
Abstract
The systemic framework of resilience and dyadic perspective of couple coping suggests that HIV-discordant couples may show heterogeneous profiles of dyadic adjustment, shaped by contextual risks and resources. This study aimed to identify heterogeneous profiles of dyadic adjustment and thus investigate the expression of resilience among 159 heterosexual HIV-discordant couples in rural China. We hypothesized that the couples could be grouped into distinct profiles: both members showing poor well-being, both members showing good well-being, and discrepant well-being across the two members. A latent profile analysis classified the couples into three subgroups based on well-being, which was measured using the World Health Organization Well-Being Index. As expected, one subgroup, labeled Maladapted Couples (n = 58, 36.5%), reported poor well-being in both people living with HIV/AIDS (PLWHA) and the seronegative spouse. The second subgroup, labeled Resilient Couples (n = 50, 31.4%), was characterized by relatively good well-being in both partners. In the third subgroup, labeled Maladapted PLWHA and Resilient Spouses (n = 51, 32.1%), the PLWHA showed poor well-being, while the seronegative spouses demonstrated good well-being. The identified subgroups were validated against external well-being measures, including depression and self-rated health measures. Exploratory analyses identified distinct patterns of contextual risks (including HIV stigma and financial difficulties) and resource factors (including individual resources and relational resources) across the subgroups. These findings underscore the heterogeneity of adjustment among heterosexual HIV-discordant couples in rural China and suggest the potential usefulness of services tailored to specific subgroups.
Introduction
With medical advancements in antiretroviral therapy (ART), the life expectancy of people living with HIV/AIDS (PLWHA) has been largely extended. 1 Meanwhile, ART can enhance the rate of viral suppression in PLWHA, which further reduces new HIV infections between sex partners. 2 Therefore, it is estimated that the number of HIV-discordant couples will increase. 3 Compared to concordant couples, HIV-discordant couples are exposed to extra stress, including within-relationship tensions related to HIV, the sense of uncertainty, and the burden of HIV transmission management, as a result of the serodiscordancy. 4,5 Previous studies have reported poor functioning among PLWHA and their seronegative spouses, including mental health problems, 6 –8 deteriorating physical health, 9,10 and even suicidality. 11,12 Recent dyadic studies in a number of countries (e.g., the United States, Australia, and Tanzania) have shown that the couple dynamics involved in HIV coping, such as care engagement and communication, vary across couples. 5,13,14 However, little is known about the variations of couple adjustment and the expression of resilience in the discordant couple as a whole.
In China, there are deep concerns about HIV stigma and testing due to delayed epidemiological responses and inadequate HIV public education, 15,16 and the number of PLWHA has increased in recent years. 17,18 Although sexual contact and intravenous use are the major drivers of recent HIV transmission in China, 19 commercial blood donation still constituted 19% of the confirmed HIV/AIDS cases in the last decade. 20 Nearly 40,000 people were reported to be infected with HIV from commercial blood donation, with 79% residing in Henan Province. 21 This population has dealt with various adversities, including financial difficulties, HIV stigma, and limited health care services (e.g., HIV test and ART). 22,23 More than 80% of the PLWHA who were former blood/plasma donors were in a heterosexual marriage, and a considerable proportion had seronegative spouses. 21,24 Therefore, more understanding about the adjustment and resilience among heterosexual HIV-discordant couples in rural China will facilitate the promotion of well-being in this relatively large vulnerable population residing in an underdeveloped area.
Based on observations that some individuals demonstrate unexpected recovery or even thrive despite major threats to life, resilience has been defined as a process of positive adjustment under adverse conditions. 25,26 Originally capturing individuals' positive adjustments, the conceptualization of resilience was more recently expanded to embrace a systemic perspective, 27 which has two important implications for research. First, it emphasizes that resilience depends on interconnected systems at multiple levels. 28 Risks and resources involved in the resilience process are distributed across different levels, from individual characteristics to a broader sociocultural context. 27 This distribution suggests the importance of integrating risks and resources across levels in resilience research. Second, the systemic framework expands the scope of resilience research from individuals to a diversity of systems, including families, communities, and even societies, while addressing the successful adjustments to threats against the systems. 29 In the case of couple adjustment, resilience was also generalized as couple resilience or dyadic resilience. 30,31 Guided by the systemic perspective, these recent developments in resilience research among couples highlight that the couple functions as an organized system when responding to adversities. 32 –34
The resilience framework could provide new insight into HIV-discordant couples' adjustments because it emphasizes the process of thriving despite difficulties, which can inform further efforts to facilitate positive adjustment in this highly disadvantaged population. 26 Emerging studies have adopted the resilience framework to investigate better-than-expected outcomes in HIV-discordant couples. Most of these studies have identified risks and resources that are correlated with adjustment outcomes in PLWHA and seronegative spouses. For example, HIV stigma has consistently been suggested to be a salient risk factor for well-being in PLWHA and seronegative spouses. 35 –37 Financial difficulties have also been widely reported by PLWHA and partners. 38 –40 In contrast, individual and relational resources, including HIV coping efficacy, 41,42 personal resilience, 10,43 relationship satisfaction, 13,31 and family resilience, 44,45 have been found to contribute to positive adjustment in PLWHA and spouses. However, the previous research paradigm only includes risks or resources at a unitary level (e.g., only including individual resources), 46,47 instead of integrating the risks and resources across levels as suggested by the systemic framework of resilience. 27
Many previous researches have also not addressed the discordant couples' interdependence in the resilience process. Yet, accumulating evidence supports the dyadic perspective of couple coping with chronic disease, showing that patients and spouses are mutually affected and that the coping dynamics within couples can generate different adjustment outcomes. 48 Theoretical models regarding couple coping (e.g., the Systemic-Transactional Model and the Coping Congruence Model) 33,49 highlighted interdependence within the couple in the coping process and adaptation, 50 which is consistent with recent ideas built upon the systemic framework that the couple functions as an organized system in the resilience process. 27,30,31 Such interdependence in couple adjustment could be particularly significant in China's HIV-discordant couples because the traditional Chinese marital philosophy emphasizes the responsibility to care for each other when in need. 51 Social isolation due to HIV stigma renders supports within the PLWHA-spouse dyad even more crucial in disease coping, 52,53 magnifying the mutuality of the discordant couple. However, most of the existing studies of HIV-discordant couples, especially the quantitative ones, only included the PLWHA or their seronegative spouses. 38,54 A few studies have included both members of the discordant couple, but have examined how risks and resources contribute to individual adjustment outcomes instead of considering the interdependence and seeking to understand the couple as a whole. 6,7 These studies investigated the resilience of the PLWHA and seronegative spouses separately, instead of addressing the resilience of the HIV-discordant couple.
