
Abstract
Poor retention in HIV care is associated with higher morbidity and mortality and greater risk of HIV transmission. The Patient-Centered HIV Care Model (PCHCM) integrated community-based pharmacists with medical providers. The model required sharing of patient clinical information and collaborative therapy-related action planning. The proportion of persons retained in care (≥1 medical visit in each 6-month period of a 12-month measurement period with ≥60 days between visits), pre- and post-PCHCM implementation, was modeled using log binomial regression. Factors associated with post-implementation retention were determined using multi-variable regression. Of 765 enrolled persons, the plurality were male (n = 555) and non-Hispanic black (n = 331), with a median age of 48 years (interquartile range = 38–55); 680 and 625 persons were included in the pre- and post-implementation analyses, respectively. Overall, retention improved 12.9% (60.7–68.5%, p = 0.002). The largest improvement was seen among non-Hispanic black persons, 22.6% increase (59.7–73.2%, p < 0.001). Persons who were non-Hispanic black [adjusted risk ratio (ARR) 1.27, 95% confidence interval (CI) 1.08–1.48] received one or more pharmacist–clinic developed action plan (ARR 1.51, 95% CI 1.18–1.93), had three or more pharmacist encounters (ARR 1.17, 95% CI 1.05–1.30), were more likely to be retained post-implementation. In the final multi-variable models, only race/ethnicity [non-Hispanic black (ARR 1.27, 95% CI 1.09–1.48) and “other or unknown” race/ethnicity (ARR 1.36, 95% CI 1.14–1.63)] showed an association with post-implementation retention. PCHCM demonstrated how collaborations between community-based pharmacists and primary medical providers can improve retention in HIV care. This care model may be particularly useful for non-Hispanic black persons who often are less likely to be retained in care.
Introduction
Retention in care is a critical component of the HIV care continuum. Retention facilitates access to antiretroviral therapy (ART) and receipt of prevention and adherence counseling. 1,2 Poor retention is associated with higher morbidity and mortality for the person with HIV and has significant implications for HIV transmission: an estimated 61% of new HIV transmissions originate from HIV-diagnosed persons who are not retained in care. 3 –6 Although retention confers individual-level health benefits and population-level prevention benefits, it is estimated that only 57% of people diagnosed with HIV are retained in care. 7 A more proximal determinant of morbidity and transmission risk, viral suppression, is estimated to be equally poor at 58%. 7
A lack of coordinated HIV care may contribute to poor retention and viral suppression. 8 Potentially exacerbating this problem is a dwindling HIV workforce, with a projected workforce growth that will not accommodate the increasing number of HIV-infected persons requiring care. 9 Due to these challenges, the 2020 United States' National HIV/AIDS Strategy specifically recommends an increase in the capacity of systems, as well as the number and diversity of available health care providers, for people with HIV. 10 Expanding the availability of HIV care services and fostering care integration can create additional care and treatment opportunities.
Even when people with HIV receive care from multiple health care providers, they often receive all their medicines from one pharmacy, making the pharmacist a key point of contact. Pharmacist-led interventions have led to improvement in a variety of therapeutic and adverse events outcomes for several disease states. 11 –13 Retail pharmacies are already located within communities, and when staffed with HIV and Medication Therapy Management (MTM) trained personnel, represent environments uniquely poised to initiate and continuously address HIV care and treatment problems. Community-based pharmacists in retail settings are also in key positions to collaborate with primary medical providers to improve access and efficiency of health care in the community. 14 Properly trained community-based pharmacists are poised to play an important role in improved service delivery and can reinforce the importance of retention in HIV care and adherence to medication therapy.
To determine if proactive referrals between community-based pharmacists and clinical providers can lead to improved HIV care and treatment, the Centers for Disease Control and Prevention, Walgreens Co., and the University of North Texas Health Science Center's System College of Pharmacy developed and implemented the Patient-Centered HIV Care Model (PCHCM). The goal of the project was to develop and implement a model of HIV care that integrates community-based pharmacists and clinic medical providers to provide patient-centered care for people with HIV. There were three overarching objectives of the project: (1) improve retention in HIV care, (2) improve adherence to ART, and (3) improve HIV viral suppression. This analysis evaluated retention in HIV care among the PCHCM participants.
