
Abstract
We conducted a cross-sectional study of 148 HIV+ on HIV antiretroviral therapy and 149 HIV− adults in Mbarara, Uganda, to estimate the association between HIV infection and homeostasis model assessment of insulin resistance (HOMA-IR) using multivariable regression analysis. In addition, we evaluated whether intestinal fatty acid-binding protein (I-FABP), monocyte activation markers soluble (s)CD14 and sCD163, and proinflammatory cytokine interleukin 6 (IL-6) mediated this association. HOMA-IR was greater among HIV+ than HIV− adults [median (interquartile range): 1.3 (0.7–2.5) vs. 0.9 (0.5–2.4); p = 0.008]. In models adjusted for sociodemographic variables, diet, hypertension, and smoking history, HIV infection was associated with 37% [95% confidence intervals (95% CIs): 5–77] greater HOMA-IR compared with HIV− participants. The magnitude of association was greater when I-FABP was included as a covariate although the additive effect was modest (40% CI: 8–82). By contrast adding sCD14 to the model was associated with greater HOMA-IR (59%; 95% CI: 21–109) among HIV+ participants compared with HIV− participants. Among HIV+ participants, greater CD4 nadir was non-significantly associated with greater HOMA-IR (22%; 95% CI: −2 to 52). Each 5-unit increase in body mass index (BMI; 49% greater HOMA-IR; 95% CI: 18–87) and female sex (71%; 95% CI: 17–150) remained associated in adjusted models. In this study of mainly normal-weight Ugandan adults, HIV infection, female sex, and greater BMI were all associated with greater insulin resistance (IR). This association was strengthened modestly after adjustment for sCD14, suggesting possible distinct immune pathways to IR that are independent of HIV or related to inflammatory changes occurring on HIV treatment.
Introduction
Sub-Saharan Africa (SSA) has the highest burden of HIV in the world; more than 25.5 million Africans are living with HIV in the region, including nearly 15 million on antiretroviral therapy (ART). 1 Expanding use of ART has led to a notable decline in HIV-associated morbidity and death in SSA. 2 Nonetheless, people living with HIV in SSA continue to experience excess morbidity and mortality related to non-communicable diseases. 3,4 Despite a paucity of data describing the burden of diabetes among people with HIV (PWH), it is estimated that anywhere between 19% and 47% of those on ART may have prediabetes. 5,6 The extent to which ART is a primary driver of increased diabetes risk in SSA is less clear. 6,7 Nonetheless, given that around 5–10% of persons with prediabetes will progress annually to Type 2 Diabetes Mellitus (DM) in the absence of biomedical interventions, 8 the incidence of DM among PWH is likely to increase as these individuals at highest risk for DM are living longer on ART. 9
Current evidence, predominantly derived from US and European cohorts, indicates that increased DM risk in PWH reflects a mix of effects of HIV and chronic inflammation, as well as potentially disproportionate contributions of obesity and aging among PWH compared with the general population. 10,11 Recent data from SSA have also highlighted that exposure to older-generation thymidine analogs or protease inhibitors (PI), malnutrition at ART initiation, and failure to gain fat mass on treatment may be important determinants of DM risk in the region. 5 Further, Intestinal Fatty Acid-Binding Protein (I-FABP), a systemic marker of gut epithelial cell death, soluble CD14 (sCD14), a marker of monocyte activation, and a coreceptor for lipopolysaccharide (LPS), 12,13 and soluble CD163 (sCD163), another marker of monocyte/macrophage activation, 14 have all been associated with DM risk in HIV-seronegative persons. 15 –18 Determining if monocyte activation and inflammation, related to microbial translocation or independent of it, are associated with disorders of glucose metabolism in PWH in SSA has yet to be established. Nonetheless, establishing the determinants of DM in PWH in the region has important clinical implications and is an important research priority.
In this study, we hypothesized that HIV infection is associated with greater insulin resistance (IR) in East Africa and that intestinal epithelial damage and consequent monocyte/macrophage activation are key drivers of the association. Further, we sought to estimate the magnitude of IR, an estimate of prediabetes, 19 among PWH on long-term suppressive ART, compared with age and sex-matched, uninfected, and population-based controls in southwestern Uganda.