To further the understanding of resilience in HIV-discordant couples, it could also be helpful to adopt the person-centered perspective in research. Previous studies have been mainly guided by the variable-centered approach, clarifying relationships among variables and teasing out contributors to specific adjustment outcomes. 9,55,56 These studies have focused on variables instead of the whole individual or system. The person-centered approach investigates individual patterns of adjustment that are developed naturally over time and grounded in lived experience. 57 For example, a classic person-centered approach paradigm used to study resilience identifies and compares adaptive and maladaptive subgroups of individuals from vulnerable samples. 58 By addressing the heterogeneity of individuals' adjustment to adversity, such an approach captures the holistic expression of resilience, which is shaped by individual lived experience over time. 57,59 The person-centered perspective can provide additional information about the holistic patterns of adjustment and underlying configured characteristics beyond the variable-centered perspective. 60 Although the scope of resilience research has expanded to include couples, previous studies have seldom investigated heterogeneous patterns of dyadic adjustment and thus have not captured the naturally occurring expression of resilience in couples. It is still unknown whether HIV-discordant couples demonstrate heterogeneous adjustment outcomes and how resilience is dyadically manifested in such couples.
Previous research has suggested complicated heterogeneity of dyadic adjustment among HIV-discordant couples. Although the dyadic perspective of couple coping emphasizes interdependence in couple adjustment, it does not assert that the patient and the spouse are equally affected by the illness. 61 Instead, the engagement in the chronic disease can be discrepant between the patient and the spouse because it is a product of complex integration among multiple factors, including the individual appraisal of the illness, relationship identity, and couple communication. 32,62 As such, prior qualitative findings have reported discrepant engagement in HIV between the PLWHA and seronegative spouses in some discordant couples. 63 –65 For example, Persson discovered that several discordant couples considered HIV management as solely the responsibility of PLWHA rather than a shared one, with the seronegative spouse demonstrating low involvement in daily care. 5 Although researchers implicated that such a discrepant coping style within the HIV-discordant couple might be shaped by distinct contextual factors and could lead to various outcomes, 5,13,66 whether such a discrepant pattern exists in dyadic adjustment of discordant couples and the other configured characteristics of these couples have yet to be investigated.
According to the systemic framework of resilience and the dyadic perspective of couple coping, the HIV-discordant couple is likely to function as a unit instead of two separate individuals during the resilience process, within the interplays of risks and resources across levels. 27,31,50 However, prior research has seldom integrated the risks and resources across different levels or has considered the couple as a unit when investigating the resilience process of discordant couples. In addition, as previous resilience studies dominantly adopted the variable-centered approach, the holistic patterns of dyadic adjustment, and expressions of resilience among HIV-discordant couples remain unclear. We thus applied the person-centered approach to examine heterosexual HIV-discordant couples by treating the couple as a unit. Using this design, we sought to capture the heterogeneity of their dyadic adjustment and investigate the underlying configured characteristics of risks and resources. We aimed to (1) employ Latent Profile Analysis (LPA) to identify heterogeneous subgroups based on the well-being of PLWHA and their seronegative spouses among a sample of heterosexual HIV-discordant couples in rural China, (2) validate the obtained subgroups against external physical and mental well-being measures, and (3) investigate differences in contextual risks and resources across subgroups.
