
Abstract
This study assesses effects of a community-based intervention across seven sites in the United States on HIV care utilization and study retention, among people living with HIV (PLWH). A two-armed study was conducted from 2013 to 2016 in each of seven community-based agencies across the United States. Each site conducted interventions involving community engagement approaches in the form of case management or patient navigation. Control conditions were standard of care involving referral to HIV clinical care. Participants (N = 583) were adults reporting erratic or no HIV care in the past 6 months. Longitudinal survey data on demographics, behavioral risks, and HIV care were collected from participants at baseline, before service delivery, and at 6-month follow-up. Unadjusted and adjusted generalized linear mixed models were used to assess the intervention effects on HIV care utilization and study retention. Participants were majority black (75.5%), cisgender male (55.1%), and heterosexual (55.4%). No significant intervention effect was observed on HIV care utilization, although both groups improved significantly over time [adjusted odds ratio (AOR): 2.09, 95% confidence interval (CI): 1.30–3.37]. Intervention participants were more likely to be retained in the study (AOR: 1.50, 95% CI: 1.03–2.20). Community intervention did not affect HIV care utilization more than standard of care, but intervention participants were more likely to be retained in the study, suggesting that such approaches support relationship building in ways that can facilitate follow-up of socially vulnerable PLWH. More research is needed to understand how such community efforts can support better HIV care utilization in these populations.
Introduction
T
Populations at increased risk for HIV/AIDS (e.g., racial, sexual, and gender minorities) are also those with intersecting vulnerabilities (e.g., poverty, trauma, injection drug use, and stigma) that exacerbate HIV risk and delayed diagnosis, and reinforce disparities in access to HIV-related services and treatment outcomes if HIV-infection occurs. 4 –9 Poor and underrepresented minority populations are less likely to receive healthcare generally, especially in the absence of healthcare safety nets. 10,11 Community-based efforts are recommended to reach populations most vulnerable to HIV and to allow for more culturally tailored and sustainable interventions. 4 Unfortunately, most studies aimed at increasing HIV testing and engagement in care among PLWH in the United States are clinic based, 12 limiting their reach to most vulnerable populations. This KP Test and Treat initiative was developed to enable community-based agencies and programs to implement innovative approaches, capable of reaching and supporting socially vulnerable PLWH to engage in HIV care. This article offers findings from the cross-site evaluation of this initiative.
Methods
KP Test and Treat supported seven unique sites to implement and evaluate innovative approaches to community-based outreach to PLWH focused on linkage to or retention in HIV care. Sites were selected via a competitive request for proposals issued in 2012 and 2013 (see Table 1 for details on study sites and interventions). A cross-site evaluation was undertaken to assess the initiative's impact on HIV care utilization 6 months after enrollment. Evaluation data were collected from the period 2013 to 2017.
Wraparound services (e.g., mental health, substance abuse treatment, housing assistance—specific services varied by site).
CM, case management; MEI, motivational enhancement intervention; MI, motivational interviewing; MSM, men who have sex with men; RCT, randomized control trial; SMS, short messaging service (i.e., text messages)–phones were not provided to participants.
Study design
Each site conducted a two-armed study comparing intervention and comparison groups, either with a randomized control trial or a quasiexperimental design (Table 1). Control conditions also varied by site (i.e., attention control, wait-list control, or standard of care control). All participants were assessed via surveys at baseline and 6-month follow-up, administered by their local evaluation teams.
Recruitment and sample
All seven sites served specific priority populations disproportionately affected by HIV/AIDS, including black and Latino/a men and women, transgender women, men who have sex with men, people coming out of incarceration, and substance using populations. Sites were based in major metropolitan areas on the east and west coasts, the suburban mid-Atlantic, and the rural southeast (Table 1). Sites recruited (1) HIV-negative adults (aged 18+ years) within their target population for HIV testing, and/or (2) PLWH who were not currently in care (i.e., newly diagnosed and never linked), or tenuously engaged in HIV care (i.e., inconsistent use of care across the past year or no antiretroviral therapy (ART) use in the past 6 months).