Methods
Study population
The Ugandan Non-Communicable Diseases and Aging Cohort (UGANDAC) Study (NCT02445079), is a prospective observational cohort study, which has been described in detail previously. 20,21 The study is comprised of ambulatory ART-experienced, PWH, and HIV-seronegative individuals enrolled from a cluster of villages ∼20 km from the clinic. PWH were enrolled from Mbarara Regional Referral Hospital HIV clinic. Eligibility criteria included (1) being actively engaged in HIV care; (2) age >40 years; and (3) on ART for a minimum of 3 years. Age- and sex-matched HIV-uninfected participants were recruited from the same region served by the HIV clinic 22 and all underwent routine confirmatory HIV testing. Participants are seen annually to complete questionnaires, and for blood collection. 23 We excluded four PWH and seven HIV-seronegative participants who had confirmed DM (defined as having a confirmed diagnosis of DM or report of anti-DM medication or fasting glucose values >126 mg/dL on two consecutive visits) based on the rationale that DM is a result, not a cause of IR. This left 297 participants in the primary cross-sectional analysis, although we did include all participants in an additional sensitivity analysis to determine if including those with diabetes influenced associations.
Measurement of markers of microbial translocation and inflammation
Using plasma blood samples collected from study participants at annual visits and stored at −80°C, we tested specimens for four biomarkers: (1) I-FABP (R&D Systems, Minneapolis MN); (2) sCD14 (R&D Systems); (3) sCD163 (R&D Systems); (4) and interleukin 6 (IL-6; MesoScale Discovery, Rockville, MD). Assays were performed in accordance with manufacturers' protocols. All biomarker tests were performed at the Laboratory for Clinical Biochemistry at the University of Vermont.
Outcomes
Our primary outcome of interest was IR, quantified using the Homeostasis Model Assessment (HOMA-IR) defined as fasting insulin (μU/mL) × glucose (mg/dL)/405. 24 Fasting specimens for glucose determination were collected in standard serum separator tubes. Blood serum for insulin determination was obtained at the same time, and all specimens were stored at −70°C until the day of assay. Serum glucose was measured using the hexokinase method, and insulin was measured using the IMMULITE 2000 assay (LabCorp, Cambridge, MA).
Covariates
Candidate covariates included demographic characteristics (i.e., age, sex, and HIV status); comorbidities (hypertension); anthropometric measures [i.e., waist circumference, weight, height, and body mass index (BMI)], laboratory parameters, (serum albumin); and lifestyle factors [i.e., smoking (current vs. exsmoker vs. none) and self-reported diet (days per week of vegetable consumption)] were all taken from the date of first study visit, or next follow-up visit if baseline data were missing. Socioeconomic status was derived from a principal components analysis using a series of 24 indicators of asset ownership using methods described previously by Filmer and Pritchett. 25 HIV-seronegative participants undergo annual HIV testing before study visits to confirm their status. Pre-ART, baseline HIV viral load, and current and nadir CD4+ T cell count values were abstracted from electronic records at the Mbarara Regional Referral Hospital HIV clinic.
Statistical analysis
We first compared sociodemographic and clinical characteristics by HIV serostatus and sex. Because HOMA-IR, I-FABP, sCD14, and sCD163 were found to have right skewed distributions, they were log transformed. We fitted multivariable linear regression models specifying HOMA-IR as the dependent variable and HIV infection as the primary covariate of interest. Estimates were adjusted for sex, diet, history of past smoking, socioeconomic status, BMI, and comorbid hypertension. To determine the extent to which intestinal epithelial damage mediated the association between HOMA-IR and serum markers of inflammation, models were adjusted I-FABP and then additionally for sCD14, sCD163, and IL-6 in separate regression models. The regression coefficients and their confidence intervals (CIs) were then exponentiated to calculate percentage differences attributable to each factor.
In analyses restricted to the subsample of HIV-infected study participants, similar models were sequentially adjusted for the same variables as well as nadir CD4+ T cell count, baseline viral load, ART duration, and ART regimen [non-nucleotide reverse transcriptase inhibitors (NNRTI) vs. PI, and tenofovir disoproxil fumarate (TDF)-containing regimens vs. zidovudine (AZT)-containing regimens].