We expected distinct heterogeneous profiles of dyadic adjustment would exist among the heterosexual HIV-discordant couples. As suggested by previous work, the enormous stress resulting from HIV can compromise the adjustment of HIV-discordant couples. 6 –12 Therefore, a sizeable proportion of discordant couples was expected to demonstrate poor well-being in both PLWHA and seronegative spouses. Consistent with the systemic framework of resilience, 27 such a maladapted subgroup would report relatively higher levels of risks and lower levels of individual and relational resources. By contrast, a second subgroup of discordant couples was hypothesized to show good well-being in both the PLWHA and seronegative spouses, despite the challenge of HIV, as suggested by previous resilience research in populations of adversity-exposed individuals that show some individuals achieve positive adjustment. 60,67 This subgroup would be configured with lower risk levels and greater individual and relational resources. Based on previous findings showing discrepant engagement in HIV care within the discordant couple, 5,13 we expected to identify a third profile of discrepant dyadic adjustment among the HIV-discordant couples. In this profile, the PLWHA would report poor well-being, while the seronegative spouses would report good well-being.
Methods
Participants
This study was conducted in five randomly selected communities from a pool of villages that have an HIV prevalence of greater than 10% in Henan Province, China. A large number of people there were infected with HIV through a commercial blood donation. 22 A total of 159 heterosexual HIV-discordant couples were recruited to participate. The inclusion criteria were (1) only one member of the couple was infected with HIV and (2) being married for more than 5 years. There were no eligibility criteria related to gender, age, linguistic ability, or intimate partner violence.
Procedure
Due to the low education levels of the participants, trained local health service providers conducted face-to-face structural interviews with participants. The interviews were conducted separately with each partner and the interviewee's partner was asked to leave the interview room during the interview. The participants provided informed consent to participate and received compensation for their time spent on the survey (60 CNY for each participant, approximately the equivalent of 10 USD). Ethical approval was obtained from the City University of Hong Kong.
Measures
Clustering measure
Well-being was measured using the World Health Organization Well-Being Index (WHO-5), and a mean score that was below 2.6 indicated poor well-being. 68 This five-item measurement has been applied to Chinese PLWHA in our previous study. 69 Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.88, seronegative spouses: α = 0.91).
External measures
Self-rated physical health was measured using eight items from the brief version of the WHO Quality of Life instrument (WHOQOL-BREF). The Chinese version was validated with good psychometric properties. 70 Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.87, seronegative spouses: α = 0.88).
Depressive symptoms were measured using the nine-item Patient Health Questionnaire 9 (PHQ-9). 71 The Chinese version of the PHQ-9 showed good psychometric properties in Chinese HIV-serodiscordant couples in our previous study. 69 Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.92, seronegative spouses: α = 0.92).
Financial difficulties were measured with four items developed by Gorgievski-Duijvesteijn et al. 72 The Chinese version was generated using the translations and back-translations procedure. Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.80, seronegative spouses: α = 0.81).
PLWHA's HIV stigma consisted of three aspects of stigma experience, including social isolation, the perception of others' fear regarding exaggerated contagiousness, and self-stigma. These three aspects were measured with the HIV/AIDS Stigma Instrument: (1) the five-item Social Isolation subscale (e.g., “People avoided me”), (2) the six-item Fear of Contagion subscale (e.g., “I was made to eat alone”), and (3) the five-item Negative Self-Perception subscale (e.g., “I felt that I did not deserve to live”). 73 The Chinese versions of these three measures were generated using the translations and back-translations procedure. Only the PLWHA completed these measures because they address the stigma experience of living with HIV. These measures demonstrated good internal reliability among the PLWHA (α = 0.94 for the Social Isolation subscale, 0.79 for the Fear of Contagion subscale, and 0.83 for the Negative Self-Perception subscale).
Seronegative spouses' courtesy stigma was measured with nine items developed by Wight et al. 74 to assess the stigmatic experience of being the spouse of a PLWHA. The Chinese version has been used in our previous study. 69 This measure showed high internal reliability among the seronegative spouses (α = 0.91).
HIV coping efficacy was measured with five items developed by Hou. 75 The Chinese version was generated by using the translations and back-translations procedure. Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.88, seronegative spouses: α = 0.86).
Personal resilience was measured with the 25-item Connor–Davidson Resilience Scale (CD-RISC). 76 The Chinese version of the CD-RISC has been previously used among Chinese PLWHA. 77 Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.89, seronegative spouses: α = 0.85).
Marital satisfaction was measured with the seven-item Relationship Assessment Scale. 78 The Chinese version was generated using the translations and back-translations procedure. Both the PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.93, seronegative spouses: α = 0.93).
Family resilience was measured with the nine-item Family Resilience Measure. 79 The Chinese version has shown good psychometric properties in previous research. 80 Both PLWHA and seronegative spouses completed this measure (PLWHA: α = 0.81, seronegative spouses: α = 0.80).
Statistical analysis
LPA based on the well-being scores of both the PLWHA and seronegative spouses was used to identify the subsets of HIV-discordant couples. LPA is a data-driven statistical protocol that identifies clusters among individuals through Maximum Likelihood estimation. 81 To identify the optimal number of classes, we used the following statistical criteria: Lo–Mendell–Rubin Likelihood Ratio Tests (LMR), Bootstrap Likelihood Ratio Tests (BLRT), Bayesian information criterion (BIC), sample-adjusted BIC (aBIC), Akaike information criterion (AIC), and entropy value. Significant values of LMR and BLRT indicate that the fitness of the k model improved compared to the (k-1) model. 82 Lower BIC and AIC values indicate a better trade-off between parsimony and fitness of the model. 83 Greater entropy values indicate better classification, with an entropy value greater than 0.80 showing a relatively high accuracy of classification. 84 We used Mplus7 statistical software to conduct the LPA.
