
Abstract
Scant research has explored the engagement of transgender (trans) women living with HIV (WLWH) in the HIV care cascade, particularly in universal health care settings like Canada. This convergent parallel, mixed-methods study drew on cross-sectional quantitative data from 50 trans WLWH in the Canadian HIV Women's Sexual and Reproductive Health Cohort Study (CHIWOS) and qualitative semistructured interview data from a subsample of 11 participants. Descriptive analyses were used to describe proportions of trans WLWH at five steps of the HIV care cascade and bivariate analyses to determine associations between hypothesized barriers/facilitators and HIV care cascade outcomes. Framework analysis was used to describe barriers and facilitators to HIV care engagement. Quantitative and qualitative data were then compared and contrasted. While use of purposive sampling, including recruitment through AIDS Service Organizations and HIV clinics, may have led to oversampling of trans WLWH who already had access to care, gaps were still seen in antiretroviral therapy (ART) outcomes (current ART use: 78%; ≥95% adherence among those currently taking ART: 67%). The number of years living with HIV was positively associated with HIV care cascade engagement. Factors associated with lower engagement included: higher health-related quality of life, depressive and post-traumatic stress disorder symptoms, barriers to access to care, transphobia, HIV-related stigma, and housing insecurity. Qualitative findings converged and expanded on how physical health, and social and structural marginalization, influence trans WLWH's engagement in HIV care. Qualitative findings elaborated on the importance of ART-related factors in impeding or facilitating engagement, including concerns about feminizing hormone–ART drug–drug interactions. Mixed-methods findings reveal how trans WLWH experience barriers common to other people living with HIV, and also experience unique barriers as a result of trans and HIV experiences.
Introduction
In 2014, the Joint United Nations Program on HIV/AIDS (UNAIDS) identified the 90-90-90 targets—aiming by 2020 that 90% of all people living with HIV (PLWH) are diagnosed, 90% of those diagnosed are receiving sustained antiretroviral therapy (ART), and 90% of those receiving sustained ART are virally suppressed. 1 These outcomes are situated within the HIV care cascade, a series of steps from diagnosis through linkage to care, retention in care, initiation of ART, adherence to ART, and ultimately, viral suppression. 2,3
As each step has the potential to be interrupted, it is important to understand where attrition occurs along the cascade, for specific populations most affected by HIV, to inform step-specific interventions to improve HIV care engagement, prevent HIV-related morbidity, and reduce HIV transmission. 4,5 One such population is transgender (trans) women, 6 a diverse group of people labeled male at birth who identify as either girls/women or on a transfeminine spectrum. Globally, trans women—particularly trans women of color—experience disproportionately high rates of HIV compared with cisgender (cis) adults whose gender identity and sex labeled at birth are congruent. 7,8
Research emerging from the United States suggests that compared with cis people, trans women have lower rates of HIV testing, 9 and trans women living with HIV (WLWH) have lower retention in care, 10 ART use, 11 ART adherence, 12 –15 and viral suppression. 15,16 There are no comparable published studies of trans WLWH's engagement in the HIV care cascade in Canada. Such studies are needed to understand and address barriers to access to HIV care for trans WLWH, given the notable differences in health care and human rights policies for trans persons (i.e., Bill C16).
Access to each point along the HIV care cascade is facilitated or impeded by contextual factors. 3 The few quantitative US studies, assessing correlates of HIV care cascade outcomes for trans WLWH, have predominantly focused on ART treatment adherence 12,14,17,18 and viral suppression, 13,18,19 with little attention paid to other steps (e.g., linkage to care, ART initiation). Qualitative studies which focus solely on the experiences of trans WLWH have identified trans-specific barriers to HIV care engagement, such as transphobia from health care providers and concerns about drug–drug interactions between ART and feminizing hormones, 20,21 suggesting the importance of analyses focused on these and other trans-specific experiences.
One quantitative study of trans WLWH (n = 59) conducted by Sevelius et al. 18 found that lower stress appraisal of transphobic experiences, higher importance of gender affirmation, and adherence to hormone therapy were associated with higher odds of ART adherence. In the same study, lower stress appraisal of transphobic experiences was associated with higher odds of viral suppression. 18 However, additional factors such as access to gender-affirming care and provider knowledge of trans health issues are under explored. Both quantitative and qualitative studies include small samples of trans WLWH, which poses challenges to comprehensively understanding HIV care outcomes. 22 –24 To help remedy this, quantitative data may be complemented with qualitative data to more comprehensively attend to the ways in which trans WLWH conceptualize their engagement in HIV care and to identify barriers and facilitators. 25
This mixed-methods study had two objectives, the first to assess the proportion of trans WLWH who (1) have ever accessed HIV care, (2) received any HIV care in the past year, (3) were taking ART at the time of the interview, (4) reported optimal adherence, and (5) had a self-reported undetectable viral load. The second objective was to comprehensively describe barriers and facilitators to HIV care cascade engagement at each step. Understanding where attrition occurs along the HIV care cascade, and barriers to HIV care engagement, may inform the design of tailored interventions to optimize HIV care for trans women.
Methods
Study design, sample, and quantitative data collection
This study utilized a convergent parallel mixed-methods design, which included the separate collection and analysis of quantitative and qualitative data to address the same research questions, followed by assessment of how data converged, diverged, and/or expanded an understanding of trans WLWH's HIV care cascade engagement. 26 Quantitative baseline survey data collected from 2013 to 2015 in the provinces of British Columbia, Ontario, and Quebec, Canada, for the community-based participatory Canadian HIV Women's Sexual and Reproductive Health Cohort Study (CHIWOS) were utilized. 27
Trained peer research associates (PRAs) recruited 1422 WLWH 16 years of age or older through word of mouth by way of multiple mechanisms (e.g., PRA networks, online, clinics). 27 PRAs obtained written informed consent and then utilized an online survey platform to administer a structured questionnaire in English or French. Participants included in this study's present analyses were those who (1) selected male or intersex as their sex labeled at birth, (2) selected woman or trans woman as at least one of their gender identities (n = 54), and (3) had complete data about their access to HIV care (n = 50).