Finally, we tested this series of models under one theoretical framework using path analysis, which uses maximum likelihood estimation, to examine whether inflammatory markers have mediation effects between HIV status and HOMA-IR, and if so, estimate the direct effect of HIV on HOMA-IR and indirect effect through inflammatory markers. This analytic approach provides a means to estimate the causal relationship between each covariate and IR in both HIV-seronegative and infected individuals. The goodness of fit of the models was evaluated with the χ2 statistic and with the following commonly reported indices: comparative fit index (CFI), standardized root mean square residual (SRMSR), and root mean square error of approximation (RMSEA). Cutoffs for good fit are p value of χ2 > 0.05, CFI >0.9, SRMSR <0.08, and RMSEA <0.06. 26 To account for missing data, we employed the full information maximum likelihood (FIML) approach for its efficiency compared with a multiple imputation (MI) approach, and for its consistency in calculating path coefficients (which MI lacks due to multiple imputed datasets). 27 All analyses were conducted using SAS system, version 9.4 (SAS Institute, Inc., Cary, NC).
Ethical considerations
Study participants gave written informed consent, and the protocol was approved by the Institutional Review Boards of Partners Healthcare and the Mbarara University of Science and Technology.
Results
Participant characteristics
Table 1 shows the demographic and clinical characteristics of the 297 participants included in the analysis, stratified by HIV status. The analytic sample was evenly divided by HIV status (49% PWH, 148/297) and sex (47% female, 140/297). Median age at enrollment was 50 years [interquartile range (IQR): 46–54], with no difference between the subgroups. PWH were less likely to be current smokers than seronegative individuals (p < 0.001). Median BMI was 21 kg/m2 (IQR 19–25 kg/m2) and waist circumference was 81 cm (IQR 74–90 cm) for the whole cohort. There was no difference in either BMI or waist circumference by HIV serostatus (p = 0.95 and p = 0.33, respectively), but women had higher BMI in both groups than men.
Demographic and Clinical Characteristics of 297 Study Participants Stratified by HIV Status
p Value from Pearson χ2 test, Wilcoxon rank-sum test or Fisher's exact test.
SES derived from a series of 24 asset indicators at baseline, using principal component analysis. SES 1 represents the poorest strata, SES 4 represents the richest strata.
ART, antiretroviral therapy; AZT, zidovudine (azidothymidine); BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance; I-FABP, intestinal fatty acid-binding protein; IL-6, interleukin 6; IQR, interquartile range; NNRTI, non-nucleotide reverse transcriptase inhibitor; PI, protease inhibitor; sCD14, soluble CD14; sCD163, soluble CD163; SES, socioeconomic status; TDF, tenofovir disoproxil fumarate.
Participants with HIV had higher I-FABP and sCD14 levels compared with seronegative participants [1792 pg/mL, IQR (1207–2597 pg/mL) vs. 1570 pg/mL, IQR (1129–2094 pg/mL), p = 0.016 and 1468 ng/mL, IQR (1200–1789 ng/mL) vs. 1200 ng/mL, IQR (1028–1470 ng/mL) p < 0.001, respectively]. There was no significant difference in either sCD163 levels [472 ng/mL; IQR (362–609 ng/mL) vs. 501 ng/mL, IQR (363–663 ng/mL) p = 0.062] or IL-6 levels [0.4 pg/mL, IQR (0.3–0.6 ng/mL) vs. 0.4 ng/mL, IQR (0.3–0.5 ng/mL) p = 0.78] by HIV serostatus. HOMA-IR was higher in PWH than in seronegative individuals and higher in women compared with men (p = 0.008 and p < 0.001, respectively). While, none of the assayed inflammatory markers was significantly correlated with HOMA-IR, I-FABP was inversely correlated with HOMA-IR [sCD14 r = −0.11 (p = 0.09); sCD163 r = −0.1 (p = 0.15); IL-6 r = −0.04 (p = 0.60); and I-FABP r = −0.14 (p = 0.041), respectively]. Among participants with HIV, the median nadir CD4+ T cell count was 117 cells/mm3 (IQR 72–183 cells/mm3), the median duration on ART was 8 years (IQR 7.3–8.8 years). The vast majority were on NNRTI-based regimens (n = 113, 76%) and AZT-including regimens (n = 115, 77%).
Association of HIV, inflammatory markers with IR
In multivariate analyses, adjusted for age, sex, diet, socioeconomic status, smoking history, hypertension, and BMI, HOMA-IR remained 37% (95% CI: 5–77) greater in PWH compared with HIV-seronegative participants (Table 2). Additional adjustment for I-FABP modestly strengthened the association of HIV infection with HOMA-IR from 37% (95% CI: 5–77) to 40% (95% CI: 8–82), as well as the association of female sex with HOMA-IR from 47% (95% CI: 10–97) to 51% (95% CI: 13–102), compared with those without HIV and those of male sex, respectively. Additional adjustment for sCD14 also substantially strengthened the association of both HIV infection [59% (95% CI: 21–109)] and female sex [61% (95% CI: 20–114)] with HOMA-IR. Including sCD163 and IL-6 in multivariate models had very little effect on the association of either HIV status or female sex with HOMA-IR.
