in the presence of accessible services. 13,14 It is likely that the higher prevalence of treatment among youth with PHIV is related to their consistent connection with medical services related to HIV care and the high level of multidisciplinary comprehensive service systems that typically provide care to PHIV children and adolescents. These systems, often funded by Ryan White and other government programs, typically include social work and other counseling services. Also, youth with PHIV in this cohort were more likely to live with a non-HIV-infected caregiver, and were more likely to have a higher annual household income; it is possible that such factors were associated with fewer adverse life events, including factors related to caregiver illness, and/or easier access to supportive resources.
Consistent with some previous studies, risk for MH disorders was not primarily related to HIV infection status, 9,10,13 as evidenced by the similar prevalence of MH problems in both cohorts in this study. Contrary to previous studies implicating early disease progression as a marker of risk for later impairment, including MH problems, 41 having a CDC AIDS diagnosis was not associated with higher risk of MH problems in this study. Similarly, CD4 count and HIV RNA concentration, the blood biomarkers that may reveal current or earlier immune compromise, were not associated with MH outcomes. The majority of youth with PHIV enrolled in AMP were under adequate virologic and immunologic control, which may attenuate the effect of immune compromise or viral replication on risk for MH disorders. We also found no association between exposure to any category of ARV treatment and risk for an MH disorder.
Instead, risk of having an MH diagnosis was related to a number of individual, family, and contextual factors, as has been observed in earlier studies. 10,42 Similar to previous findings, stressful life events were associated with the prevalence of an MH diagnosis in this population. 5,26,43 Youth affected by HIV may be at increased risk for exposure to serious or frequent stressful life events, which may contribute to a cycle of increased stress hormones and fatigue, with a direct or indirect influence on MH symptoms. 44,45
Caregiver health and family resources, particularly caregiver MH, were related to youth MH outcomes. This relationship is likely complex and inter-related, with influences from genetic as well as parenting processes. MH disorders, including depression and post-traumatic stress disorder, are highly prevalent among mothers with HIV, 2,8,46 and may be associated with an increased risk for poor child outcomes. 41 A caregiver with HIV and concomitant MH difficulties may also be challenged by health-related physical complications and may experience ongoing or intermittent limitations in ability to monitor and/or optimally participate in children's daily activities and/or prevention/intervention services.
Other family-related findings were not as intuitive. An association between having a married caregiver and higher risk for a mood or anxiety disorder among those with PHIV is not as clearly interpretable, but may reflect a more stable home environment, possibly with adoptive caregivers, who are more prevalent in the PHIV cohort, and a greater likelihood for utilizing diagnostic MH services. Other findings suggested that not being aware of HIV status conferred a higher risk for an ADHD diagnosis for youth with PHIV. We surmise that those with ADHD were less likely to be disclosed to, given the increased risk of a child with less than optimal self-regulation making unplanned disclosures to others.
Age and gender played a role in the prevalence of specific types of diagnoses, as is seen in the general population and in other studies examining MH in the PHIV population. 9,13 PHEU youth and males were at higher risk for ADHD. There was also a trend of a higher prevalence of ADHD in the younger age groups, while the adolescent age group had a significantly higher prevalence of behavior disorders compared to their older and younger peers. The young adults were at greatest risk for mood and anxiety disorders. This is typically the age range in which mood and/or anxiety disorders become prevalent. Older youth/young adults are transitioning to more independent functioning with greater responsibility for employment, continuing education, housing, and maintenance of important peer/social relationships, sometimes with inadequate support. The development of MH problems may also reflect the presence of stressful life events experience by older youth, such as disclosure of HIV status to intimate partners or exposure to HIV-related stigma within social situations or relationships, which may result in MH complications. Although there was a relatively low prevalence of trauma disorders reported, there was a slight increase of these disorders for youth 18 years of age and older. Given the complicated interactions between neurobiological changes and a sometimes stressful adolescent/young adult environment, it is important to recognize the dynamic nature of the risk for psychopathology during these developmental stages. 47
This study has many strengths, including a large national cohort, prospective data collection, inclusion of an appropriate comparison group, and inclusion of data on emotional and behavioral symptoms, as well as MH diagnoses. There are also limitations. Diagnoses were obtained through parent interview or medical record rather than by formal diagnostic assessment, allowing for reporting bias, including social desirability, poor recall, and stigma-influenced responses, as well as variability in the criteria or standards under which a diagnosis is made. Because this cohort is part of a longitudinal study in which youth were followed regularly for long periods and were not only more likely to achieve stable HIV control but also have easier access to MH services, participants may not be representative of the wider population of youth with PHIV in the United States, which may explain why the prevalence of MH disorders was lower than in earlier US cohort studies. 9,13 They may also not adequately represent youth from low-resource countries where HIV is more prevalent in the general population and ART may have been unavailable until recent years.
