
Abstract
Pre-exposure prophylaxis (PrEP) has the potential to significantly reduce HIV incidence among men who have sex with men (MSM) in the United States. However, the extent to which suboptimal PrEP adherence and retention in care may limit successful implementation is unknown. An agent-based model was used to represent the entire population of MSM in Rhode Island from 2013 to 2017. The impact of potential interventions to improve PrEP adherence and retention in care on HIV transmission was evaluated. Demographics, behaviors, and PrEP adherence and retention in care rates were based on local clinical data. We assumed that 20% of HIV-negative MSM had ever taken PrEP. The primary outcome was HIV incidence over the 5-year period. The model included 23,815 MSM with an estimated 4.1% HIV prevalence based on local surveillance data. An estimated 173.1 new infections occurred over 5 years [95% simulation interval (SI): 171.5–174.7], including 29.1 new infections among individuals who had ever initiated PrEP (95% SI: 28.6–29.7). Interventions that improved retention in PrEP care by an odds of 5.0 compared with the base case maximized reductions in HIV incidence among MSM who had ever initiated PrEP by 37.5%. Interventions focusing on improving PrEP adherence had little to no effect on HIV incidence, regardless of intervention efficacy. Retention in care is a critical component of the PrEP care continuum. Interventions that improve retention in PrEP care may lead to greater reductions in population-level HIV incidence compared with interventions focused exclusively on adherence.
Introduction
Men who have sex with men (MSM) continue to be disproportionately impacted by HIV in the United States, with a 1 in 11 lifetime risk of HIV infection. 1 Pre-exposure prophylaxis (PrEP) is highly efficacious in preventing HIV acquisition and has the potential to help achieve the goals of the National HIV/AIDS Strategy. 2,3 Defining a PrEP care continuum is important to identify gaps in implementation and includes PrEP awareness, linkage to care, initiation, adherence, and retention in care. 4 Previous studies have demonstrated challenges in the initial stages of the PrEP care continuum. 4 A previous agent-based model (ABM) of HIV transmission among MSM in Rhode Island found that substantial increases in uptake are needed to decrease HIV incidence in this setting, 5 with other modeling studies reaching similar conclusions. 6,7 However, less is known about adherence and retention in PrEP care in real-world settings and their impact on population-level HIV incidence. Previous studies have demonstrated suboptimal adherence and low retention in care that may significantly impact the effectiveness of PrEP at the population level. 8 –10
Adherence to daily pill taking is essential for conferring individual-level protection from HIV infection. 11 Several studies have demonstrated that poor adherence to PrEP has the potential to considerably diminish estimates of efficacy in randomized controlled trials. 8,9 Several measurements are often used to characterize adherence, including measures based on self-report, pill counts, and serum drug levels, leading to challenges in assessing adherence and strategies to improve it. 12 Adherence to daily pill taking is heavily impacted by several barriers, including anticipated and enacted stigma, where individuals do not want to be seen taking PrEP because of concerns about being perceived be promiscuous and/or living with HIV infection. 13
The reasons for PrEP discontinuation are much less understood than those for nonadherence to PrEP. Reductions in perceived risk for HIV infection because of changes in sexual behaviors are a common reason for discontinuation. In qualitative interviews with MSM in Rhode Island, Underhill et al. 14 found that many individuals report temporal shifts in risk behavior, perceived risk of HIV infection, and willingness to use PrEP. In some periods of increased numbers of sexual partners, for example, perceived risk of HIV infection is higher, corresponding to higher willingness to use PrEP. 14 In other periods, where numbers of sexual partners are lower (i.e., beginning of a monogamous partnership), perceived risk of HIV infection is lower, corresponding to lower willingness to use PrEP. 14 However, the oscillation of risk behaviors does not fully account for all instances of PrEP discontinuation and other factors (e.g., changes in insurance coverage and physician access) also impact short- and long-term retention in care. 10
To improve adherence and retention in PrEP care, various clinical and behavioral interventions are being developed, 7 –10 involving counseling, 15 education, 16 mobile technologies, 17 patient/peer navigation, 18 and case management. 19 Although suboptimal adherence and retention in care can dampen the individual-level benefits of PrEP, the optimal levels of adherence and retention in PrEP care needed to maximize reductions in HIV incidence at the population-level are not well understood. Using data from a real-world PrEP program, we adapted an existing ABM to evaluate the potential effectiveness of interventions focused on improving adherence and retention in care. We sought to determine optimal intervention efficacy at which reductions in population-level HIV incidence were maximized.
Methods
Study setting
The Rhode Island Sexually Transmitted Diseases (STD) Clinic is the only publicly funded STD clinic in the state. 20 In 2013, the clinic began offering PrEP to patients with behavioral indications according to recommendations from the United States Public Health Service. 21 We reviewed patient data from 2013 to 2017 for all MSM prescribed PrEP at our clinic including demographic, behavioral, and laboratory data. Retention in care was evaluated based on attendance in quarterly clinical visits, with data extracted on attendance at visits 3 and 6 months after initiation. Adherence was based on the self-reported number of missed doses in the preceding 7 days at each of these clinical visits, which previous studies have found to be highly correlated with drug concentration levels in this setting. 22
Institutional Review Board approval and consent
This study was approved by the institutional review board at the Miriam Hospital. This study also received a waiver of consent.