Factors Associated with Homeostasis Model Assessment of Insulin Resistance After Additional Adjustment for Markers of Immune Activation, Microbial Translocation and Inflammation
Bold refers to statistically significant (p < 0.05) values.
and bAdjusted for hypertension, diet, current and past history of smoking, SES. Change in IR is per doubling in concentration of each biomarker. Coefficients represent percentage increase or decrease. Dietary information missing on 20 persons; I-FABP, sCD163, sCD14, and IL-6 was missing for 11. Full Information Maximum Likelihood approach was used to account for these missing values.
CI, confidence interval; IR, insulin resistance.
In analyses restricted to PWH, women had markedly greater HOMA-IR in demographically adjusted multivariate models [58%, (95% CI: 18–187)], compared with men (Table 3). Every five unit increase in BMI was associated with 49% (95% CI: 18–87) increase in HOMA-IR. Greater baseline viral load [16% (95% CI: 1–33)], but not pretreatment CD nadir [22% (95% CI: −2 to 52)], was associated with significantly greater HOMA-IR. By contrast, each doubling in I-FABP levels was associated with significantly lower HOMA-IR [−18% (95% CI: −38 to −1)] in models adjusted for demographic, lifestyle factors, and body composition. Additional adjustment for each of the assayed inflammatory markers had minimal effect on the association between greater I-FABP and lower HOMA-IR. However, in models additionally adjusted for sCD14, each 100 cell increase in nadir CD4+ T cell count was associated with 26% (95% CI: 2–56) increase in HOMA-IR and the association of female sex with HOMA-IR was 73% higher (95% CI: 19–153). ART duration did not have a significant effect on HOMA-IR in any of the models and was not included in final multivariate regression analyses.
Factors Associated with Homeostasis Model Assessment of Insulin Resistance in Models Restricted to People with HIV Individuals Only and After Additional Adjustment for Markers of Immune Activation, Microbial Translocation and Inflammation
Bold refers to statistically significant (p < 0.05) values.
Change in IR is per doubling in concentration of each biomarker. Dietary information missing on seven persons; I-FABP, sCD163, sCD14, and IL-6 was missing for five. Full Information Maximum Likelihood approach was used to account for these missing values.
Adjusted for hypertension, diet, current and past history of smoking, SES.
In an additional sensitivity analysis that included those persons with confirmed diabetes mellitus, the associations between HIV, each of the assayed biomarkers and HOMA-IR were not markedly different from the analysis that excluded those participants with DM.
Path analysis—the effect of inflammatory parameters on HOMA-IR in HIV
Using path analysis with FIML and standardization of all covariates, we estimated the effect on HOMA-IR that might be mediated by innate immune activation and intestinal epithelial damage (measured by I-FABP). Figure 1 shows the adjusted associations of different covariates with HOMA-IR in a model that included all study participants. Most goodness-of fit statistics indicated a reasonably good fit of the model, with CFI = 0.97, χ2 p value >0.01, SRMSR = 0.03, and RMSEA = 0.07. BMI, HIV status, and female sex were significantly associated with greater HOMA-IR, and a current smoking history was significantly associated with lower HOMA-IR. While both HIV and female sex were associated with significantly higher sCD14, higher sCD14 levels were associated with lower HOMA-IR levels.