To validate the identified subgroups, we compared external adjustment measures, including self-rated physical health and depressive symptoms across the subgroups. To further investigate the configured patterns of risks and resources, we compared the identified subgroups based on risks (PLWHA: financial difficulties, social isolation, exaggerated contagiousness, and self-stigma; seronegative spouses: financial difficulties and courtesy stigma) and resources (for PLWHA and seronegative spouses, separately: HIV coping efficacy, personal resilience, marital satisfaction, and family resilience). The subgroup comparisons were conducted using Multi-variate Analyses of Variance (MANOVA) in SPSS. Four separate MANOVAs were conducted for demographic characteristics (which included the duration of HIV diagnosis), adjustment measures, risk measures, and resource measures. The MANOVAs for adjustment measures, risk measures, and resource measures were conducted after controlling for covariates of demographic characteristics and the duration of HIV diagnosis. A significant F-value indicated a meaningful difference across the subgroups, with a partial η 2 around 0.01 suggesting a small effect size, a partial η 2 around 0.09 suggesting a medium effect size, and a partial η 2 larger than 0.25 indicating a large effect size. 85 The post-hoc tests were conducted using a Bonferroni correction.
Results
Table 1 shows the participant demographic characteristics and duration of HIV diagnosis. The heterosexual HIV-discordant couples included in this study were mostly middle aged with relatively low education and income levels. In this sample, all discordant couples, except two, reported a longer marriage duration than the HIV diagnosis duration.
Demographic and HIV Characteristics with Subgroup Comparison
Scores are displayed in mean ± SD or %.
p < 0.05; ** p < 0.01.
MC, maladapted couples; MPRS, maladapted PLWHA and resilient spouses; PLWHA, people living with HIV/AIDS; RC, resilient couples; SD, standard deviation.
Identifying subgroups
Table 2 shows the results of the LPA. The three-class solution fit the data significantly better than the two-class solution (LMR <0.05, BLRT <0.01) and demonstrated an entropy value greater than 0.90. The four-class solution showed higher BIC than the three-class model and identified a subgroup with a very small proportion (n = 4, 3%). Therefore, the model with three classes was selected for further analysis.
Results of Latent Profile Analysis
aBIC, sample-adjusted BIC; AIC, Akaike information criterion; BIC, Bayesian information criterion; BLRT, Bootstrap Likelihood Ratio Tests; LMR, Lo–Mendell–Rubin Likelihood Ratio Tests.
The three-group solution of LPA is shown in Table 3 and is depicted graphically with standardized scores in Fig. 1. Subgroup 1, consisting 36.5% of couples (n = 58), was labeled the Maladapted Couples subgroup because both the PLWHA [M = 1.39, standard deviation (SD) = 0.46] and seronegative spouses (M = 2.22, SD = 0.53) demonstrated low levels of well-being (below the poor well-being cutoff score of 2.6 in WHO-5). 68 Subgroup 2 (n = 50, 31.4%) was labeled as the Resilient Couples subgroup because both PLWHA (M = 3.35, SD = 0.49) and seronegative spouses (M = 3.38, SD = 0.67) showed higher levels of well-being than the poor well-being cutoff of the WHO-5. Subgroup 3 (n = 51, 32.1%) was labeled as the Maladapted PLWHA and Resilient Spouses subgroup because PLWHA demonstrated poor well-being (M = 1.36, SD = 0.38), while seronegative spouses showed relatively high levels of well-being (M = 4.36, SD = 0.42).

Patterns of adjustment measures across subgroups.
Subgroup Comparison in Adjustment Measures
Scores are displayed in mean ± SD.
p < 0.01.
MC, maladapted couples; MPRS, maladapted PLWHA and resilient spouses; PLWHA, people living with HIV/AIDS; RC, resilient couples; SD, standard deviation.
The subgroup differences in demographic characteristics and duration of HIV diagnosis (MANOVA results) are also displayed in Table 1. There were main effects for groups [Wilks' lambda = 0.71, F (14, 296) = 3.89, p < 0.01]. The Maladapted Couples subgroup was significantly older than the Resilient Couples subgroup and had been married longer than the couples in the other two subgroups. Compared to the other two subgroups, the couples in the Maladapted PLWHA and Resilient Spouses subgroup had significantly poorer education levels, lower per capita income, and a shorter duration of HIV diagnosis.
Validating subgroups
Table 3 shows the comparisons of the adjustment measures (well-being, self-rated health, and depressive symptoms) across the identified subgroups (MANOVA results). The differences across the subgroups on adjustment measures are also shown with standardized scores in Fig. 1. There were main effects for groups [Wilks' lambda = 0.07, F (12, 248) = 58.43, p < 0.01]. Among the three subgroups, the PLWHA and seronegative spouses in the Maladapted Couples subgroup showed relatively low levels of self-rated health and high levels of depressive symptoms. The PLWHA in the Resilient Couples subgroup had the highest levels of self-rated health and lowest levels of depressive symptoms. The seronegative spouses in this subgroup also scored relatively high in self-rated health and similarly low in depressive symptoms. By contrast, the seronegative spouses in the Maladapted PLWHA and Resilient Spouses subgroup had a higher level of self-rated health and a lower level of depressive symptoms. The PLWHA in this subgroup demonstrated low levels of self-rated health and high levels of depressive symptoms, similar to those in the Maladapted Couples subgroup. The subgroup differences in the external adjustment measures of physical well-being (self-rated health) and mental well-being (depressive symptoms) were consistent with the difference in the clustering measure (WHO-5 scores), which supported the validity of the three-group solution.