Quantitative variables
Five outcomes representing steps of the HIV care cascade were assessed.
(1) Ever accessed HIV care was measured utilizing the question “After receiving your HIV diagnosis, when did you first access HIV medical care?” (never versus ever). (2) Received any HIV care in the past year was measured among participants who had ever accessed care utilizing the yes/no question, “Have you received any HIV medical care in the past year?.” (3) Current ART use was measured among the participants who reported ever accessing HIV care by asking “Have you ever taken antiretroviral medication for your own health,” and participants were classified as never took ART, not currently but previously took ART, and currently taking ART. Since all participants who initiated ART were currently taking ART, these outcomes were dichotomized as never versus currently for further analyses. (4) ART adherence was measured among participants who reported current ART use by asking participants to report the percentage of ART medication they had taken in the last month (0–100%), dichotomized to suboptimal (<95%) versus optimal adherence (≥95%), which is considered a standard cutoff for maximum ART benefits. 28,29 (5) Viral suppression was measured among the participants who reported current ART use by asking them to indicate if their most recent viral load was undetectable (e.g., below 50 copies/mL) or detectable (e.g., over 50 copies/mL). 30
Covariates included sociodemographic, clinical, intrapersonal, interpersonal, structural, and trans-specific factors. Sociodemographic factors included age (continuous), education (less than high school, high school or higher), annual personal income (<$20,000, ≥$20,000), and ethnoracial group (white, Indigenous, Latina, and other; dichotomized as white versus person of color for bivariate analyses due to small cell sizes). Clinical factors included years living with HIV (measured continuously) and overall physical health-related quality of life (HR-QoL) (6-item SF-12 physical health component subscale, 31 higher score indicates better physical health, range: 15.75–68.43, Cronbach's alpha = 0.74). All score ranges and Cronbach's alpha are presented for the current analyses.
Intrapersonal variables included mental HR-QoL (6-item mental health component subscale of SF-12, 31 higher score indicates better mental health, range: 5.84–66.32, Cronbach's alpha = 0.85), hazardous alcohol use (adapted 3-item AUDIT-C, 32 higher score indicates more hazardous alcohol use, range: 0–9, Cronbach's alpha = 0.67), history of injection drug use [(currently/not currently but previously) vs. never], and depressive symptoms [10-item Center for Epidemiologic Studies Depression Scale (CES-D), 33 higher score indicates more frequent depressive symptoms, range: 0–30, Cronbach's alpha = 0.91].
Post-traumatic stress disorder (PTSD) symptoms were measured using the 6-item PTSD Checklist–Civilian Form 34,35 (higher score indicates more severe PTSD symptoms, range: 6–29, Cronbach's alpha = 0.87), and resilience was measured using the 10-item Resilience Scale 36 (higher score indicates higher resilience, range: 29–70, Cronbach's alpha = 0.91). Negative self-image HIV-related stigma was measured using the 3-item negative self-image subscale (e.g., having HIV makes me feel unclean) of the HIV Stigma Scale (higher score indicates more stigma, range: 0–12, Cronbach's alpha = 0.88). 37,38
Interpersonal factors included social support, HIV-related stigma (personalized, disclosure), and violence in adulthood (ever having experienced any form of violence vs. no). Social support was measured using the 4-item Medical Outcome Study Social Support Survey 39 (higher score indicates more social support, range: 4–20, Cronbach's alpha = 0.87), with each dimension of social support (emotional/information, tangible, affectionate, positive social interaction) coded separately. Personalized HIV-related stigma, which includes HIV-related stigma experienced in interpersonal relationships and disclosure HIV-related concerns were measured using subscales from the HIV Stigma Scale 37,38 (3-items, higher score indicates more stigma, range: 2–12, Cronbach's alpha = 0.85 and 2-items, higher score indicates more stigma, range: 1–8, Cronbach's alpha = 0.76, respectively).
Housing insecurity, public attitudes (community-level) HIV-related stigma, and barriers to access to care were structural factors explored in this analysis. Housing insecurity was dichotomized as insecure (self-contained room, transition house, halfway house, safe house, couch surfing, outdoors on street, parks, or in a car) versus secure [apartment (own/rent) or a house (own/rent)]. Concern about public attitudes toward PLWH, (e.g., most people think a person with HIV is disgusting) was measured using a 2-item subscale of the HIV Stigma Scale (higher score indicates more stigma, range:1–8, Cronbach's alpha = 0.78). The 12-item Barriers to Care Scale (BACS) was used as a composite measure of barriers to accessing medical and social care, some overlapping with other measures (e.g., community-level HIV stigma, employment), and others newly assessed with the BACS (e.g., geographical barriers) 40 (higher score indicates more problematic barriers, range: 12–48, Cronbach's alpha = 0.94).
Trans-specific factors included feminizing hormone use (yes vs. no), perceived knowledge of HIV physician about trans health issues, comfort discussing trans health issues with one's family physician, ever experiencing transphobia in HIV care, physician discussion of drug–drug interactions, and experiences of transphobia more broadly. Perceived knowledge of physician on trans health issues was dichotomized as more (very/somewhat knowledgeable) versus less knowledgeable (not very/not at all knowledgeable/HIV physician has never talked to me about trans health). Comfort discussing trans health issues with one's family physician was dichotomized as more (very comfortable/comfortable) versus less (uncomfortable/very uncomfortable/do not know—I have never talked to my family doctor about trans health issues).