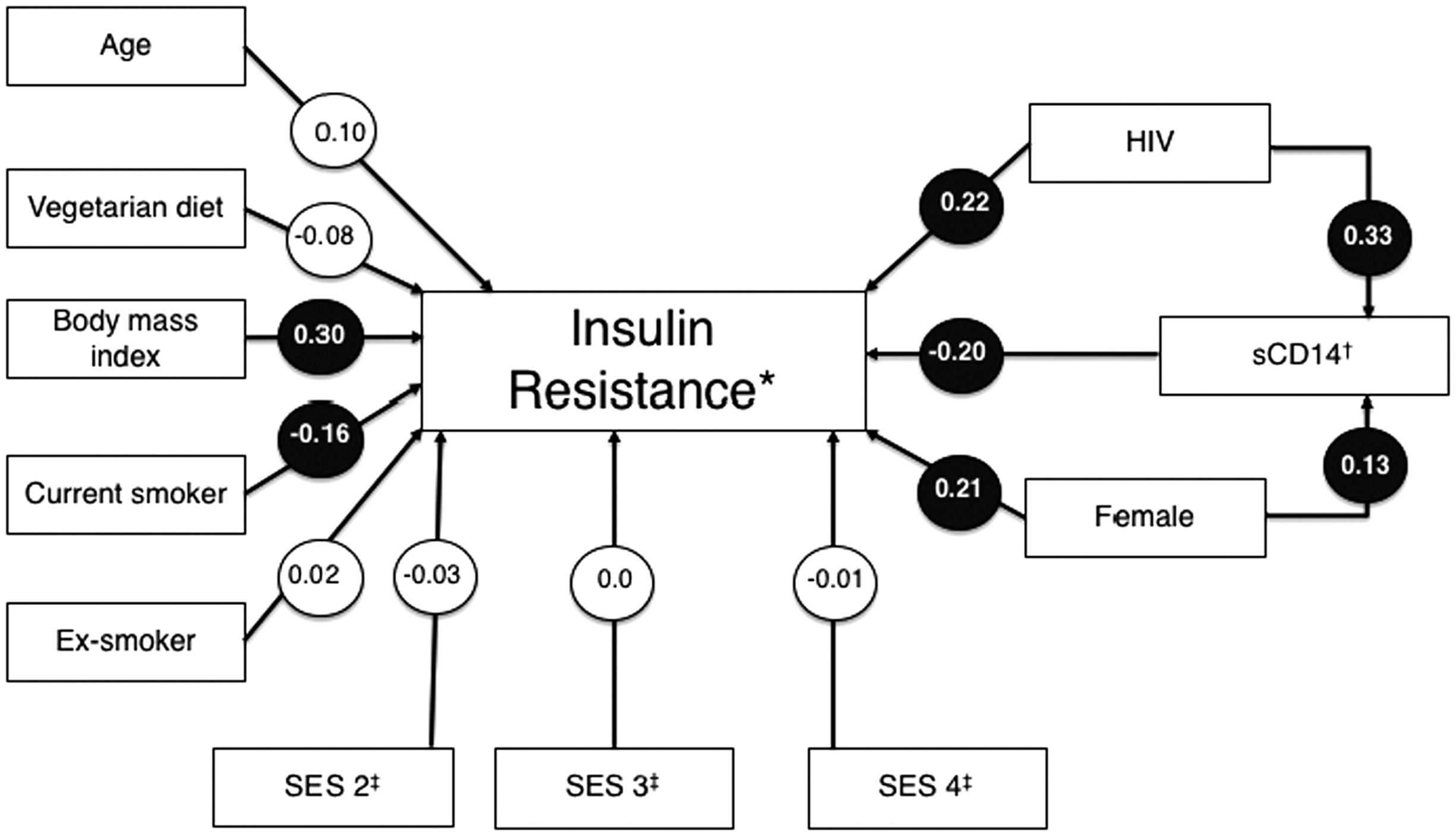
Path analysis: all participants. +All coefficients standardized, emboldened, purple-circled coefficients significant, p < 0.05. Full Information Maximum Likelihood applied to account for missing data; *insulin resistance measured as log change in HOMA-IR; † denotes log change in serum concentration; ‡SES, compared with individuals from SES 1 (i.e., poorest strata). Chi square = 15.94, degrees of freedom = 8; Chi square probability <0.01; SRMSR = 0.03; RMSEA = 0.07; comparative fit index = 0.97. HOMA-IR, homeostasis model assessment of insulin resistance; RMSEA, root mean square error of approximation; SES, socioeconomic status; SRMSR, standardized root mean square residual.