Comparing subgroups in risk and resource measures
The comparison of subgroups based on risk measures is shown in Table 4 (MANOVA results) and the subgroup differences (Z-scores) are depicted in Fig. 2. There were main effects for all groups [Wilks' lambda = 0.48, F (12, 266) = 9.95, p < 0.01]. Members of the Resilient Couples subgroup showed lower levels of financial difficulties and stigma indicators. In contrast, participants in the Maladapted Couples subgroup scored relatively high in financial difficulties and stigma indicators. The couples in the Maladapted PLWHA and Resilient Spouses subgroup reported the highest level of financial difficulties. The PLWHA reported a stronger stigma experience in exaggerated contagiousness and self-stigma than those in the Resilient Couples subgroup; however, the seronegative spouses in this group reported the lowest level of courtesy stigma among the three groups.
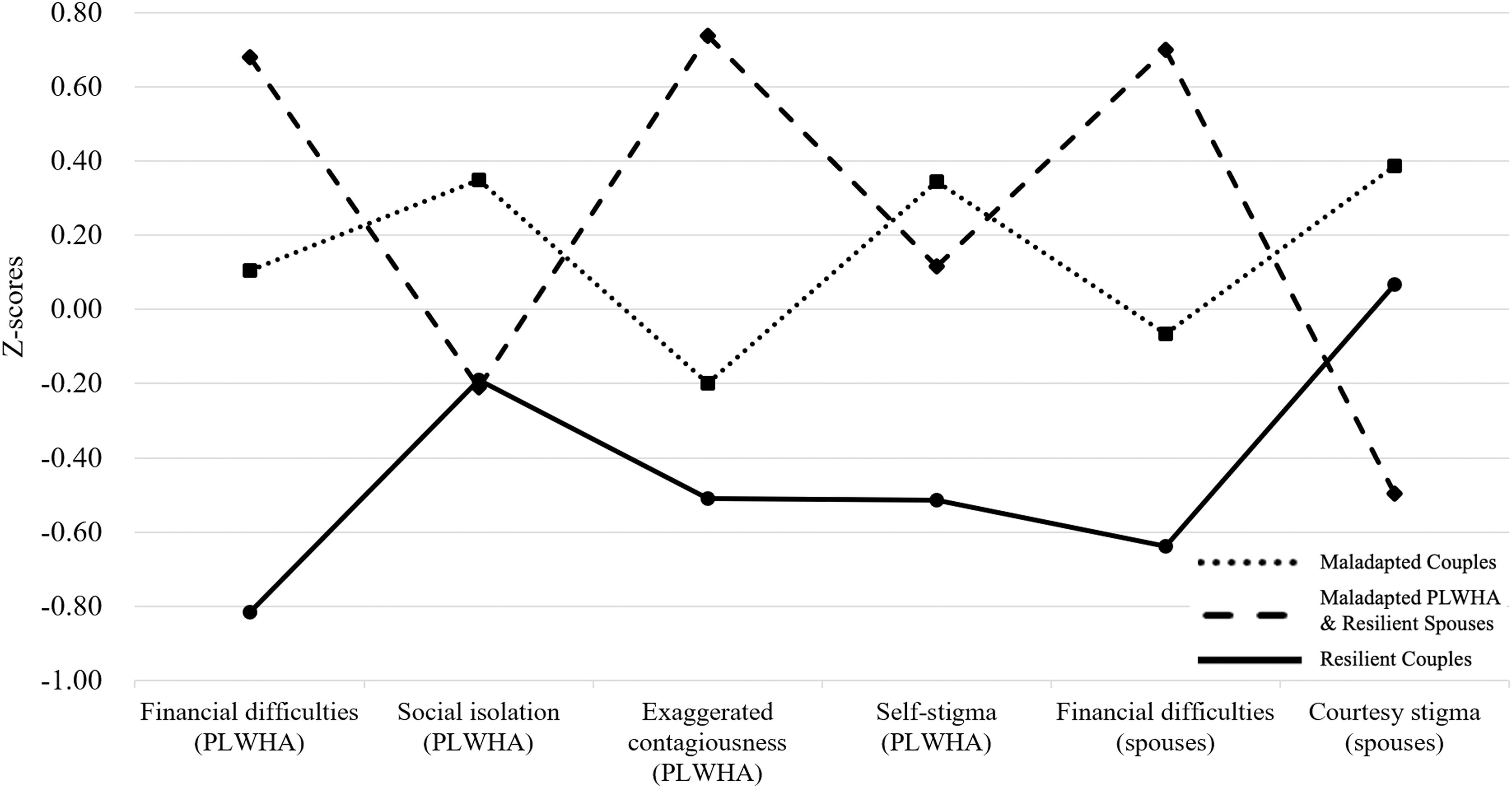
Patterns of risk measures across subgroups.