Intervention
For this initiative, interventions at each site were community based and delivered via trained peers or community members serving as case managers 13 –16 or patient navigators 17,18 ; these interventionists elicited information regarding clients' social and healthcare needs and offered personalized approaches to help clients connect to services to meet these needs (Table 1). Interventions all included one-on-one sessions delivered via direct face-to-face contact, although the rural site did use short message service (SMS) messaging for follow-up. 19 Structural supports (e.g., transportation and food security) were also provided due to high social needs of populations served. 20 As all interventions used a community-based strategy and personalized connection to link participants to healthcare, we aggregated data across sites to assess effects of the initiative as a whole, relative to their control groups.
There was some variation by site in intervention approaches as well as population of focus. Group interventions, in addition to one-on-one sessions, were included in interventions for women to build social support 21 ; women-focused programs also reported assessment and linkage to services for trauma from violence. One site also used groups for nutrition education. 20 Theoretical underpinnings of approaches also varied and included strength-based case management, traditional case management (assessment and referral for service needs), 15,16 patient navigation, 12,17,18 motivational interviewing/motivational enhancement, 13,14,16,21 –24 and psychoeducational counseling. 25 Number of sessions and intervention duration also varied by site. Hence, although sample sizes were small within each site, exploratory analyses were used to examine intervention effects by site.
Procedure
On enrollment, participants (N = 583) were consented and completed a baseline survey administered by a trained agency or external evaluation staff. Surveys were conducted privately and completed on paper or using mobile tablets, as per agency preference. Participants were then allocated to either an agency-specific intervention designed to support engagement in HIV clinical care or the agencies' comparison group as per each site's evaluation design (Table 1). Six-month surveys were also conducted by agency or evaluation staff. Remuneration for study participation varied from $10 to $25, reflecting each agency's goal to be responsive to their clients' needs and maintain an established rapport with their respective communities. All study procedures were approved by the local institutional review boards of each site and/or the University of California, San Diego. This study was registered with
Measures
Sociodemographic items included age (continuous), race (white, black, Hispanic/Latino, and other), sexual orientation (heterosexual, lesbian/gay/queer, and bisexual), and gender identity (cisgender man, cisgender woman, and transgender woman [male-to-female]).
Our primary outcome was HIV care utilization, which relied on self-report due to the nonclinical nature of the initiative. We limited our outcome to reports of CD4 testing to ensure the care appointment recalled focused on HIV care; with a focus on HIV care utilization in the past 6 months, measured at both baseline and 6-month follow-up. To further explore change in the primary outcome over time, a variable henceforth referred to as “Engagement in Care” was created, with four categories:
No engagement (having no HIV care appointment in the past 6 months at baseline or follow-up), Loss to care (having an HIV care appointment in the past 6 months at baseline but no follow-up), (Re)engagement in care (having no appointment at baseline but one at follow-up), and Continuous care (having an appointment at both time points).
The HIV care variables were developed based on the Centers for Disease Control and Prevention's (CDC's) definition of HIV medical care (receipt of ≥1 CD4 or viral load tests) and continuous care (≥2 CD4 or viral load tests performed at least 3 months apart). 26 The latter variable was modified for this study to a 6-month time frame due to the timing of survey data collection used in this study.
Our secondary outcome was study retention, which was based on whether or not the participant was reached and participated at 6-month follow-up. This secondary outcome is a proxy for whether or not the intervention facilitated better agency engagement with socially vulnerable PLWH.
Covariates included study site (agency), time since HIV diagnosis (dichotomized as <12 months or ≥12 months), history of incarceration (never, in the past 12 months, or yes, but not in the past 12 months), being medically insured (yes, no), and homelessness (defined as spending at least 1 day on the streets or in a housing shelter in the past 90 days). We also included history of sexual abuse and substance use based on baseline analyses from this study, indicating the importance of these on HIV care utilization. 27 Lifetime sexual violence was defined as ever “having been forced or pressured for sex” or having someone “physically hurting the sexual parts of your body, including touching that made you feel uncomfortable.” To measure drug and alcohol-related risk behaviors, the TCU-DS2 28 and an adapted version of the AUDIT-10 (items 1–3, 9–10) 29 were used, respectively. These behaviors were defined as any self-reported illicit drug use (excluding marijuana) in the past 30 days or binge drinking in the past 30 days (≥5 drinks in one setting; adapted from AUDIT-10 item 3).