In path analysis restricted to PWH with all variables standardized to enable comparison, we also examined which variables in the model were associated with HOMA-IR. As Fig. 2 illustrates, BMI, female sex, higher nadir CD4+ T cell count and baseline viral load were all associated with greater IR, in a model that demonstrated considerable superiority when covariance matrix was evaluated. All the goodness of fit indices showed a great fit of the model, with CFI = 1.0, 26 χ2 p value = 0.88, RMSR = 0.02, and RMSEA <0.01. Coefficients for the association of both I-FABP and sCD14 with HOMA-IR were negative and significant, (−0.15 and −0.17, respectively). Relative to other variables in the model, baseline HIV viral load had the strongest association with HOMA-IR. There was no interaction between HIV and sex with IR. Further, when we explored a possible association between specific ART regimens and IR, there was no significant difference in HOMA-IR levels according to whether study participants were on AZT (n = 115) or TDF-containing (n = 14) regimens, or PI-based (n = 15) versus NNRTI-containing (n = 113) regimens.
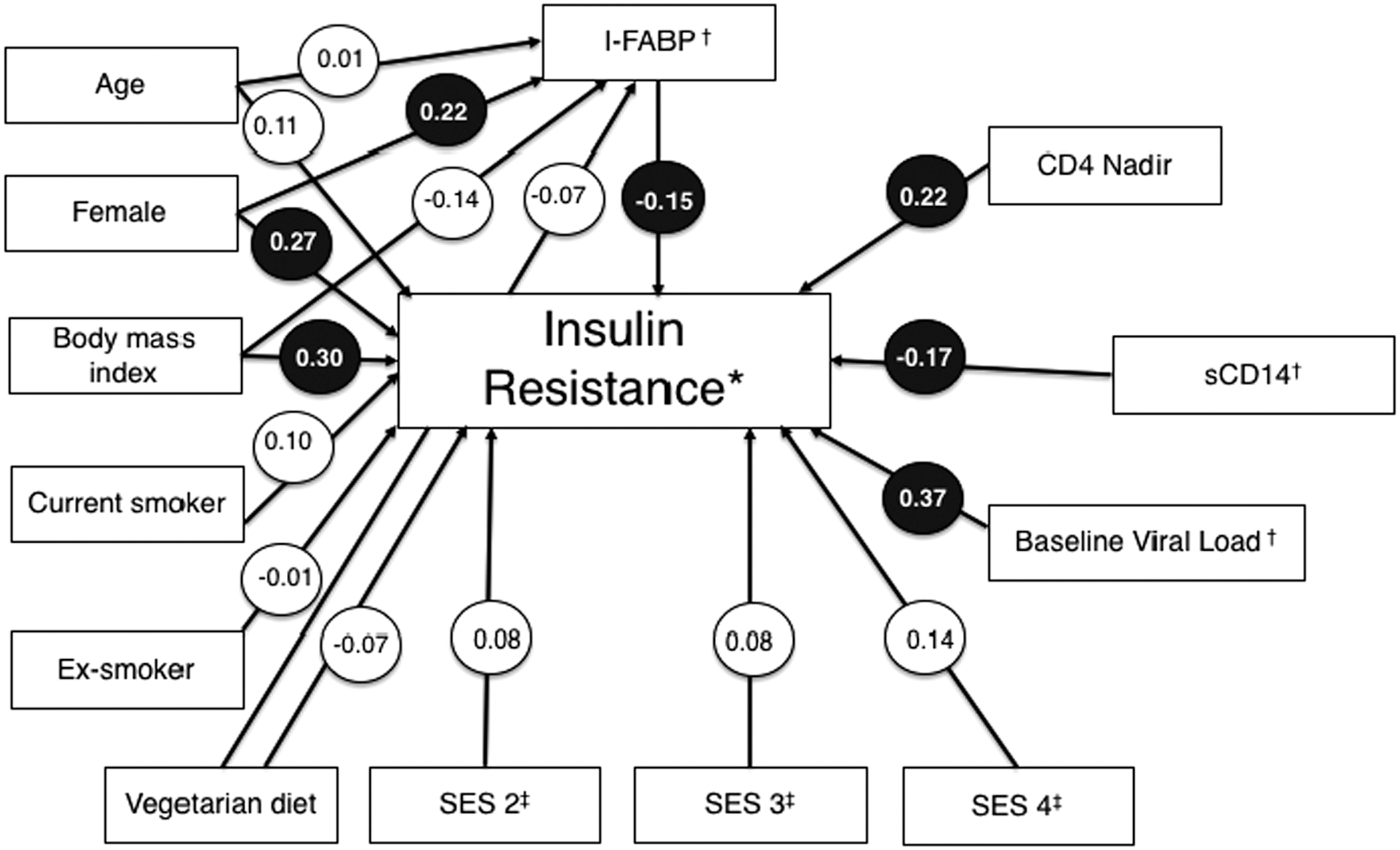
Path analysis: participants with HIV only. +All coefficients standardized, emboldened, purple-circled coefficients significant, p >< 0.05. Full Information Maximum Likelihood applied to account for missing data; *insulin resistance measured as log change in HOMA-IR; †denotes log change in serum concentration; ‡SES, compared with individuals from SES 1 (i.e., poorest strata). Chi square = 3.77, degrees of freedom = 8; Chi square probability <0.88; SRMSR = 0.01; RMSEA = 0.00; comparative fit index = 1.00.