Ever having experienced transphobia in HIV care was measured using a question from the Trans PULSE survey 41 by asking participants if 1 of 10 discriminatory acts or other had occurred in the context of HIV care (e.g., HIV care provider refused to see you or ended your care because you were trans), dichotomized as any (any of the 10 and/or other indicated) versus none reported. Those who had ever accessed HIV care, reported taking hormones, and had informed their doctor of hormone use, were asked whether their doctor had discussed possible drug–drug interactions between HIV medications and hormones (yes/no). Transphobia more broadly was measured using a 9-item scale from Trans PULSE, pretested for content validity and clarity that captured enacted discrimination and violence as well as everyday experiences of stigma 42 (higher score indicates more transphobia, range: 4–27, Cronbach's alpha = 0.89).
Quantitative analyses
For each of the five dichotomous HIV care cascade outcomes, proportions and bootstrapped 95% confidence intervals (CIs) were calculated using 500 replicates. 43 Bivariate analyses were then conducted to test for statistically significant associations (p < 0.05) between covariates and each of the five dichotomous HIV care cascade outcomes. For categorical covariates, Fisher's exact tests were used. Mean was compared using t-tests. All analyses were conducted using SPSS Version 24. 44
Qualitative interviews
A subset of trans WLWH who completed the baseline CHIWOS survey (n = 11) participated in an open-ended, semistructured, individual interview in 2017–2018, focused on barriers and facilitators to their engagement in HIV care. For example, participants were asked “What, if anything, gets in the way of you taking your HIV medications? What supports you in taking your HIV medications?”. PRAs were encouraged to purposively recruit participants with varied levels of HIV care engagement (e.g., those engaged in HIV care, those who had never accessed HIV care). Of 11 interviews, 10 were conducted by the first author and 1 by a PRA. Interviews (25–100 min; median 90 min) were conducted using a semistructured interview guide developed to explore multilevel barriers and facilitators among WLWH of diverse experiences and identities, consistent with a social ecological approach that recognizes that a woman's access to care is influenced by factors operating and interacting at multiple levels. 45,46 Interviews were digitally recorded and transcribed verbatim.
Participants received a $50 honorarium for their participation in the baseline quantitative survey and $50 for their participation in an interview. Ethics approval for CHIWOS was obtained from the Research Ethics Boards of Women's College Hospital (Ontario), Simon Fraser University and the University of British Columbia/Providence Health (British Columbia), and McGill University Health Center (Quebec). Ethics approval for this subanalysis, including the qualitative component, was also received from the University of Toronto and Simon Fraser University/University of British Columbia/Providence Health.
Qualitative analyses
Qualitative interviews were analyzed by the primary investigator (A.L.-D.) following the six steps of framework analysis, 47 including: familiarization with the data; open coding of three transcripts to develop a preliminary analytic framework; revising and testing the analytic framework on three additional transcripts; applying the analytic framework to all transcripts through line-by-line coding; charting data into a table summarized by codes and participants; and mapping and interpreting data. Rigor was established through illustrating key themes with demonstrative quotes, documenting analytic decisions and data interpretations, sharing the charting process with additional team members (E.S.K., C.H.L., P.A.N., and G.R.B.), and debriefing with trans members of the CHIWOS Trans Community Advisory Board. 48,49 Analyses were facilitated by the use of NVivo 11.4.0. 50
Mixed-methods analyses
Mixed-methods analyses included first specifying dimensions for quantitative and qualitative data comparison (e.g., barriers and facilitators to HIV care cascade engagement) and information to be compared [e.g., proportion difference/mean difference, associated 95% for factors associated with HIV care cascade outcomes (quantitative) and participant narratives about barriers and facilitators to HIV care engagement (qualitative)]. Next, comparisons were visually represented through a summative joint display and considering how results converged, diverged, or expanded understanding. 26
Results
Quantitative results
Participant characteristics
Quantitative participant characteristics (n = 50) are reported in Table 1. Participants were a mean age of 41.0 years (SD: 10.09), predominantly had a high school education or higher (83.7%), an annual personal income less than $20,000 CAD per year (89.8%), and were white (38.0%) or Indigenous (34.0%).
Sociodemographic and Clinical Characteristics of a Sample of Trans Women Living with HIV in Canada (n = 50) a
Unless otherwise specified.
Other ethnicities include Arab, West Asian, black/African/Caribbean, and multiple races/multiracial ethnicity. Categories are collapsed to protect the confidentiality of participants.
CAD, Canadian dollar; SD, standard deviation.
HIV care cascade
Of the 50 participants, 92% (95% CI: 84–100%) had ever accessed HIV care and, among the 46 who had accessed care, 91% (95% CI: 82–98%) had received any HIV care visit within the past year. Approximately three-quarters (78%, 95% CI: 67–89%) of women who had ever accessed care had initiated ART use, and all who had initiated were also currently using ART. Of the 36 currently using ART, two-thirds (67%, 95% CI: 52–83%) reported ≥95% adherence. Most, who were currently using ART, had a self-reported undetectable viral load (89%, 95% CI: 77–97%) (Fig. 1).