Statistical analyses
As noted above, data were aggregated across sites, by intervention and control conditions. Descriptive statistics, Pearson's chi-square tests, and independent samples Student's t-tests were used to compare participants across demographic characteristics and outcomes by group assignment, site, and retention in study. Unadjusted and adjusted generalized linear mixed model (GLMM) longitudinal logistic regression was used to assess the intervention effect over time on HIV care utilization (primary outcome), with a random subject effect to account for within-subject correlations. Adjusted models included the above-noted covariates. This “difference-in-differences” analysis amounts to testing for a statistical interaction between time and intervention group in the longitudinal model. These findings (for effect on HIV care utilization) are presented as an adjusted ratio of odds ratios (AROR). Follow-up data were available for n = 397 individuals, but n = 15 were excluded due to missing values on covariates (n = 15), resulting in an analytic sample of n = 382.
Retention in study (secondary outcome) differences between intervention and control groups were evaluated using Wald tests of unadjusted and adjusted GLMMs. The adjusted models for all outcomes included a random effect for site and a fixed effect for time since diagnosis. All other covariates were considered for inclusion via backward stepwise model building and removed at the p > 0.15 threshold level. These analyses excluded n = 7 for whom there was insufficient time to collect 6-month follow-up data and n = 17 with missing values on covariates, resulting in a subsample of n = 559 for analyses.
Given the variation by site, we also conducted unadjusted analyses by site for the primary and secondary outcomes, using the approaches previously described. Unadjusted models were used due to small site-specific sample sizes. Descriptive analyses on engagement in care were also conducted for the subsample with follow-up data (n = 397) and depicted graphically by site and treatment arm. Small cell sizes precluded significance testing.
All statistical tests were two tailed and significance was defined as p < 0.05. Analyses were conducted using SAS software, version 9.4 (Cary, NC).
Results
Among the 583 HIV-positive baseline participants, the mean age was 43.4 (standard deviation = 11.6; range = 18–78 years), and most (86.5%) had been diagnosed with HIV for a year or more (Table 2). Over half the samples were cisgender men (55.1%), approximately one-third were cisgender women (34.1%), and 10.8% were transgender women. Three-quarters of participants were black (75.5%), and 15.1% were Hispanic/Latino; 55.4% identified as heterosexual, 29.0% as lesbian/gay/queer, and 15.6% as bisexual. Nearly a third had been homeless in the past 90 days (30.4%), and 17.0% were medically uninsured. Most (69.0%) had been incarcerated in their lifetime, and a third had experienced sexual violence (33.2%). Within the past month, nearly one in five (19.0%) had used illicit drugs and 16.3% engaged in binge drinking. Intervention and control groups were not significantly different on these variables, except for binge drinking, which was more common for control relative to intervention participants (19.3% vs. 13.2%). Significant variations in these characteristics by site were seen, in part, due to different populations targeted by study site (Table 3).
Pearson's chi-square p < 0.05.
Independent samples t-tests were conducted for continuous variables, and Pearson's chi-square tests were conducted for categorical variables. Degrees of freedom (df) are indicated in parentheses.
Excluding marijuana/hashish.
SD, standard deviation.
Pearson's chi-square p < 0.01, *** p < 0.001.
Pearson's chi-square test statistics with degrees of freedom (df) is presented.
Past 30 days.
Excluding marijuana/hashish.