Nonetheless, understanding types, prevalence, and factors associated with MH diagnoses and their treatments may help inform targeted prevention and intervention efforts. At the same time, identification of serious emotional and behavioral symptoms allows us to understand youth who are experiencing MH problems, but have ambiguous or subthreshold symptoms that do not yet meet diagnostic criteria or have not yet accessed mental healthcare. 48 Early identification of these youth is critical for preventing the development of serious MH conditions, which may precipitate high-risk behaviors, including substance abuse and condomless sex leading to HIV transmission, as well as nonadherence to HIV treatment regimens and care for youth with PHIV. 49 –52
Our data support the provision of multi-level, evidence-informed prevention and interventions that appreciate the dynamic nature of adolescence and recognize both individual and family risk factors as key targets for prevention/intervention services. Although some community and structural stressors are not easily modified, they must be recognized and preempted through mental healthcare, recognition and development of individual strengths and resilience, and development of effective communication and coping skills for both youth and their caregivers.
Footnotes
Acknowledgments
We thank the children and families for their participation in PHACS, and the individuals and institutions involved in the conduct of PHACS. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development with co-funding from the National Institute on Drug Abuse, the National Institute of Allergy and Infectious Diseases, the Office of AIDS Research, the National Institute of Mental Health, the National Institute of Neurological Disorders and Stroke, the National Institute on Deafness and Other Communication Disorders, the National Heart Lung and Blood Institute, the National Institute of Dental and Craniofacial Research, and the National Institute on Alcohol Abuse and Alcoholism, through cooperative agreements with the Harvard T.H. Chan School of Public Health (HD052102) (Principal Investigator: George Seage; Project Director: Julie Alperen) and the Tulane University School of Medicine (HD052104) (Principal Investigator: Russell Van Dyke; Co-Principal Investigator: Ellen Chadwick; Project Director: Patrick Davis). Data management services were provided by Frontier Science and Technology Research Foundation (PI: Suzanne Siminski), and regulatory services and logistical support were provided by Westat, Inc. (PI: Julie Davidson). The following institutions, clinical site investigators, and staff participated in conducting PHACS AMP and AMP Up in 2016, in alphabetical order: Ann and Robert H. Lurie Children's Hospital of Chicago: Ram Yogev, Margaret Ann Sanders, Kathleen Malee, and Scott Hunter; Baylor College of Medicine: William Shearer, Mary Paul, Norma Cooper, and Lynnette Harris; Bronx Lebanon Hospital Center: Murli Purswani, Mahboobullah Mirza Baig, and Alma Villegas; Children's Diagnostic & Treatment Center: Ana Puga, Sandra Navarro, Patricia A. Garvie, and James Blood; Boston Children's Hospital: Sandra K. Burchett, Nancy Karthas, and Betsy Kammerer; Jacobi Medical Center: Andrew Wiznia, Marlene Burey, Ray Shaw, and Raphaelle Auguste; Rutgers—New Jersey Medical School: Arry Dieudonne, Linda Bettica, and Juliette Johnson; St. Christopher's Hospital for Children: Janet S. Chen, Maria Garcia Bulkley, Latreaca Ivey, and Mitzie Grant; St. Jude Children's Research Hospital: Katherine Knapp, Kim Allison, Megan Wilkins, and Jamie Russell-Bell; San Juan Hospital/Department of Pediatrics: Midnela Acevedo-Flores, Heida Rios, and Vivian Olivera; Tulane University School of Medicine: Margarita Silio, Medea Gabriel, and Patricia Sirois; University of California, San Diego: Stephen A. Spector, Kim Norris, and Sharon Nichols; University of Colorado Denver Health Sciences Center: Elizabeth McFarland, Eric Cagwin, Emily Barr, and Alisa Katai; and University of Miami: Gwendolyn Scott, Grace Alvarez, Gabriel Fernandez, and Anai Cuadra.
Compliance with Ethical Standards
Author Disclosure Statement
No competing financial interests exist.