Methods
Medication therapy management
MTM is a pharmacist-led patient-centric intervention that seeks to optimize therapeutic outcomes for individual patients. 15 MTM consists of five core components: (1) medication therapy review, (2) personal medication record, (3) medication-related action plan, (4) intervention and/or referral, and (5) documentation and follow-up.
In short, the first step of MTM is often the medication therapy review. This review is a systematic process of assessing medication regimens for indication, effectiveness, safety, and adherence. Medication therapy review may include review of response to therapy and appropriateness of each medication (e.g., proper dosing, clinical indications). The review can be comprehensive (i.e., comprehensive medication review or CMR) in which all of a patient's medications and health conditions are reviewed by the pharmacist or it can be targeted toward specific medications or medical conditions. 15
The personal medication record is a comprehensive record of each patient's current medications, compiled by the pharmacist for use by the patient. A medication-related action plan is a patient-centric document, intended for use by the patient, containing a list of actions for the patient to use in tracking progress for self-management. Intervention and/or referral occurs when the pharmacist provides consultative services and intervenes to address primarily medication-related problems. Referral to a clinic provider may occur when the patients' needs extend beyond the pharmacists' expertise or scope of practice. The final steps in the MTM consultation include documentation of services provided and a scheduling of a follow-up visit, as needed. 15
PCHCM structure
The PCHCM was a demonstration project designed to expand upon the current MTM model to be inclusive of clinical medical providers. The key differences between PCHCM and MTM are information sharing between pharmacy and clinic teams; collaborative medication-related action planning between pharmacists, medical providers, and patients; and quarterly follow-up pharmacy visits. In order for the pharmacists to conduct broader and more precise MTM, partnered clinic staff (e.g., nursing staff) compiled and provided the pharmacists with participants' medical history. This information included, but was not limited to, current and previous medical conditions, HIV viral load and CD4 test results, other laboratory test results (e.g., viral hepatitis serologies, liver function tests, serum creatinine), current and discontinued medications, drug allergies, immunizations, and social history (e.g., history of tobacco, alcohol, or illicit drug use).
Additionally, project pharmacists proactively monitored prescription refills (consistent with the HIV-specialized pharmacy program of the participating pharmacy) to ensure continuous adherence to treatment; provided individualized adherence support; and monitored medical history, including clinical and laboratory test results, to assess treatment response and identify potential therapy-related adverse events. Based on the pharmacists' assessment of clinical need, the project pharmacists then worked directly with their partnered clinic to make recommendations and discuss potential action plans and intervention strategies, for problems identified during the MTM sessions or during review of patients' medical and prescription refill histories. Pharmacists, patients, and medical providers then collaborated to implement the action plans, and progress was reviewed at subsequent project visits.
Protocol procedures
Project clinic and pharmacy staff approached patients to explain the project, its voluntary nature, and determine willingness to participate; informed consent was not required. Once patients agreed to participate, they were referred to the partnered pharmacy to schedule an initial CMR. Prior to the CMR visit, clinic staff provided pharmacists up to 2 years of participants' medical history. If the time between patient agreement to participate and the scheduled CMR appointment was short, an abbreviated medical history may have been given to the pharmacist with detailed information provided after the CMR was completed. Updated participant medical histories were provided quarterly to the pharmacists through standardized forms, and participants were scheduled for quarterly follow-up with the pharmacist. Follow-up visits were generally conducted in person, but they could also be conducted by phone. At the quarterly follow-up visit with the pharmacist, all HIV-related medications and drug therapy problems were reviewed; in addition, non-HIV-related conditions were reviewed when deemed clinically appropriate (by either the pharmacist or based on the action plan developed). More frequent pharmacist support was available as needed (e.g., participants could consult with their pharmacist monthly when picking up monthly prescription refills).