Discussion
In our cross-sectional analysis of PWH on suppressive ART and matched HIV seronegative individuals enrolled in a large Ugandan cohort, we found that HIV infection, female sex, and BMI were strongly associated with HOMA-IR. Contrary to our hypothesis, the association of HIV status with HOMA-IR was not attenuated by greater intestinal epithelial damage nor innate immune activation.
HIV serostatus and IR
Our finding that HIV infection was associated with greater IR in our analysis is consistent with data from SSA, where studies report a high prevalence of impaired fasting glucose 28 and DM 29 in PWH, independent of BMI. 30 We observed that PWH had 37% higher HOMA-IR compared with HIV-seronegative persons, even after adjusting for BMI. In path analysis, we found that higher nadir CD4+ T cell levels and higher baseline viral load were associated with greater IR, even after adjustment for markers of immune activation. ART initiation earlier during HIV infection may predispose to greater risk for IR due to a more rapid normalization of health and weight gain, whereas greater viral replication before initiating ART may potentiate HIV-associated fat loss. 31 HIV studies from the United States 32,33 have shown an association of HIV infection (independent of ART type) with subcutaneous fat loss and in the general population, severe subcutaneous fat loss or lipoatrophy has been associated with IR, 34 which could be a possible mechanism for the association of HIV with IR independent of BMI. In our analysis, we did not find that any specific ART drug or drug class was a significant mediator of IR, although drug class comparisons were limited by the small number of participants on TDF or PI-based regimen.
HIV, inflammation, and IR
Consistent with research in the US, levels of both I-FABP and sCD14 were significantly higher in PWH, compared with age and sex-matched controls. 35 However, our finding that markers of innate immune activation are not associated with IR in the setting of HIV is contrary to our prior findings and others from the United States and Europe. 35,36 We found that in US women with HIV, soluble inflammatory markers, in particular sCD163, 35 was associated with IR and DM. 36 By contrast, in this Ugandan study, higher levels of I-FABP was associated with lower HOMA-IR levels in PWH. 37 Given the wide CIs associated with models, including I-FABP, these findings should be interpreted with caution. However, it is possible that the differences found in this study compared with our research in women with HIV in the United States may be explained by differences in the patient populations in the United States and Uganda and may reflect that PWH in Africa are more likely to start ART at much lower BMIs, where inflammation is less likely to be related to obesity-related factors that are more prevalent among PWH in the United States. This hypothesis is supported by a recent study of PWH in the United States, where I-FABP was inversely associated with BMI and visceral adiposity, suggesting that increased I-FABP may be related to changes in nutrient absorption and body composition. 38 Future studies to investigate the role of intestinal damage on nutrient absorption and IR are needed to elucidate the mechanisms of these relationships.
Body mass index and IR
Consistent with research performed in US and European cohorts, 35,39,40 as well as recent data from elsewhere in SSA, 41,42 our analysis confirmed that higher BMI was strongly associated with greater IR; in the demographically adjusted models that included all study participants, regardless of HIV status, each five unit increment in BMI was associated with a 42% greater HOMA-IR. While the median BMI in this population was relatively low, the association between BMI and HOMA-IR is particularly relevant given the increasing prevalence of obesity, both in the general population and among PWH in SSA. 43,44 In this cross-sectional analysis, we were not able to assess the impact of change in BMI on HOMA-IR, which may have been substantial, especially for PWH who recently started ART. Interestingly, a study of PWH in Zambia and Tanzania, who started ART at a low BMI found that the risk of pre-DM or DM after treatment initiation was paradoxically highest among those with the lowest pre-ART BMI. 37 The importance of body composition changes, especially those with lower pretreatment BMI, 45 as a potential driver of diabetogenesis, 46 has been described in high-income settings and we intend to explore this in an additional prospective analyses in this cohort.