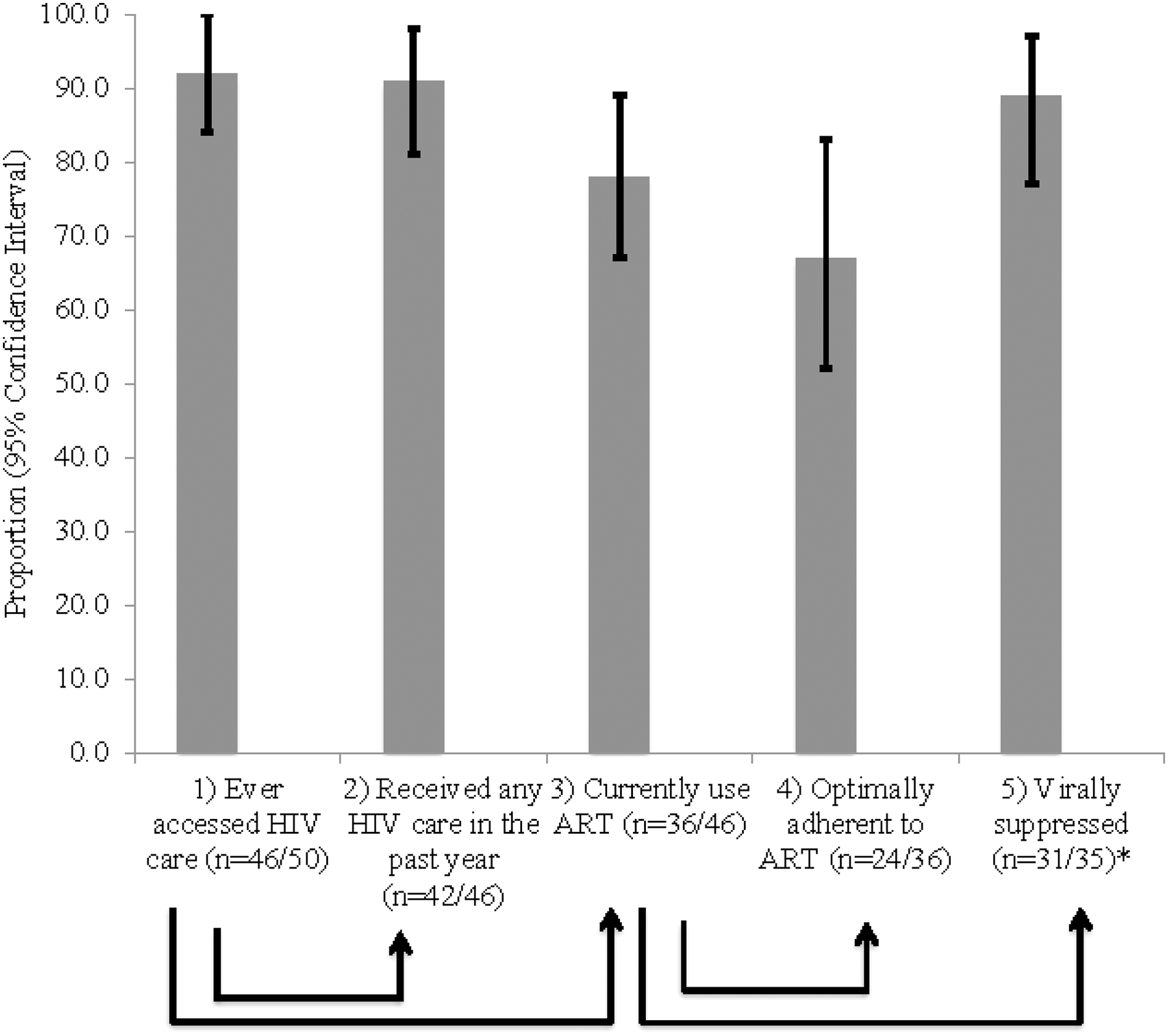
Proportion of trans women living with HIV at each step in the HIV care cascade (n = 50). Ninety-five percent confidence intervals for proportions were calculated using bootstrap variance estimation technique using a set of 500 replicates. Self-reported ART optimal adherence was defined as reporting ≥95% of ART in the past month. Self-reported viral load suppression <50 copies/mL. *One participant was missing data for viral load. ART, antiretroviral therapy.
Bivariate analyses
Compared with trans women who had ever accessed HIV care, trans women who had never accessed HIV care: had lived with HIV for a shorter period of time, reported a higher physical HR-QoL, had a lower prevalence of experiencing violence in adulthood, and reported experiencing more barriers to access (Table 2). Compared with trans women who had accessed any HIV care in the past year, those who had not accessed care reported more tangible social support and positive social interaction, but also experienced more transphobia (Table 2).
Quantitative Findings of Barriers and Facilitators to Ever Accessing HIV Care and Receiving Any HIV Care in the Past Year Among Trans Women Living with HIV
Proportion difference and mean difference calculated by subtracting Yes proportions or mean from No proportions or mean; * p < 0.05, ** p < 0.01, *** p < 0.001; Fisher's exact tests were used to examine significant associations between proportions. t-Tests were used to examine significant associations between means.
Not collected for people who have never accessed HIV care.
One hundred percent of participants with complete data on these variables reported receiving any HIV care in the past year.
CI, confidence interval; HR-QoL, health-related quality of life; PTSD, post-traumatic stress disorder.
Compared with trans women who were currently using ART, trans women who were not using ART were younger and had been living with HIV for a shorter period of time.
Women not currently using ART reported a lower prevalence of experiencing violence in adulthood; however, they also reported more social and structural marginalization, including higher personalized HIV-related stigma, barriers to access to care, and transphobia, as well as a higher prevalence of insecure housing (Table 3). Adherence to ART was only associated with intrapersonal outcomes: trans women who reported suboptimal (<95%) adherence reported experiencing more depressive and PTSD symptoms than trans women who reported ≥95% adherence. Compared with trans women who reported an undetectable viral load, a higher proportion of those reporting a detectable viral load were uncomfortable or very uncomfortable discussing trans health issues with their family physician. Tangible social support was also higher among this group (Table 4).