Once the CMR or follow-up pharmacy visits were completed, the pharmacist forwarded a consultation report to the clinic. For pharmacy recommendations that required clinician action (e.g., increase or decrease in medication dosage, start or discontinuation of a medication, additional laboratory tests), the pharmacist discussed the recommendation with a clinic provider, and a collaborative plan was developed to address the identified problem(s). Project pharmacists recorded all CMRs and pharmacy follow-up visits on project-specific data collection forms.
Institutional review board
The Centers for Disease Control and Prevention determined that the PCHCM constituted a public health program activity and not research. In addition, the Office of Research Compliance, on behalf of the Institutional Review Board of the University of North Texas Health Science Center determined the project met criteria for exempt status.
Project sites
Each of 10 project sites consisted of 1–2 pharmacies partnered with a medical clinic. Project sites were located in Albany, GA; Chicago, IL; Fort Lauderdale, FL; Kansas City, MO; Miami, FL; New York, NY; Palm Springs, CA; Philadelphia, PA; St. Louis, MO; and Washington, D.C. Project clinics were chosen after an initial review of the Health Resources and Services Administration's Uniform Data System and Ryan White HIV/AIDS Program Services report, to identify potential project clinics based on clinics' HIV population, and viral suppression and retention rates. Once a potential project clinic was identified, it was matched with a nearby project pharmacy.
All project pharmacies were community-based HIV-specialized retail pharmacies of a national pharmacy chain. As HIV-specialized pharmacies, all pharmacists and pharmacy technicians had previous training on HIV treatment, stigma, and cultural competency, and each pharmacy carried appropriate HIV medications and offered proactive patient care and adherence support as part of their baseline program. 16 The pharmacists received regular educational updates related to HIV/AIDS to remain current with developments in the field.
Model participation
Participants were recruited from each project clinic using a convenience sample of persons deemed eligible for participation. Eligibility criteria were as follows: aged ≥18 years at time of enrollment, on or planning to start ART, agreed to clinic visits every 6 months and to initial and quarterly MTM visits, and were willing and able to use the project pharmacies to fill their prescription medications. Additional eligibility and exclusion criteria are listed in Table 1.
Patient-Centered HIV Care Model Participant Eligibility and Exclusion Criteria
ART, antiretroviral therapy; ARV, antiretroviral; MTM, medication therapy management.
Project implementation began in a staggered manner at each site between August 2014 and September 2015. Patient follow-up ended in September 2016, which allowed for at least 1 year of follow-up for all enrolled persons. All persons who completed an initial CMR and who filled prescriptions at the project pharmacy were considered enrolled in the project at the date of the initial CMR. Each participant received at least 12 months of model services.
Definition and measurement of retention in care
Retention in care was defined as at least one medical visit with a physician, nurse practitioner, or physician assistant, in each 6-month period of a 12-month measurement period (defined in the next paragraph) with a minimum of 60 days between medical visits. 17 Medical visits were determined through clinic appointment records reported on project data collection forms.
Pre-implementation retention was measured during the 12 months leading up to and including the enrollment date, and post-implementation retention was measured from 1 day after the enrollment date to 12 months forward.
Analysis inclusion criteria
Persons were included in the analysis if they had a documented HIV diagnosis date that was ≥12 months before the enrollment date. If the HIV diagnosis date was not documented, a person was included if they had a scheduled clinic appointment at the project clinic, HIV viral load or CD4 test, or filled an antiretroviral (ARV) prescription ≥12 months before the enrollment date. A person was excluded if there were no recorded date(s) for clinic visits in the pre-implementation period.
Model intervention categories
For the purpose of the analysis, model interventions were grouped into three categories: (1) adherence support, (2) pharmacist–patient action plan, and (3) pharmacist–clinic action plan. Adherence support was defined as individualized patient adherence counseling only, without development of a pharmacist–patient or pharmacist–clinic action plan. A pharmacist–patient action plan was defined as the development of a medication-related or other action plan in collaboration with the patient for the patient's use (e.g., instructions to take medication with food to prevent nausea) and no development of a pharmacist–clinic action plan. A pharmacist–clinic action plan was defined as the development of a medication-related or other action plan in collaboration with the clinic (e.g., change medication regimen). Model interventions were counted from the date of the initial CMR and were abstracted from project pharmacy records.