HIV care engagement
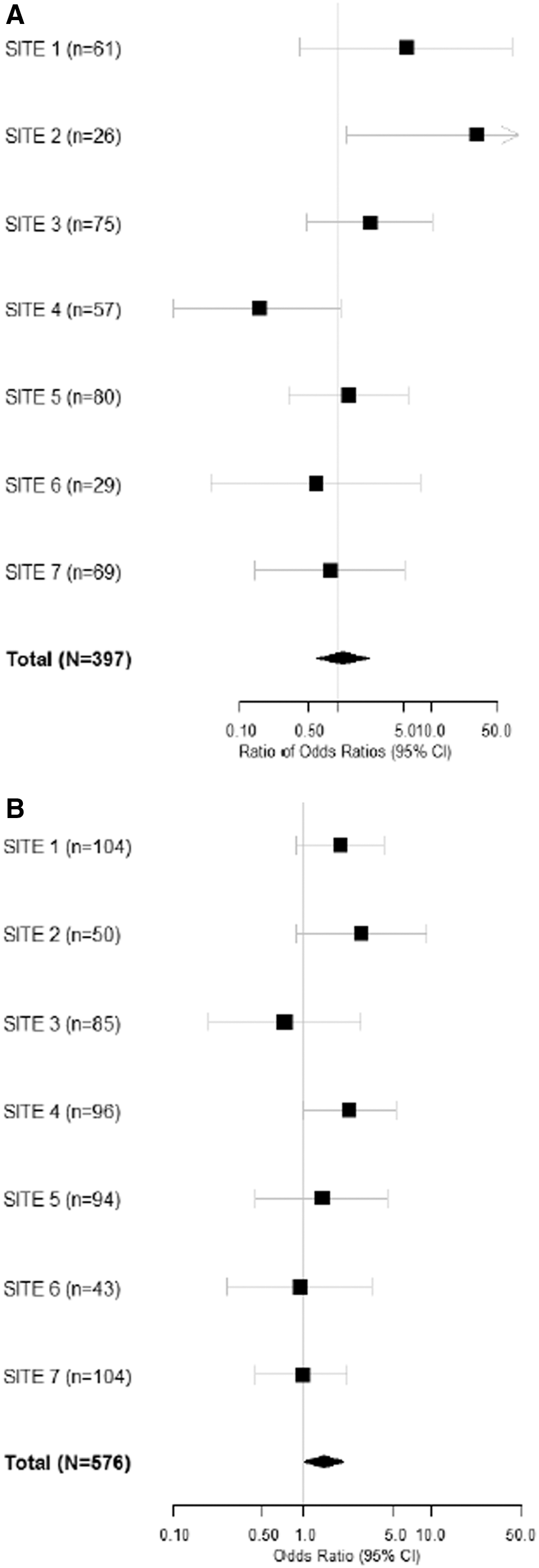
At baseline, 64.2% of participants had received HIV care in the previous 6 months, and those reporting past 6-month HIV care were significantly more likely to report that they were on ART. Difference-in-differences analyses indicate no difference between treatment groups over time on receipt of HIV care (AROR: 1.19, 95% CI: 0.61–2.32), although a significant time effect was observed across both treatment groups [adjusted odds ratio (AOR): 2.09, 95% confidence interval (CI): 1.30–3.37; Table 4]. Lifetime sexual violence and incarceration were associated with this outcome, although only the former had a clear positive relationship (AOR: 1.60, 95% CI: 1.09–2.35; Table 4). Exploratory analysis indicated that those incarcerated within the past year, relative to those previously incarcerated, had higher odds of recent HIV care (AOR: 1.77, 95% CI: 1.10–2.86), but this association did not stand up to a Bonferroni correction. Site-level variation in effect on this outcome was indicated by site-level analyses (Fig. 1A). However, subsequent exploratory analyses conducted to determine if there was heterogeneity in intervention effect on this outcome based on site differences indicated no significant heterogeneity of effect.
Unadjusted intervention effect over time on HIV care utilization
Wald p < 0.05, ** p < 0.01.
Time 2 × Time 1 analysis using Wald test of a GLMM; missing data at time 2 treated as “no”; 186 respondents removed due to no follow-up data; 15 removed due to missing values on covariates.
Time 2 analysis using Wald test of a GLMM; 7 respondents removed due to insufficient time to collect follow-up data; 17 removed due to missing values on covariates.
Study site was treated as a random effect; omitted covariates were removed during model building.
Adjusted ratio of odds ratios assessing the intervention effect over time, or “difference-in-differences analysis.”
Past 30 days.
AOR, adjusted odds ratio; CI, confidence interval; GLMM, generalized linear mixed model.