Female sex and IR
The association between female sex and IR was also striking; HOMA-IR levels were 47% higher in women compared with men in multivariate models. Our path analysis demonstrated that this association was independent of BMI. Of note, studies from SSA and the United States have demonstrated that black women, especially premenopausal women, are more insulin resistant than other ethnic groups 47,48 and when compared with men. 49,50 Data from Western Europe 51 and Asia 52 have reported that accumulation of visceral adipose tissue (VAT) is an important determinant of increased IR in women. However, US studies also show that black women have less VAT than black men. 32,33 Whether sex differences in VAT in SSA is a driver of IR, especially among PWH on ART, is unclear.
In our study, the association of female sex and IR was strengthened in models adjusted for each of the assayed inflammatory biomarkers, although the effects of adding I-FABP, sCD163, and IL-6 were modest, and CIs for coefficients associated with these associations were wide. Adjustment for sCD14 led to an absolute increase in the association between female sex and IR of 22%. Path analysis confirmed this interaction: sCD14 levels were higher in women than men, but greater sCD14 concentration was associated with lower HOMA-IR. The mechanism behind the differences in IR in women, and the mitigating effect of sCD14 should be an area of active investigation, particularly because sCD14 levels are strongly and independently correlated with all-cause mortality in treated infection in Europe 53 but not Uganda. 54 Greater VAT has been associated with lower sCD14 in an analysis of North American PWH 55 and may explain the association highlighted in our analysis. Notably, in our earlier work we have also demonstrated an inverse, although non-significant, association between sCD14 and hypertension in PWH in Uganda. 56 Inverse associations of sCD14 with hypertension and IR represent an ART-mediated ‘return to health.’ 57 It is also possible that gender differences in body composition, independent of ART, but poorly characterized by BMI (such as visceral adiposity) explain this finding. Further prospective studies are needed to characterize the causal pathways linking HIV and effective ART and body composition with changes in circulating inflammatory mediators, and to understand how these influence diabetes risk. Unfortunately, the majority of participants in our study were on the same ART regimens, limiting comparisons between classes or individual HIV drugs.
Limitations
Our study has some important limitations. First, we were unable to make conclusions about causal relationships due to the cross-sectional design of the study. While path analysis helps to clarify the nature of the relationship between the independent and dependent variables, we are cautious not to overinterpret modest changes in regression coefficients that have wide CIs; further prospective research is necessary to validate the findings in our analysis. Second, we acknowledge that the results should only be generalized to rural East African populations, characterized by subsistence farming, and high rates of food insecurity and biomass cooking fuel exposure. 58,59 Third, since many potentially important factors, including data on specific comorbidities, alcohol consumption, waist circumference, and adipose tissue parameters, were not included in the regression analyses, we are unable to rule out confounding by these factors. Further, we did not perform duplicate testing of inflammatory assays. However, all inflammatory markers were tested at globally respected laboratory, where extensive internal quality control is routinely performed. Finally, we used I-FABP as a surrogate of gut permeability instead of blood concentrations of bacterial LPS. We recognize the limitations of HOMA-IR as a predictor of diabetes. 60 Nonetheless, it is a robust clinical and epidemiological tool in descriptions of the pathophysiology of diabetes and relevant for use in this setting, especially given the high increasing incidence of diabetes and prediabetes both among PWH and in the general population, especially in women. 5 These data should prompt additional attention to the determinants of IR, especially among women, in the region and a concerted effort to identify effective interventions to mitigate the risk of ensuing diabetes mellitus.
Conclusions
HIV, female sex, and higher BMI are positively associated with IR in rural Uganda. Contrary to findings elsewhere, we found that biomarkers of inflammation and gut permeability appeared to be protective against IR, and strengthened the association of both HIV and sex with greater IR. It is plausible that this may be due to residual relationships between HIV-associated inflammation and underweight or wasting. The interplay between HIV disease, ART, and traditional risk factors in the pathophysiology of IR and diabetes in SSA PWH is yet to be fully understood. There is a need for long-term longitudinal studies to elucidate the role of various risk factors in the pathogenesis of IR and future research in evaluating interventions to disrupt the progression of prediabetes to overt DM.
Footnotes
Acknowledgments
This work was supported by the US National Institutes of Health (R21 HL124712, P30 AI060354, R24 AG044325, P30 AG024409, K23 MH099916) and a grant from UCSF's AIDS Research Institute.
Author Disclosure Statement
No competing financial interests exist.