Censoring
Persons were censored from the analyses at the first date that one of the following occurred: patient died, too ill (e.g., moved into hospice), moved out of area, transferred care to non-project participating clinic or provider, incarcerated, voluntarily withdrew from project, or were no longer filling prescriptions at project pharmacy. If the clinic indicated that one of the above-mentioned conditions occurred, but a date was not recorded for when the condition occurred, the person was censored 1 day after their last clinic visit. Two project sites did not collect censoring data. For these sites, it was first determined if a person had indications of being in care (i.e., person had clinic visits for any reason or had HIV viral load or CD4 tests drawn). For persons with no indications of being in care, it was then determined if the person continued to fill prescriptions (implying that they were getting prescriptions from someone other than a project clinic provider). For individuals from these two sites, persons were censored 1 day after the date of the last clinic visit if a person had no clinic visit, HIV viral load, or CD4 test drawn for >6 months but continued to fill prescriptions at the project pharmacies in the last 6 months of the project implementation period.
Statistical analysis
The proportion of persons retained in care was modeled using log binomial regression. Repeated measures were accounted for by using generalized estimating equations with an exchangeable working correlation structure, which assumes that the responses for individual subjects are equally correlated. Pre- and post-implementation retention for the entire study population was compared by including implementation period (pre or post) as the sole main effect in a model predicting retention. Similar comparisons were made within each level of the demographic predictors by including the main effect terms for implementation period, the demographic factor, and an implementation period by demographic factor interaction term.
The analysis also sought to identify the demographic factors and model interventions that predicted retention during the post-implementation period after controlling for baseline retention (whether a person was retained in care during the pre-implementation period). First, adjusted risk ratios (ARRs) for the levels of each demographic factor (age group, race/ethnicity, gender, and insurance status), the number of CMRs and other medication therapy review, type of model intervention (adherence support, pharmacist–patient action plan, pharmacist–clinic action plan), and the number of patient–pharmacist encounters were estimated separately.
Next, multi-variable models using only the demographic factors as predictors (controlling for baseline retention) were run. Then, multi-variable models including only the demographic predictors that were statistically significant at the 0.10 level in the previous stage were run separately with each intervention type and the number of pharmacist encounters included as predictors. The final multi-variable models were determined using forward stepwise variable selection, and only those factors that were significant at the 0.05 level were included.
Results
Project sites
The majority of the 10 project clinics were Infectious Disease/HIV specialty (70%), Ryan White (70%), Federally Qualified Health Center (FQHC), or FQHC look-alike clinics (60%) and were located in urban settings (80%). Project clinics served a median of 1186 [interquartile range (IQR): 1099–2391] patients with HIV and 2872 (IQR: 1123–8402) patients without HIV. All project pharmacies were community-based retail pharmacies and had operated a median of 2 (IQR: 1–8) years as part of a national retail chain HIV-specialized pharmacy program. Project pharmacies served a median of 504 patients with HIV (IQR: 291–608) and 2074 patients without HIV (IQR: 790–4250), monthly. Each project site enrolled between 26 and 107 patients.
Participant demographics
Of the 765 persons enrolled in the project, the largest proportions were male (73%), non-Hispanic black (43%), Medicaid-insured (34%), and had a median age of 48 years (interquartile range 38–55). A total of 680 and 625 persons were included in the pre- and post-implementation analyses, respectively (Fig. 1). There were no significant demographic differences between enrolled and included participants. Demographics for enrolled participants and the analytic cohorts are shown in Table 2.