Subgroup Comparison in Risk Measures
Scores are displayed in mean ± SD.
p < 0.05; ** p < 0.01.
MC, maladapted couples; MPRS, maladapted PLWHA and resilient spouses; PLWHA, people living with HIV/AIDS; RC, resilient couples; SD, standard deviation.
The MANOVA findings on the resource measures are presented in Table 5, and the subgroup differences (Z-scores) are shown in Fig. 3. There were main effects for all groups [Wilks' lambda = 0.39, F (16, 218) = 8.04, p < 0.01]. The couples in the Maladapted Couples subgroup had relatively low levels of resources among the three subgroups. In contrast, the Resilient Couples subgroup had relatively high levels of resources across the different measures. Interestingly, both the PLWHA and seronegative spouses in the Maladapted PLWHA and Resilient Spouses subgroup had high levels of personal resilience, marital satisfaction, and family resilience, but they scored lower on HIV coping efficacy.
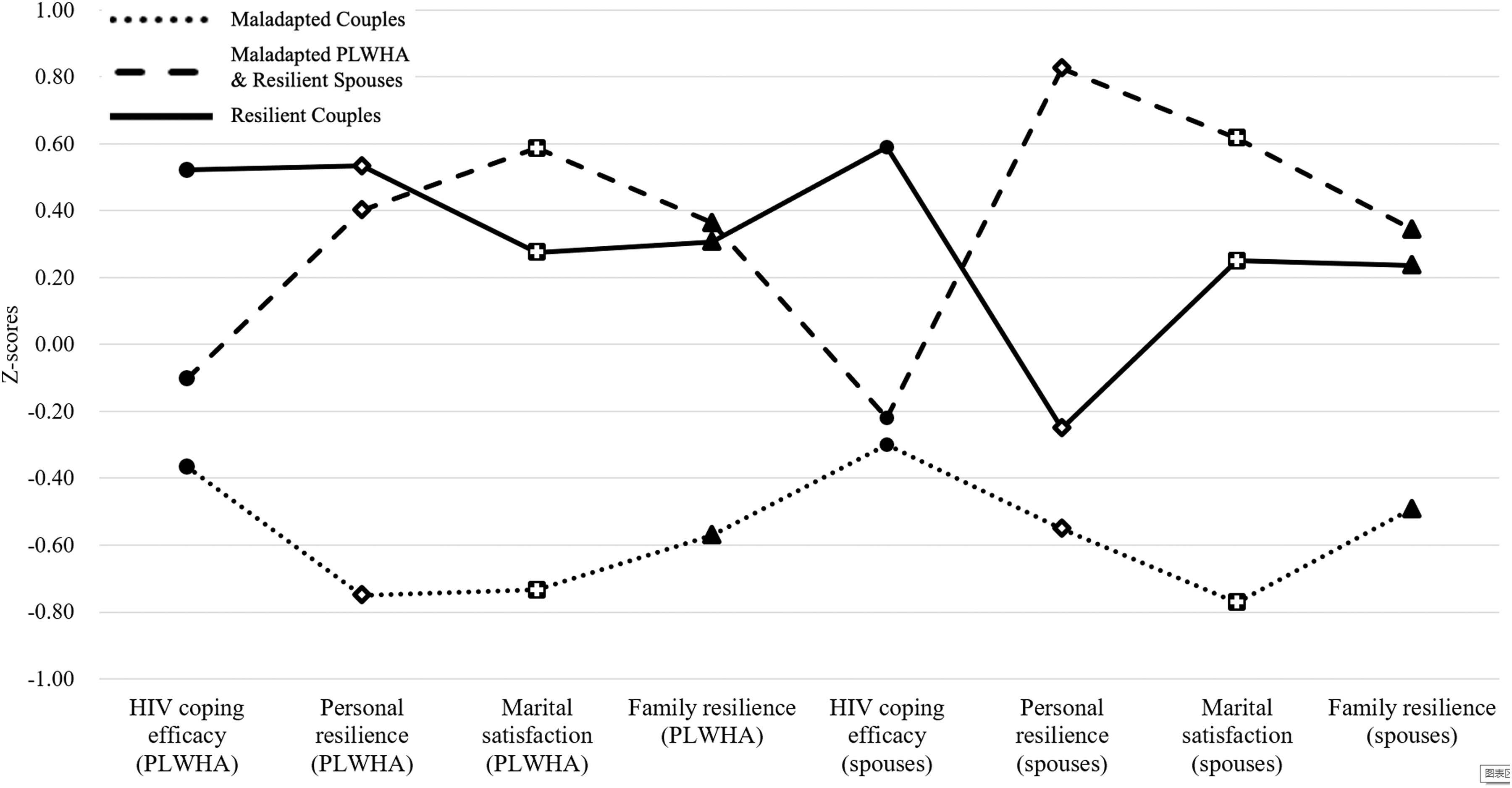
Patterns of resource measures across subgroups.
Subgroup Comparison in Resource Measures
Scores are displayed in mean ± SD.
p < 0.01.