Quantitative Findings of Barriers and Facilitators to Current Antiretroviral Therapy Use and Adherence Among Trans Women Living with HIV
Proportion difference and mean difference calculated by subtracting Yes proportions or mean from No proportions or mean; * p < 0.05, ** p < 0.01, *** p < 0.001; Fisher's exact tests were used to examine significant associations between proportions. t-Tests were used to examine significant associations between means.
ART, antiretroviral therapy; CI, confidence interval; HR-QoL, health-related quality of life; PTSD, post-traumatic stress disorder.
Quantitative Findings of Barriers and Facilitators to Viral Suppression Among Trans Women Living with HIV
Proportion difference and mean difference calculated by subtracting Yes proportions or mean from No proportions or mean; * p < 0.05, ** p < 0.01; Fisher's exact tests were used to examine significant associations between proportions. t-Tests were used to examine significant associations between means.
CI, confidence interval; HR-QoL, health-related quality of life; PTSD, post-traumatic stress disorder.
Qualitative results
The qualitative subsample included trans WLWH from Toronto (n = 5), Vancouver (n = 3), and Montreal (n = 3), inclusive of both Anglophone (n = 9) and Francophone (n = 2) participants, ranging in age from 20s to 60s (median 40s), of white (n = 4), Indigenous (n = 3), or other ethnicity, inclusive of Latina, black/African/Caribbean, and women of multiracial ethnicity (n = 4), and mostly living with HIV >14 years (n = 8). Participant narratives did not follow the steps in the HIV care cascade as utilized for quantitative outcomes, focusing more explicitly on their experience of HIV diagnosis and linkage to HIV care and their experiences of engagement within HIV care more generally, as opposed to any one specific step. To increase comparability between quantitative and qualitative data, qualitative findings are presented as barriers and facilitators affecting linkage to HIV care postdiagnosis; ART initiation/use; ART adherence; and, multiple steps/ongoing engagement in HIV care. Additional demonstrative quotes are presented in Table 5.
Qualitative Findings of Barriers and Facilitators to HIV Care Cascade Engagement Across the Cascade Among Trans Women Living with HIV
ART, antiretroviral therapy; WLWH, women living with HIV.
Linkage to HIV care postdiagnosis
Participants described a postdiagnosis period characterized by rejection and/or disbelief about their diagnosis, facilitated by feeling physically well; as participant 4 described, “I couldn't feel it. It wasn't something that I knew was taking place in my body…I don't believe it's happening to me.” Some participants experienced immediate grief and a sense of life being over or that they would now “lose everything” (P1). Half of participants expressed some self-blame or judgment about their HIV status and/or a sense of fatalism that an HIV diagnosis was an eventuality. As participant 4 reported, “I wasn't surprised.” Yet, at the same time, an HIV diagnosis represented a significant shift in participants' perceptions of self. In multiple cases, it took a period of several years for participants to initiate HIV care.
Engagement in HIV care was facilitated by a reduced sense of fatalism, “You are positive. It's not the end of the world” (P1) and increased sense of self-worth. Prior engagement with health care, social service, and trans communities facilitated more timely linkage to HIV care.
ART initiation/use
The most commonly cited barrier to ART initiation/use among trans WLWH was concern about drug–drug interactions between ART and feminizing hormones. Those who concurrently took ART and hormones described concerns about adverse events, with two participants reporting adverse events, including negative impacts on their physical transition and feeling physically ill. Others reported on other women's concerns about drug–drug interactions: “They [other trans women] are scared to come out HIV positive because they are seeking the hormone treatment…” (P1). Two participants who were not currently taking ART held strong personal beliefs that ART use would negatively impact their physical and/or mental health. For example, participant 6's past experience seeing others die of complications due to HIV while taking ART led her to decide she did not want to take ART and would prefer to see out the untreated progression of her HIV.
Declining physical health was a facilitator of ART initiation, as it often precipitated ART recommendations from HIV care providers or study participants asking about ART. Among those living with HIV in the early days of ART, side effects were a serious deterrent. For participant 6, this, in combination with other factors, led her to stop taking ART altogether: “It [ART] was making me really sick and I said, you know what, no.” However, treatment advancements such as the development of regimens perceived to have fewer side effects facilitated ART use. For one participant, the later regimens were also seen to have less of an impact on the effectiveness of her feminizing hormone regimen.
ART adherence
Although in the quantitative results the largest attrition was seen between current ART use and optimal adherence, most qualitative participants did not discuss challenges with adherence to ART, even with prompting. For those who did discuss adherence, participants noted that adherence was impeded by changes to daily routines and medication changes as well as medication fatigue. Concerns about drug resistance and perceived physical benefits of ART adherence, particularly having an undetectable viral load and an increase in CD4 count, facilitated adherence.
Ongoing engagement in HIV care
Participants faced multiple life circumstances that impeded their engagement in HIV care, including trauma, substance use, social isolation, violence, and housing insecurity. Almost all women's narratives were characterized by multiple losses and punctuated by verbal harassment and physical and sexual violence, events that happened both recently and over the course of their lives. The majority of participants also experienced some period of homelessness early in their transition. Participant 3 reflected that maintaining an ART regimen is “very hard especially for people living on the street.”