Descriptive analysis of engagement over time by site and treatment group indicated that 52.9% of the subsample with follow-up data (intervention and control groups combined) reported continuous HIV care, and an additional 26.5% were (re)engaged in care (Fig. 2). One in five either lost to care (9.8%) or not linked at all (10.8%). Site-level variation is indicated by descriptive data, but small numbers precluded significance testing for confirmation.
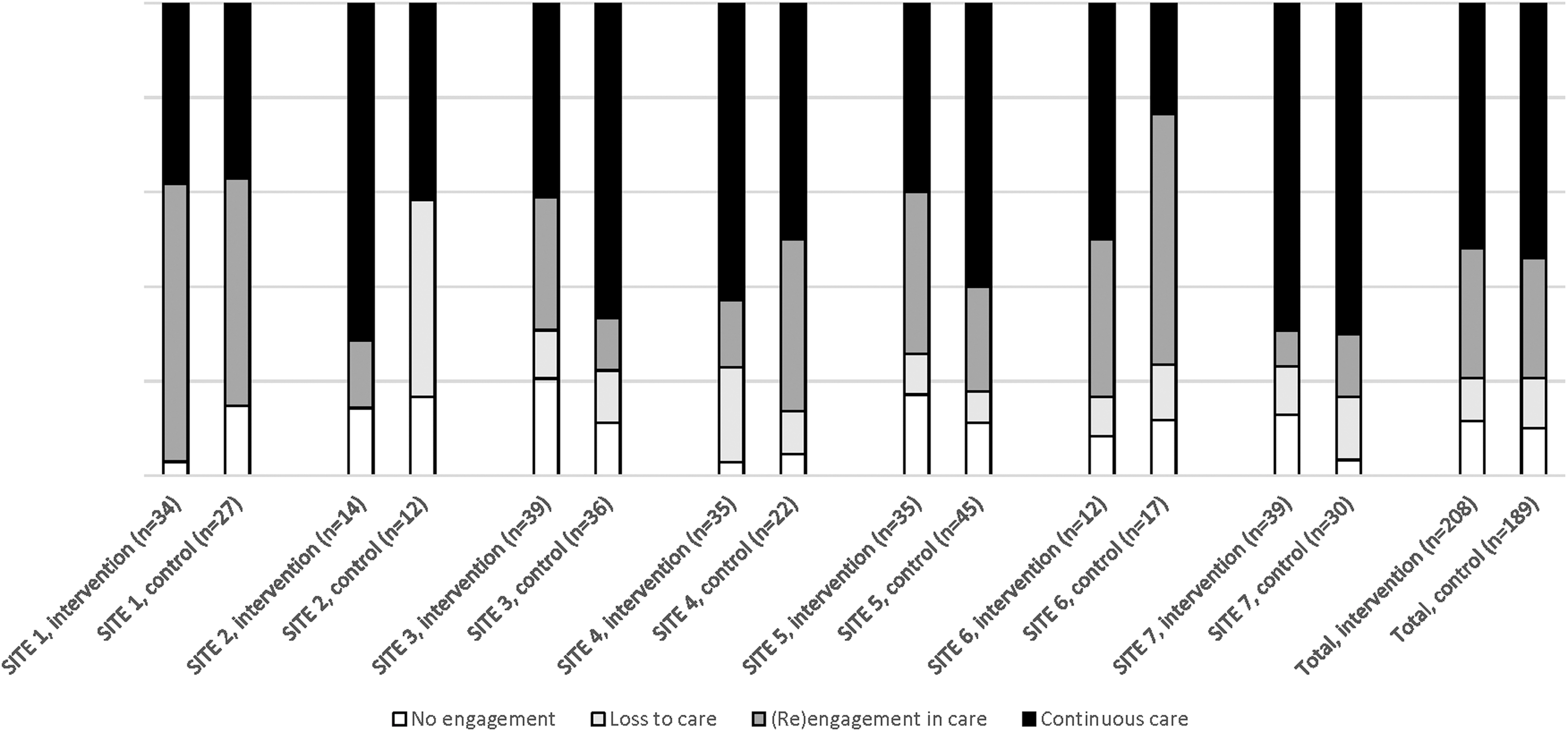
Engagement in care from baseline to 6-month follow-up, intervention and control conditions by study site (n = 397). No engagement = no HIV care reported at time 1 or time 2; loss to care = HIV care at time 1 but not time 2; (re)-engagement in care = no care at time 1 but care at time 2; and continuous care = HIV care at time 1 and time 2.