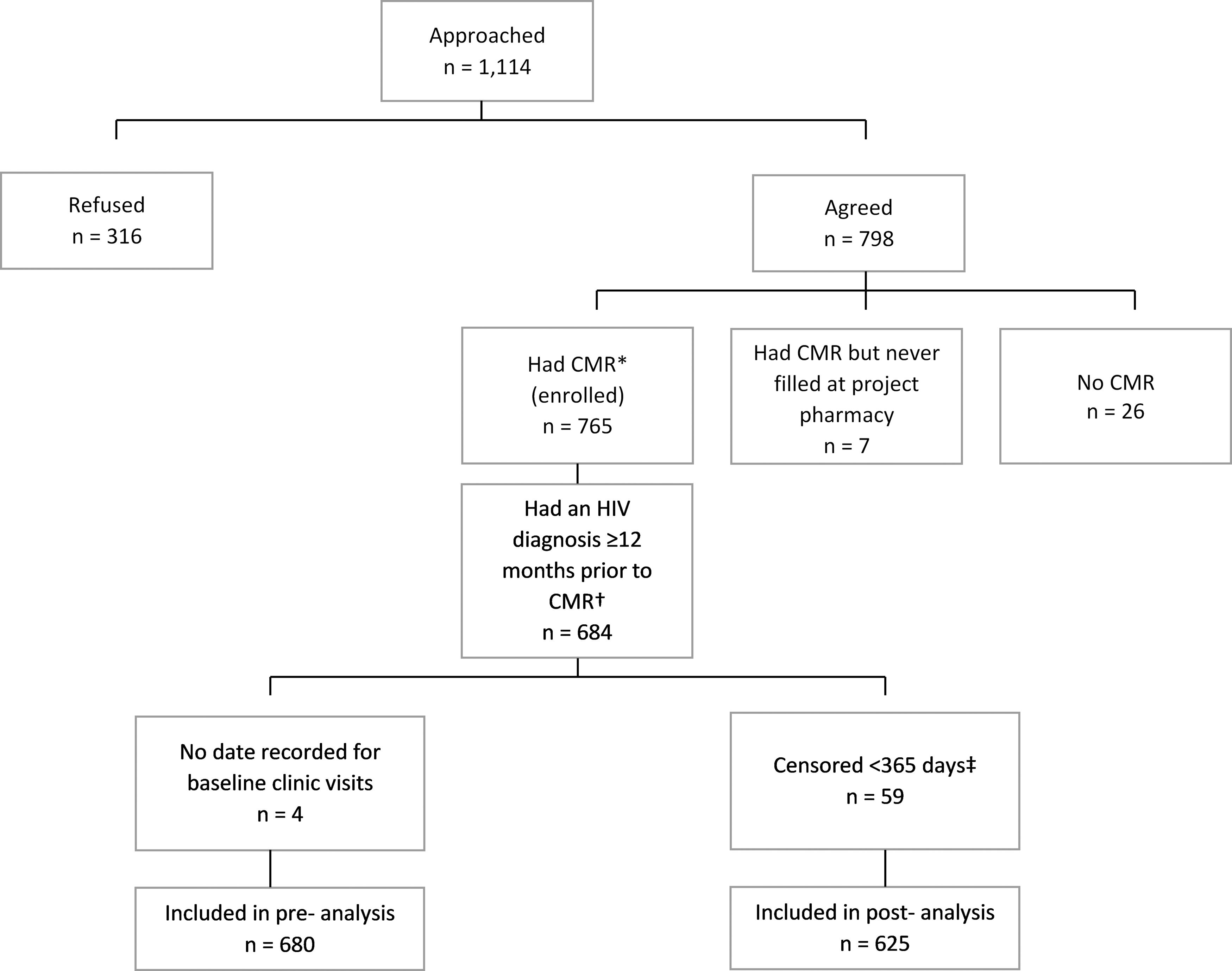
Flow diagram of inclusion in pre- and post-implementation retention in care analysis. *CMR = Comprehensive Medication Review. All persons who completed an initial CMR and who filled prescriptions at the project pharmacy were considered enrolled in the project. †Four hundred thirteen people had a documented date of HIV diagnosis ≥12 months before the initial CMR/enrollment date. There were 311 persons with a missing HIV diagnosis date; of these persons, 40 were excluded because they had no indication that they were HIV diagnosed ≥12 months before the initial CMR/enrollment date (no clinic visit of any kind, no HIV viral load or CD4 laboratory test result, no ARV prescriptions filled). ‡Persons were censored in the post-implementation period before they accrued sufficient follow-up time to meet the retention in care definition and were excluded from the analysis. Persons were censored for the following reasons: 1 was immediately censored, 7 people died, 2 were too ill, 12 moved out of the area, 10 transferred care to another clinic, 3 voluntarily withdrew from project, 18 were no longer filling prescriptions at the project pharmacies, and 6 were censored according to the censoring criteria for the 2 sites that did not collect censoring data.