MC, maladapted couples; MPRS, maladapted PLWHA and resilient spouses; PLWHA, people living with HIV/AIDS; RC, resilient couples; SD, standard deviation.
Discussion
Built on the systemic framework of resilience and dyadic perspective of couple coping, 27,32,50,65 this study conceptualized the discordant couple as a functioning totality in HIV coping. We also investigated the heterogeneity of dyadic adjustment, while examining resilience in HIV-discordant couples with regard to contextual risks and resources. An LPA identified three distinct adjustment patterns within heterosexual HIV-discordant couples in rural China: Maladapted Couples, Resilient Couples, and Maladapted PLWHA and Resilient Spouses. This subgrouping was supported by validation analysis based on external, physical, and mental well-being measures. The comparison of the subgroups based on contextual risks and resources identified different characteristics across the patterns of dyadic adjustment. We used the person-centered approach to investigate the dyadic adjustment of couples by treating the couple as the unit of analysis. Our findings capture holistic dyadic adjustment patterns and corresponding configured contextual risks and resources among heterosexual HIV-discordant couples in rural China.
Heterogeneity of dyadic adjustment among heterosexual HIV-discordant couples
This study found three distinct profiles of dyadic adjustment in heterosexual HIV-discordant couples. Consistent with previous findings about the poor functioning of discordant couples, 6,9,12 the largest subgroup of couples, the Maladapted Couples (37%), had poor adjustment in both the PLWHA and seronegative spouses. Nearly one-third of the couples (32%) reported poor adjustment in the PLWHA, but positive adjustment in the seronegative spouses, and this group was labeled Maladapted PLWHA and Resilient Spouses. A striking proportion of couples (31%) was classified as Resilient Couples because they reported positive adjustment in both the PLWHA and seronegative spouses. The results of the validation analyses in external adjustment measures supported this solution of the LPA, with the identified subgroups showing patterns of self-rated health and depressive symptoms that were consistent with the clustering of well-being scores. The adjustment heterogeneity among HIV-discordant couples has been neglected because previous dyadic studies have mainly used the variable-centered approach in data analysis to address relationships among variables (e.g., the Actor-Partner Interdependence Model) rather than distinguishing different subgroups. 37,86
The distinction between Maladapted Couples and Resilient Couples is consistent with our hypotheses based on the resilience framework. Decades of resilience research have suggested that individuals show large variability in adjustment to adversity, with some falling apart, while others thrive. 67,87 Our findings expand such variability to couples' dyadic adjustment, which supports recent developments in the systemic framework of resilience and the dyadic perspective of couple coping that the couple adjust to the chronic disease as an organized system. 31,61 Although a large proportion of heterosexual discordant couples reported compromised functioning, others demonstrated better-than-expected outcomes in both partners, suggesting that HIV-discordant couples have the potential to achieve positive adjustment as a unit despite the challenges.
As hypothesized, a proportion of the couples showed a discrepant dyadic adjustment pattern in which the PLWHA were maladapted and seronegative spouses reported resilient outcomes. Such a pattern has been overlooked in previous studies. 55,88,89 This discrepant adjustment pattern corresponds with previous qualitative findings that some HIV-discordant couples with disengaged seronegative spouses conceptualized HIV coping as the issue of the PLWHA alone rather than as a challenge shared by both partners. 5,63 Interestingly, these couples reported that their relationship quality was not compromised by such discrepant engagement in HIV, 13,60 which is consistent with the relatively high levels of marital satisfaction and family resilience reported by the Maladapted PLWHA and Resilient Spouses in this study. Future studies should investigate the cognitive and behavioral characteristics of the Maladapted PLWHA and Resilient Spouses.
Contextual characteristics across dyadic adjustment profiles
The three dyadic adjustment profiles of the heterosexual HIV-discordant couples had distinct patterns of contextual risks and resources. As expected, the Maladapted Couples consistently reported relatively high levels of risks (financial difficulties and HIV stigma) and low levels of individual (HIV coping efficacy and personal resilience) and relational (marital satisfaction and family resilience) resources in both the PLWHA and seronegative spouses. In contrast, both partners of the Resilient Couples demonstrated relatively low levels of risks, but high levels of resources. The multi-faceted differences of contextual characteristics between the Maladapted Couples and the Resilient Couples are consistent with notions of the systemic framework of resilience in that the resilience process involves the interplays of multiple systems. 27 Therefore, a unitary factor or a unitary level of factors cannot determine a holistic resilience outcome in heterosexual HIV-discordant couples. Instead, the resilience of the couple is characterized by lower contextual risks and higher contextual resources at both the individual and relational levels in both partners. 90
The Maladapted PLWHA and Resilient Spouses subgroup demonstrated a unique pattern of risks and resources in contrast to the other two subgroups. This subgroup was characterized by the highest levels of financial difficulties and discrepant stigma experience within the couple (strong exaggerated contagiousness and self-stigma in PLWHA, and weak courtesy stigma in seronegative spouses) and had relatively high levels of most resources, except HIV coping efficacy. Previous studies have found that some PLWHA in rural China reported financial difficulties as the major barrier to seeking health service, despite subsidies from the government. 40,91 The unaffordability of medical care resulting from financial difficulties, together with the lack of HIV coping efficacy, could negatively affect the PLWHA in particular, as their well-being is directly threatened by HIV in contrast to the seronegative spouse. The discrepant stigma experience could also account for the discrepant adjustment outcomes within the discordant couple because experiencing HIV stigma strongly undermines successful adjustment. 35,92 The particularly high level of exaggerated contagiousness reported by PLWHA in this subgroup also merits attention. Exaggerated contagiousness describes a stigmatic experience in which others show their fear of direct contact with the PLWHA, reflecting others' irrational fear about HIV or erroneous beliefs about the transmission (e.g., refusal to eat together and refusal to share utensils). 73 Such an experience is prevalent within the family as it is the context in which most of these direct contacts take place. 92,93 Discrimination from family members can bring particular distress to the PLWHA and even break optimal communication and bonding within the family, 36 which may further contribute to the discrepant adjustment pattern that the PLWHA is maladapted, while the seronegative spouse is resilient.