Retention in study
At 6-month follow-up, more than two-thirds of participants (68.9%, n/N = 397/576) were retained in the study. Intervention participants had higher odds of retention in study relative to those in the control group (AOR: 1.50, 95% CI: 1.03–2.20; Table 4). Bivariate analysis suggested a number of characteristics differed between those retained and those lost to study follow-up (Table 5). However, adjusted analyses indicated that participants who were older (AOR: 1.02, 95% CI: 1.003–1.04) and those who had a history of sexual violence (AOR: 1.74, 95% CI: 1.13–2.68) were more likely to be retained in the study, and those reporting past 30 days of illicit drug use were less likely to be retained in the study (AOR: 0.41, 95%: 0.21–0.79; Table 4). Site-specific intervention effects on study retention were nonsignificant, possibly due to small cell sizes (Fig. 1B). As with our primary outcome, additional exploratory analysis was undertaken to determine if there was significant heterogeneity in intervention effect on study retention, and no significant heterogeneity in effect was observed.
Chi-square p < 0.05, ** p < 0.01, *** p < 0.001.
Seven respondents removed due to insufficient time to collect follow-up data.
Continuous variable: bivariate t-test statistic. We tested for equality of variances and did not reject the null hypothesis that variances were equal; a pooled estimate for equal variances was used. Proportions: chi-square test statistics with degrees of freedom (df) is shown.
Past 30 days.
Excluding marijuana/hashish.
SD, standard deviation.
Discussion
Study findings did not demonstrate significant effects of community-based intervention—in the form of case management and/or patient navigation—on HIV care utilization among socially vulnerable PLWH. Inadequate effects on improving HIV care utilization were likely limited partly by fairly good rates of self-reported HIV care at study start. At baseline, two-thirds of participants reported past 6-month HIV care utilization. Sites showing stronger intervention effects on use of care at follow-up were those with lower reported HIV care engagement at baseline. For this population, broader health and social welfare supports, rather than an HIV care-specific focus, may be more useful. 30 While most reported recent receipt of HIV care at baseline, the proportion reporting this is smaller than that seen in national surveillance data, indicating that almost three-fourths of PLWH have received care and 57% are in continuous care. 26 These findings showcase the heightened risks faced by the populations reached via these community-based efforts. Importantly, study findings did indicate that both intervention and control participants reported an increase in HIV care utilization over time. Improvements in engagement in care overall for study participants were observed with more than half of the sample reporting continuous HIV care at follow-up (52.9%), similar to that observed at the national level, 26 with an additional 26.5% (re)engaged in care. These findings suggest that community-based sites are able to support improvements in HIV care utilization. Current standard of care, which offered supported referral and connection to social services, may provide important elements for effectiveness that should not be lost as we continue to try to improve intervention approaches to achieve CDC-recommended 90-90-90 goals. 31 Given study findings that the intervention participants were more likely than control participants to be retained in the study, the personalized engagement through case management or patient navigation may be useful to help maintain relationships with PLWH in ways that can support better follow-up.
Additional findings from this study document that participants with a history of sexual violence were more likely to report HIV care over time and more likely to be retained in the study. These findings are consistent with baseline findings from this study documenting that among PLWH, those with a history of sexual violence were more likely to get HIV care and social support services. 27 These findings run counter to those seen from the literature on intimate partner violence (IPV), demonstrating that IPV is associated with lower likelihood of HIV care, 32 as well as poorer ART adherence and viral suppression. 33 Sexual violence disclosure may differ from IPV disclosure in terms of engagement in care. More consistent with the literature are findings that recent incarceration is related to better HIV care utilization where less recent incarceration increases risk for nonutilization of care. A systematic review of the extant literature found that while engagement in HIV care may improve during periods of incarceration, these improvements decline postrelease and may even worsen relative to preincarceration engagement in care. 34 Factors identified as improving engagement in HIV care postrelease included access to resources such as transportation and stable housing. This review found that interventions that helped to address these unmet needs as well as other barriers such as limited social support, stigma, and substance use have generally helped to improve postrelease engagement in HIV care. 34 Lack of focus on these issues by the initiatives' interventions of focus may have tempered intervention effects; a fostering environment at the agency level may also have allowed for equivalent benefits to both treatment groups.