Characteristics of Persons Within the Patient-Centered HIV Care Model
Characteristics at enrollment in project.
ADAP, AIDS drugs assistance program; IQR, interquartile range.
Model interventions
There were 720 CMRs and 904 other medication therapy reviews conducted during the post-measurement period. There were 5166 model interventions including 248 adherence support, 1104 pharmacist–patient action plans, and 3814 pharmacist–clinic action plans. Participants received a median of five interventions (IQR: 3–9). One hundred eleven persons received ≥1 adherence support, 317 received ≥1 pharmacist–patient action plans, and 598 received ≥1 pharmacist–clinic action plans. Six hundred twelve persons received more than one intervention and 310 persons received more than one type of intervention during the measurement period.
Retention in care
Overall, retention in care improved 12.9% from 60.7% to 68.5% (p = 0.002), pre- to post-model implementation. Retention improved among persons aged ≥50 years [12.3% increase; 62.5–70.2% (p = 0.029)], males [13.9% increase; 60.4–68.8% (p = 0.005)], persons seen in the Ryan White/ADAP clinics [22.4% increase; 63.9–78.2% (p = 0.023)], and non-Hispanic black persons [22.6% increase; 59.7–73.2% (p < 0.001)] (Table 3). Of the 267 people who were not retained during the pre-implementation period, 147 (55.1%) were retained post-implementation.
Proportion of Persons Within the Patient-Centered HIV Care Model Who Were Retained in Care, Pre- and Post-Model Implementation
Retention in care was defined as at least one medical visit with a physician, nurse practitioner, or physician assistant, in each 6-month period of a 12-month measurement period with a minimum of 60 days between medical visits. Pre-implementation retention was measured during the 12 months leading up to and including the enrollment date, and post-implementation retention was measured from 1 day after the enrollment date to 12 months forward.
The p-values are the tests of significance comparing the relative retention rate (pre- versus post-implementation) within each level of each factor.
ADAP, AIDS drug assistance program.
Factors associated with retention in care post-model implementation
After adjusting for baseline retention, non-Hispanic black persons [ARR 1.27, 95% confidence interval (CI) 1.08–1.48] and persons classified as “other or unknown” race (ARR 1.30, 95% CI 1.07–1.57) were more likely to be retained in care during the post-implementation period compared with non-Hispanic white persons. Persons with one or more pharmacist–clinic action plan (ARR 1.51, 95% CI 1.18–1.93) and persons with three or more encounters with the pharmacist (ARR 1.17, 95% CI 1.05–1.30) were more likely to be retained in care when compared with persons who did not receive a pharmacist–clinic developed action plan and those who had less than three pharmacist encounters, respectively. Neither adherence support nor patient–pharmacist action plan alone was significantly associated with retention (Table 4).
Factors Associated with Retention in Care in the Post-Implementation Period, After Controlling for Baseline Retention
ADAP, AIDS drug assistance program; ARR, adjusted risk ratio; CMR, comprehensive medication review; LCI, lower confidence interval; UCI, upper confidence interval.
Final multi-variable models
In the model that included only the demographic factors as predictors (after controlling for baseline retention), non-Hispanic black race/ethnicity (ARR 1.27, 95% CI 1.09–1.48) and race/ethnicity classified as “other or unknown” (ARR 1.36, 95%CI 1.14–1.63) were the only factors significantly associated with post-implementation retention. None of the demographic factors remained significant in the multi-variable model that included pharmacist–clinic action plan as a predictor. In the model that included the number of pharmacist encounters as a predictor, race/ethnicity was the only demographic factor that remained significant. The ARR for the number of pharmacist encounters (in the model that included both baseline retention and race/ethnicity) was 1.12 [95% CI 1.00–1.24 (p = 0.047)].