Interestingly, we found no significant difference in sex distributions across profiles of heterosexual discordant couples even though some previous studies have reported sex difference in the experience related to a heterosexual HIV-discordant relationship. 4,54,94 Among heterosexual discordant couples, female PLWHA have reported higher levels of depression than male PLWHA, with their seronegative partners reporting similar levels of depression. 89 These previous studies suggest that sex matters in individual experiences. However, we found that sex had no effect on the adjustment profiles in heterosexual discordant couples. This inconsistency suggests that although sex might cause differences in individual adjustment outcomes, it might not alter the holistic patterns of dyadic adjustment in heterosexual discordant couples. This finding highlights how using the person-centered approach and considering the discordant couple as a whole can provide additional information beyond the traditional variable-centered approach.
Implications and limitations
Our findings have important implications for the promotion of resilience in heterosexual HIV-discordant couples. The heterogeneity of dyadic adjustment patterns we found highlights the significance of targeted interventions for those who are not Resilient Couples. Although neither the Maladapted Couples nor Maladapted PLWHA and Resilient Spouses subgroups reported optimal adjustment outcomes in which both partners experienced good well-being, they nonetheless endorsed distinct patterns of contextual characteristics that could inform different directions for interventions. The Maladapted Couples demonstrated multi-faceted disadvantages in risks and resources when compared to the Resilient Couples, suggesting that resilience promotion in this subgroup might require holistic interventions that address contextual risks and resources at multiple levels in both partners. The salient stigma experience of the PLWHA in the Maladapted PLWHA and Resilient Spouses highlights the importance of targeted stigma reduction. The particularly high level of exaggerated contagiousness experienced by the PLWHA suggests that they and their family members might need further education about HIV transmission.
A number of studies have developed psychosocial interventions involving both the PLWHA and seronegative spouses to prevent HIV transmission and facilitate HIV management, and most of these studies have reported good efficacy. 3,95 However, only a few dyadic interventions have targeted the well-being of the discordant couple, and these interventions had small sample sizes and mixed findings of efficacy. 96,97 Our findings strongly suggest that future studies should focus on dyadic interventions that target the well-being of discordant couples and consider heterogeneity in this population.
Notwithstanding the importance of its findings, this study has some limitations. First, the LPA results could have been highly influenced by the selection of indicators and samples. 60 The data-driven subgrouping in this study has yet to be replicated in other samples with alternative indicators. Second, due to the difficulty of concurrently recruiting PLWHA and their seronegative spouses, we only managed to include 159 discordant couples. Although this sample size is acceptable for LPA estimations, 98 it is a relatively limited sample and could undermine the generalizability of our person-centered findings. Third, our findings were obtained only from heterosexual HIV-discordant couples. The variations of adjustment patterns among couples with different gender compositions (e.g., male couples) deserve replications because such couples face distinct stressors (e.g., homosexual stigma, the lack of legal protection of marriage) compared to heterosexual couples. 99 Fourth, the PLWHA in this study were infected through commercial blood donations. Future studies are needed to generalize our findings to the PLWHA who were infected in a different manner. Finally, resilience is a dynamic process that operates in contingent trajectories over time, 67 but these cross-sectional findings can only capture static dyadic adjustment profiles and the corresponding characteristics of each profile. Therefore, the relationships among the profiles and characteristics are correlational in nature, and caution should be used when drawing causal conclusions without evidence obtained from experimental studies. Future longitudinal studies would be helpful to depict variations and mechanisms of the long-term adjustment process of HIV-discordant couples.
By integrating PLWHA and seronegative spouses as a unit in HIV coping and applying the person-centered perspective to couple adjustment, this study offers new evidence into the resilience of couples. We found robust variations in the adjustment patterns of heterosexual HIV-discordant couples in rural China, including Maladapted Couples, Resilient Couples, and Maladapted PLWHA and Resilient Spouses. We also identified distinct configured patterns of contextual risks and resources for each subgroup. Our findings highlight the importance of investigating the heterogeneity of couple adjustment in future work. The findings from this study also suggest the need for targeted resilience promotion strategies for vulnerable subgroups of heterosexual HIV-discordant couples.
Footnotes
Acknowledgments
The work described in this article was supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project No. CityU 11600617). The sponsor had no further role in study design, in the collection, analysis, and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.