While findings suggest that community efforts may be useful in reaching and supporting HIV care utilization, 1 in 10 participants retained in the study reported no engagement in HIV care at either baseline or follow-up. These findings suggest that there are segments of the population of PLWH who may simply not wish to engage in HIV clinical care, despite maintaining connection with community organizations serving PLWH. More research is needed to understand how these populations can continue to be served by community services in the absence of clinical care utilization. Clinical care cannot be the sole outcome or necessarily even the primary purpose for these populations, if we are to support PLWH with a care-focused model rather than strictly population-based HIV prevention efforts.
Study findings should be considered in light of certain limitations, in particular reliance on self-reported measures. Ideally, medical records would be used to assess HIV care appointments. This was not possible. In addition, small sample sizes by sites limit our ability to infer causality at the level of the individual interventions. Further, dose or per protocol analyses were not possible due to differential lengths and contact data collection approaches across sites. Per protocol analyses may have yielded HIV care effects. Geographic representation of this study was limited to seven sites across six US cities, and sites targeted different populations of PLWH, affecting generalizability of study findings. Although variability existed among sites on the prevalence of HIV care utilization at each time point by group assignment, there was no statistically significant heterogeneity of intervention effect found among sites. We had low retention in the study, partly due to the vulnerable nature of the sample and the limited research support available at some sites. Notably, younger and substance using populations were more likely to be lost to study follow-up. Hence, findings may be less reflective of these groups. More research is needed to better support retention of these groups in longitudinal studies as these often include newly diagnosed individuals and those more likely to fall out of care.
In conclusion, this study finds that agencies engaging in community-based approaches to reach and retain PLWH contending with multiple forms of marginalization may offer an important complement to clinically focused retention in care programs. While the interventions undertaken by these agencies did not demonstrate greater effect on HIV care than control conditions, both treatment groups demonstrated improvements in HIV care engagement over time. Further, those involved in the interventions were more likely than control participants to be retained in the study, suggesting better relationship building through the interventions. Findings illustrate the promise of community-based organizations as a complement to clinical services to help support socially vulnerable PLWH. Such an approach should be considered part of the expansion of system-of-care factors to help PLWH achieve viral suppression, for their own health and well-being and to reduce HIV transmission. 35
Footnotes
Acknowledgments
The authors thank the community-based agencies, staff, and participants of KP Test and Treat; Action.Skills.Knowledge.4Care (ASK4Care), Duke Global Health Institute (Beth Stringfield, Sara LeGrand), Fortune Society (Nilda Ricard, Brendan O'Connell, Adrian Assing), Institute for Public Health Innovation (IPHI; Abbi Charles, Bradley Boekeloo), John Wesley Community Health (JWCH) Institute (Christopher Hucks-Ortiz, Sergio Avina, Orlando Rivera), North Jersey Community Research Initiative (NJCRI; Corey Rosmarin-DeStefano, Liliane Windsor), Public Health Institute (PHI; Mariko Iwamoto, Tooru Nemoto, Jasmine McKay), Women Organized to Respond to Life-Threatening Diseases (WORLD; Cynthia Carey-Grant, Stephanie Cornwell, Samantha Feld), as well as the Kaiser Permanente Community-Based HIV Test and Treat Study Team (Alexandra Caraballo, Pamela M. Schwartz, John Edmiston, and Melissa Ramos), without whom the study would not have been possible. They are also extremely thankful for the many hours of administrative and analytic support provided by Emma Jackson, Sankari Ayyaluru, Elizabeth Gaidry, and Sanne P. Møller. The article was also supported by NIDA K01 DA039767 to L.R.S. and K01 DA036439 to L.U. This research was supported by Kaiser Permanente and East Bay Community Foundation (Grant No. 20030041). No authors hold any financial disclosures associated with this work.
Author Disclosure Statement
No competing financial interests exist.