Participants also described both HIV and transphobia in health care as barriers to access to HIV care. Although HIV care was perceived as safe relative to other care environments (e.g., emergency departments), trans WLWH perceived HIV stigma from laboratory technicians and in hospital settings, where technicians and nurses were seen as hesitant toward and whispering about them. Two participants highlighted experiences of transphobia with HIV care providers. These included being misgendered in public spaces, breaching their confidentiality, and negatively impacting their safety. Some participants also described organizational barriers to ongoing engagement in HIV care, including a lack of appointment reminders and long wait times.
Participants' relationships with HIV health care providers were generally positive, which facilitated their engagement in HIV care. Women described how their providers displayed nonjudgmental attitudes through supporting them in difficult times in their lives. Moreover, providers reportedly showed a genuine interest in their lives beyond their medical care and participants described valuing when providers accepted their health care decisions, such as choosing not to take ART. Some participants connected physician's acceptance to having a level of trans cultural competency/knowledge of trans health issues. The majority of trans WLWH felt that their HIV care providers were “competent at both” (P10) and that they could “touch base on both” (P4) trans and HIV health issues. Having health insurance through social assistance was a frequently cited facilitator of access to HIV care, and particularly ART use.
Mixed-methods results
Some overlap in barriers and facilitators to trans WLWH's engagement in the HIV care cascade were identified in quantitative and qualitative findings (Fig. 2). Qualitative findings expanded on and helped to explain quantitative associations between HIV care cascade outcomes and years living with HIV, physical HR-QoL, violence, transphobia, HIV stigma, housing instability, trauma, and barriers to access to care. For example, quantitative findings showed that having a higher physical HR-QoL is negatively associated with ever accessing HIV care. Qualitative findings showed how physical wellbeing contributes to women's disbelief or denial of their HIV status, inhibiting their linkage to HIV care postdiagnosis, and how declining physical health is the catalyst for initiating and maintaining current ART use. For another example, quantitative findings showed that trans WLWH who reported suboptimal adherence experienced a higher frequency of PTSD symptoms; qualitative findings showed the context of violence and stigma within which trauma may proliferate for trans WLWH.
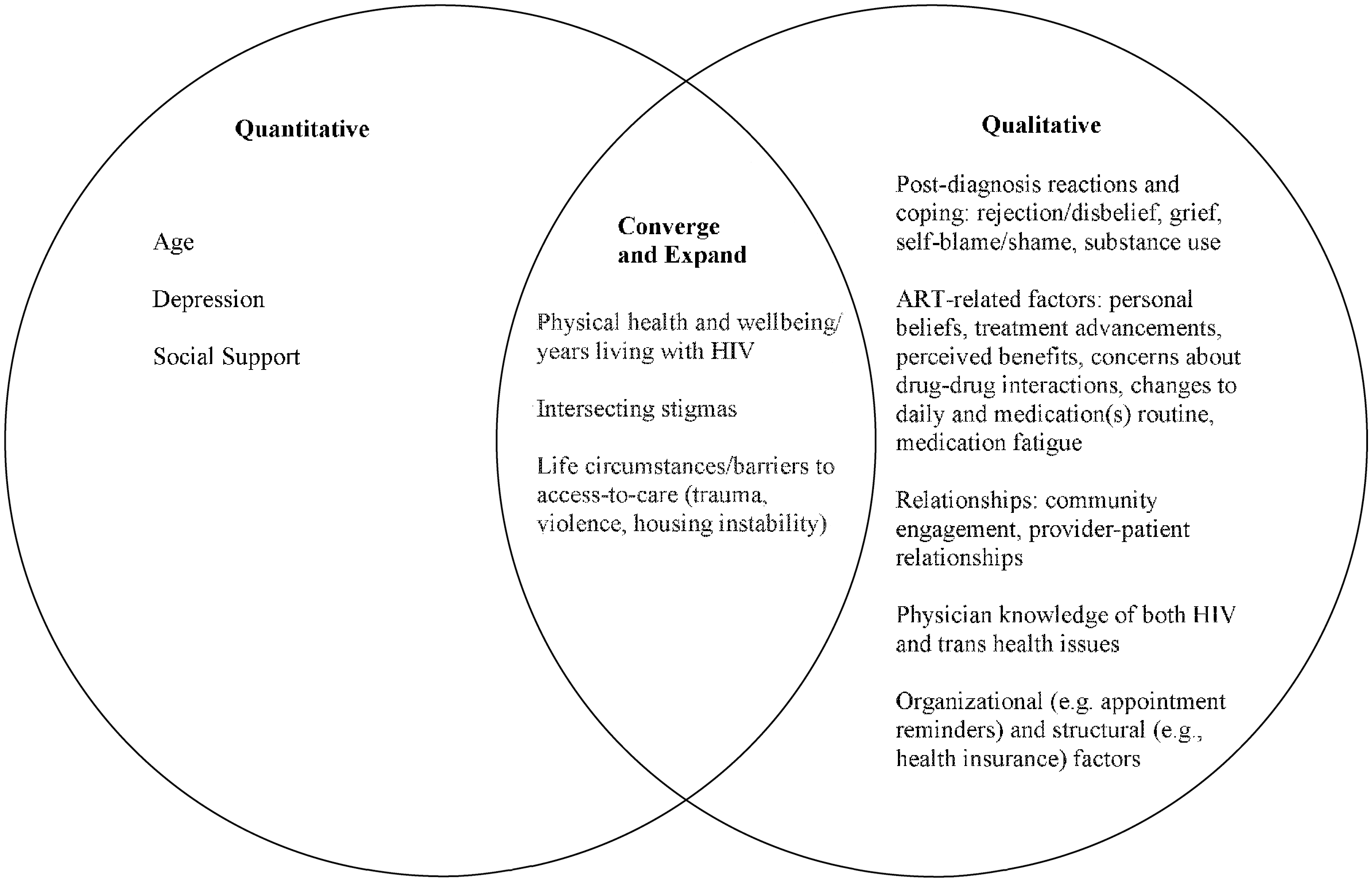
Joint display of mixed-methods findings about barriers and facilitators to HIV care cascade engagement among trans women living with HIV. ART, antiretroviral therapy.