Discussion
The PCHCM sought to provide patient-centric HIV care by: building strong working relationships between community pharmacists and clinicians; addressing HIV medication therapy-related problems with the goal of collaborative action planning between community pharmacists and clinicians; addressing patients' medication-related concerns; and providing patients additional pharmacist-led adherence support. One of the goals of the model was to improve participants' retention in HIV care. Before model implementation, retention among participants was similar to national estimates at 60% and improved to 68%, post-implementation. While lower than the national retention in care goal of 90%, there was an overall relative increase in retention of 13%. 10
The model may have improved retention by involving each of the three pivotal parties in patients' care: patients, pharmacists, and clinic providers. First, pharmacists worked to increase patients' ability to self-manage their disease states and adhere to medication regimens. Studies have shown that patients who are more activated are more engaged in care and have better health outcomes. 18,19 Second, strong patient–provider relationships defined by trust and good communication have often been cited as facilitators to retention. 20 –23 The model sought to build stronger relationships between both the pharmacists and patients, and between the pharmacists and clinic providers. Finally, enhanced personal contact with patients has been shown to increase retention. 24
Although retention outcomes did not vary substantially among demographic groups or intervention categories pre- to post-implementation, the 23% increase in retention among non-Hispanic black persons is of particular note. Post-implementation retention among this group was 73%, which was higher than national estimates of 54% among non-Hispanic black persons. 25 This increase is important because failure to remain in care may contribute to disparities in survival, HIV transmission, and a higher incidence of new infections among this population. 26 A 2016 modeling study estimated that increasing the proportion of persons diagnosed with HIV in care can avert 52% of new infections. 27 Because black persons make up the greatest proportion of persons with HIV, retaining this population in care is critical to managing HIV in the United States.
The project results should be viewed in light of its limitations. First, a convenience sample was used, limiting generalizability. Second, project pharmacies provided services in-kind; the pharmacists were not reimbursed for model services, which may be required to scale this model. The measurement period for the analysis was limited to 1 year; because time has an impact on attrition, a longitudinal evaluation is needed to determine if the model has long-term effects. Many of the demographic subgroups were small; the analysis may have lacked the power needed to detect differences among these smaller groups. Finally, the PCHCM was a demonstration project, not a research study; the pretest–post-test evaluation design is not as strong as a study with control groups.
In conclusion, the PCHCM demonstrated how collaborations between community-based pharmacists and medical providers can lead to increased retention in HIV care. This model of care may be particularly useful for non-Hispanic black persons, who often are less likely to be retained in care.
Footnotes
Acknowledgments
The authors thank all the members of the Patient-Centered HIV Care Model team: Michael Aguirre, Osayi Akinbosoye, David M. Bamberger, Ben Bluml, Katura Bullock, Diane C. Burrell, Tim Bush, Clifton Bush, Kathy K. Byrd, Chad Cadwell, Nasima M. Camp, Roberto Cardarelli, Terri Clark, Patrick G. Clay, Andrew Crim, Angela Cure, Kristin Darin, Traci Dean, W. Ambrose Delpino, Michael DeMayo, Shara Elrod, Ashley L. Eschmann, David Farmer, Rose Farnan, Heather Free, Andrew Gudzelak, Andrew Halbur, Felecia Hardnett, Ronald Hazen, Heidi Hilker, John Hou, Brian Hujdich, Lisa Johnson, Heather Kirkham, James Lecounte, Sayuri Lio, Guanzhong Lo, Sondra Middleton, Brittany Mills, Christopher M. Nguyen, Linda Ortiz, Glen Pietrandoni, Kim Scarsi, Jon Schommer, Michael D. Shankle, Ram Shrestha, Daron Smith, Sumihiro Suzuki, Michael S. Taitel, Gebeyehu N. Teferi, Vikas Tomer, Louis Terres, Paul J. Weidle, Carmelita Whitfield, and Jason E. Willman. This work was supported by the Secretary's Minority AIDS Initiative fund and the Centers for Disease Control and Prevention (CDC) through a cooperative agreement (CDC RFA PS13-1315) with the University of North Texas Health Science Center's System College of Pharmacy. Walgreens Co. provided all services in-kind.
Author Disclosure Statement
No competing financial interests exist.