As mentioned, while the qualitative interview guide was designed to ask questions about each step in the HIV care cascade, participants chose to focus more on specific steps (e.g., linkage to care postdiagnosis, ongoing engagement in HIV care, generally) and less on others (e.g., ART adherence). There were some divergent findings with respect to facilitators to HIV care that were highlighted through the qualitative interviews (e.g., physician knowledge of both HIV and trans health issues), that were not identified through bivariate analyses. However, the slight difference in how the quantitative question pertaining to knowledge was asked, the small sample size, and the uniformity in the response to this question (e.g., everyone who received HIV care in the past year reported their HIV physician to be very/somewhat knowledgeable about trans health issues) limited our ability to test for and/or detect a significant quantitative association. There were other findings, such as the association between different types of social support and HIV care cascade outcomes, and the importance of the interpersonal relationship between trans WLWH and their HIV care providers were highlighted only through quantitative or qualitative findings, respectively, highlighting the importance of drawing on both types of data to comprehensively understand engagement in HIV care among trans WLWH.
Discussion
This study comprehensively described the HIV care cascade for trans WLWH in Canada, utilizing mixed methods. Attrition from the cascade occurred at all stages, from 8% (95% CI: 0–16%) lost at linkage to care, to 22% (95% CI: 11–34%) lost at ART initiation/current ART use, and 33% (95% CI: 18–51%) lost at ART adherence. The findings contribute to the global literature suggesting that trans WLWH may not receive the numerous benefits of sustained ART use at optimal adherence levels, 12 –15 such as reduced morbidity and mortality. 51,52 Ultimately, findings suggest that ART initiation may be a critical point of intervention, particularly for achieving the 90-90-90 goals. 30
Beyond documenting gaps in access to HIV care for trans WLWH, this study builds on research documenting socioecological barriers and facilitators of HIV care among trans WLWH 12 –14,17 –19,53 by highlighting how HIV status and gender identity function together to produce a unique context of HIV care access for trans WLWH. Qualitative findings converged and expanded on our understanding of how physical health and wellbeing, multiple stigmas, and challenging life circumstances (e.g., violence, trauma), influence engagement in HIV care. Finally, the qualitative findings uniquely demonstrated the complexity of women's experiences of coping with an HIV diagnosis, their specific experiences with and concerns about ART use, and the importance of key relationships, trans women-specific clinical knowledge, organizational supports, and policies in shaping their engagement in both discrete steps of the HIV care cascade and HIV care more broadly.
In light of the recent WHO recommendation that ART be initiated for all PLWH at any CD4 count, 30 future studies are needed to explore ART prescribing practices for trans WLWH. Building on the literature on HIV care providers more broadly, 54 future qualitative studies can explore how providers cultivate and maintain trust with trans WLWH specifically. Interventions may also be warranted that link young trans women to care sooner after diagnosis and emphasize the importance of ART to optimize health and wellbeing, irrespective of clinical disease progression.
One such intervention, Antiretroviral Treatment Access Study (ARTAS), which used strength-based case management to increase linkage to and retention in HIV care among those recently diagnosed, is identified as an evidence-based HIV prevention intervention by the US Centers for Disease Control and Prevention. 55 –57 By combining individual-level counseling with referrals to social support groups, social determinants of health (e.g., housing), and advocacy for the client's needed medical care and support services, the ARTAS intervention is one promising approach to address the multi-level barriers to care for trans WLWH in this study.
At an intrapersonal level, trans WLWH reporting suboptimal ART adherence had almost double the depressive symptom (CES-D) score of those reporting greater than or equal to 95% adherence. These findings corroborate those of a meta-analysis which identified depressive symptoms as one of the factors most strongly negatively correlated with ART adherence among PLWH. 58 One study of trans women in Ontario, Canada (n = 191) showed that approximately two-thirds of participants had clinically significant CES-D scores, suggesting that depression may be a major issue for this population regardless of HIV status. 59 A recent study conducted with PLWH (n = 1811) in four countries (Canada, Namibia, Thailand, United States) identified several intrapersonal factors associated with less than optimal adherence, including depression and stressful life events. 60 Future research should aim to better understand the events that lead to depression and trauma among trans WLWH in Canada and to explore trauma-informed care, to mitigate the potential impacts of unaddressed mental health issues on ART adherence. 61
Perhaps most importantly, this study shows that transphobia is higher among those with limited access to HIV care, including lower ART initiation and adherence. Future studies should further explore how multiple types and forms of stigma experienced within and external to HIV care impact trans women's engagement in care. Perhaps due to the small sample size, it is important to note that most trans-specific HIV physician factors (e.g., perceived knowledge of HIV physician about trans health issues, ever experienced a transphobic event in a health care setting) were not associated with access to HIV care, contrary to qualitative findings. One-sixth (17%) of participants had experienced a transphobic event in an HIV health care setting, which is relatively low based on studies conducted among trans women in other care settings. 62
However, quantitative results showed that a higher proportion of those reporting a detectable viral load were uncomfortable or very uncomfortable discussing trans health issues with their family physician, and qualitative findings showed the deleterious effects trans and HIV stigma can have on HIV care engagement and HIV clinical outcomes. Taken together, these findings suggest that the creation of gender-affirming HIV services—safe places where trans women are met with welcoming attitudes from health care personnel 20,63,64 —is important but insufficient for increasing access to HIV care for trans WLWH.
The quantitative study findings did not show feminizing hormone use to be associated with initiating ART use or ART adherence, similar to Baguso et al. 12 However, hormone therapy has been described qualitatively as an entry point into HIV care 20,63 –65 and qualitative findings in this study showed that concerns about drug–drug interactions were commonly expressed among trans WLWH; this suggests the importance of further exploring women's perceptions of having experienced drug–drug interactions and/or fear of potential drug–drug interactions, as well as the need for biomedical investigations.
This study has several limitations. The small cross-sectional dataset precluded causal analysis, and the bivariate analyses that were possible did not include confounder control. Multiple bivariate analyses increased the overall risk of type 1 error. While without purposive (nonrandom) sampling by PRAs it is possible we may not have recruited any trans women at all, sampling predominantly at ASOs and HIV clinics may have led to oversampling of trans WLWH at points of stability or undersampling of trans WLWH experiencing marginalization, and certainly led to over sampling of trans WLWH primarily from urban, well-resourced, settings. Future studies should seek to recruit rural trans WLWH, who may experience more barriers to accessing care as well as more challenges with disclosure and social engagement and research participation. Collected data were self-reported and, therefore, subject to social desirability and recall bias. The small sample size, which decreased at each step along the cascade due to attrition resulted in insufficient power to detect significant differences of moderate to small sizes.
However, this study also has notable strengths. Community advisory boards were formed to enhance targeted recruitment of groups overrepresented in Canada's HIV epidemic, including trans women. Social desirability risk was mitigated through PRA training and the option to complete certain parts of the survey without the interviewer (e.g., sexual health and violence). 27 Validation studies of self-report CHIWOS viral load data with a subset of participants for whom health record data linkage was available have shown a high degree of validity of self-report for viral load. 66 This study is the first on the care cascade among trans WLWH published in a Canadian context, and includes the largest quantitative sample of trans WLWH in Canada, including diverse trans WLWH from three provinces. The qualitative component supported in-depth exploration of trans WLWH's experiences of engagement in the HIV care cascade and the mixed-methods design yielded results that were highly convergent.
HIV care cascade analyses are valuable in directing local programs to address issues along the care cascade. 67 While the high proportion of WLWH linked to HIV care could be regarded as a success, in a setting of universal health care such as Canada, any linkage less than 100% leaves room for improvement. Several multi-site studies have developed evidence-based strategies to increase linkage to HIV care for those newly diagnosed (e.g., ARTAS), which can be adapted to specific populations. 56,57 Interventions are also being pilot tested that address barriers to HIV care among trans WLWH, more specifically. 68 These interventions include elements common to ARTAS (e.g., case management, individual psychosocial support) as well as drop-in groups and referrals to gender-affirming HIV care. 68
Organizations seeking to support trans WLWH may consider adding components of these community-driven and theoretically informed interventions. Emerging innovative interventions may also use a combination of in-person and technology-based supports to increase engagement in HIV care among trans WLWH. 69 weCare is one such intervention that has shown to significantly reduce missed HIV care appointments and increase viral load suppression among sexual and gender minority persons. 69 These technology-based interventions may have even greater success if messages are tailored to meet the unique needs of trans WLWH (e.g., referrals to gender-affirming HIV care, address concerns/answer questions about drug–drug interactions).
Importantly, individual-level interventions will have limited success if they do not simultaneously address the structure/organization of health care and attempt to reduce multiple types of stigma, including HIV related and transphobia. Health care providers can advocate for human rights protections for trans people, such as Bill C-16 passed in 2017, which added gender identity and expression as prohibited grounds of discrimination to the Canadian Human Rights Act. Human rights protections are essential to broadly increase trans women's access to education, employment, housing, and health care. However, the findings of this study show that even with the passing of Bill C-16, stigma is pervasive and impedes access to care. Therefore, health care managers must also support providers to provide competent care to trans WLWH by enacting gender-inclusive policies (e.g., antidiscrimination policies that explicitly list gender identity and expression) and practices (e.g., gender-inclusive forms).
Opportunities for increased training in trans and HIV competency must be further researched, building on evidence of effective gender-affirming care training for medical providers. 70,71 Moreover, findings showed how trans WLWH experienced barriers common to WLWH more broadly (e.g., violence) and also experience unique barriers (e.g., concerns about drug–drug interactions) as a result of trans and HIV experience and stigmas. Further research is needed to understand the mechanisms by which socioecological factors, including those that are trans-specific (e.g., transphobia), impede women's HIV care access. Addressing barriers at multiple levels may help to achieve the 90-90-90 goals, ultimately promoting health and social justice for trans WLWH.
Footnotes
Acknowledgments
The authors would like to acknowledge the participants of the Canadian HIV Women's Sexual and Reproductive Health Cohort Study (CHIWOS). The authors thank them for trusting them with their stories. They also wish to acknowledge the administrative and recruitment support of Mina Kazemi, Angela Underhill, Rebecca Gormley, Karéne Proulx-Boucher, and the entire Peer Research Associate Team. The CHIWOS was funded by Canadian Institutes of Health Research (CIHR) Operating Grant (grant# MOP-111041), the CIHR Canadian HIV Trials Network (CTN 262), the Ontario HIV Treatment Network, and the Academic Health Science Center (AHSC) Alternative Funding Plan (AFP) Innovation Fund. This substudy was funded by a Social Science and Humanities Research Council (SSHRC) Doctoral Fellowship. MS is supported by an Ontario Trillium Scholarship (OTS). For the remaining authors, none was declared.
Author Disclosure Statement
No competing financial interests exist.