Model setting
Clinic data were used to parameterize an ABM that simulated HIV transmission over a 5-year period among a virtual population representing all MSM in Rhode Island. All model parameters and processes have been described previously. 5 The agents in the model were assigned specific demographic, behavioral, and clinical characteristics (including probabilities of adherence and retention in care) with distributions informed by data on MSM who initiated PrEP at the Rhode Island STD Clinic. Other local surveillance data and estimates also informed this model (Table 1).
Key Parameter Values for an Agent-Based Model (ABM) Assessing Pre-Exposure Prophylaxis (PrEP) Implementation Among Men Who Have Sex with Men (MSM) in Rhode Island
Model progression
The ABM simulated a dynamic population in a steady state, where agents left the population at death or because of aging at 65 years. Agents were replaced based on demographic, behavioral, and clinical attributes drawn stochastically from the same distributions used to develop the base population. The model progressed in discrete monthly time-steps, during which agents were able to form and dissolve sexual partnerships. At the beginning of each year, agents were assigned target numbers of partners and sex acts for that year drawn from local data. 23 Agents were able to form sexual partnerships with each other at a given time-step and additional partnerships at future time-steps in a probabilistic fashion based on their target annual number of partners. Partnerships were assigned a set duration at their formation, allowing for a dynamic sexual network where partnerships are formed and dissolved over time. All simulations were coded, tested, and calibrated in Python (Version 2.7.13). All model outputs were analyzed in R (Version 3.5.3).
HIV transmission
At model initialization, agents were assigned a sexual role to determine their position during anal sex (receptive or insertive). The probability of condom use within the partnership was a function of the number of previous sexual acts with a given partner, where condom use was most common in new partnerships. 24 Condom-protected sex acts were assumed to carry no risk. All condomless anal sex acts within serodiscordant dyads were assumed to carry some risk of HIV transmission, where the base estimates of per-act risk of HIV transmission were set at 1.38% and 0.11% for receptive and insertive anal sex, respectively. 25 These probabilities were scaled based on whether the HIV-positive partner within the dyad was aware of their infection status, was on treatment, and had achieved viral load suppression, and whether the HIV-negative partner within the dyad was using PrEP. The proportion of HIV-positive agents aware of their infection status was estimated to be 82% and the proportion of HIV-positive agents who had achieved viral load suppression was set at 27%. 26
Model scenarios
In the base case scenario, agents using PrEP were retained in care at 6 months after initiation with a probability of 60% and were adherent (i.e., took four or more doses per week) with a probability of 82%, based on observed clinic data. 10 The impact of varying adherence and retention on the number of HIV infections averted (NIA) in counterfactual scenarios were then determined for the overall population of MSM, and the population of MSM who had ever initiated PrEP. The first scenario held adherence constant with a probability of 82% while varying the proportion of agents retained in care from 60% to 88% (based on the increases predicted by a hypothetical intervention that improves retention based on odds up to 5.0). The second set of scenarios held retention in care constant with a probability of 60% while varying the proportion of agents with optimal adherence from 82% to 96% (simulating a hypothetical intervention that improves adherence with odds up to 5.0). NIAs for each counterfactual scenario were calculated as the mean difference between the cumulative number of infections in the base case and the cumulative number of infections in the modeled scenario. These estimates are also presented as percent change in the cumulative number of infections.
Each scenario began in January 2013 and ended in December 2017. This 5-year period was selected as the time horizon for all model scenarios as this represents the time after which no agents who initiated PrEP at model initialization would be retained in care, assuming no further initiation of other agents on PrEP. As described previously, the ABM was calibrated to reproduce the observed HIV diagnosis and estimated prevalence trajectories in Rhode Island from 2009 to 2013. 27 Each of these scenarios was simulated 500 times and all runs were subject to a burn-in period (i.e., a period in which transmission was simulated without PrEP) of 4 years before the initiation of the PrEP program. With all outcome measures, we report 95% simulation intervals (SIs) as measures of uncertainty.
Results
The model was based on the total population of MSM in the state of Rhode Island (n = 23,815), 28 with an estimated 4.1% prevalence of HIV infection. 29 At model initialization, 20% of HIV-negative MSM were assumed to have ever initiated PrEP. 10 In the base case scenario, there were an estimated 173.1 new infections over 5 years (95% SI = 171.5–174.7), including 29.1 new infections among the individuals who had ever initiated PrEP (95% SI = 28.6–29.7).
Assuming constant levels of adherence (82%), interventions focused on increasing retention in PrEP care had a significant impact on the overall reduction in new HIV infections among MSM. As retention in PrEP care increased from 60% to 75% [intervention efficacy odds ratio (OR) = 2.0], the number of new HIV infections among MSM who had ever initiated PrEP (Fig. 1) decreased from 29.1 (95% SI = 28.6–29.7) to 26.2 (95% SI = 25.7–26.7), representing a reduction of 13.8% (95% SI = 12.2 = 15.3). Maximum reductions were observed when retention in PrEP care was 88% (equivalent to an intervention OR of 5.0), which resulted in a 37.5% reduction in HIV incidence among MSM who had ever initiated PrEP.
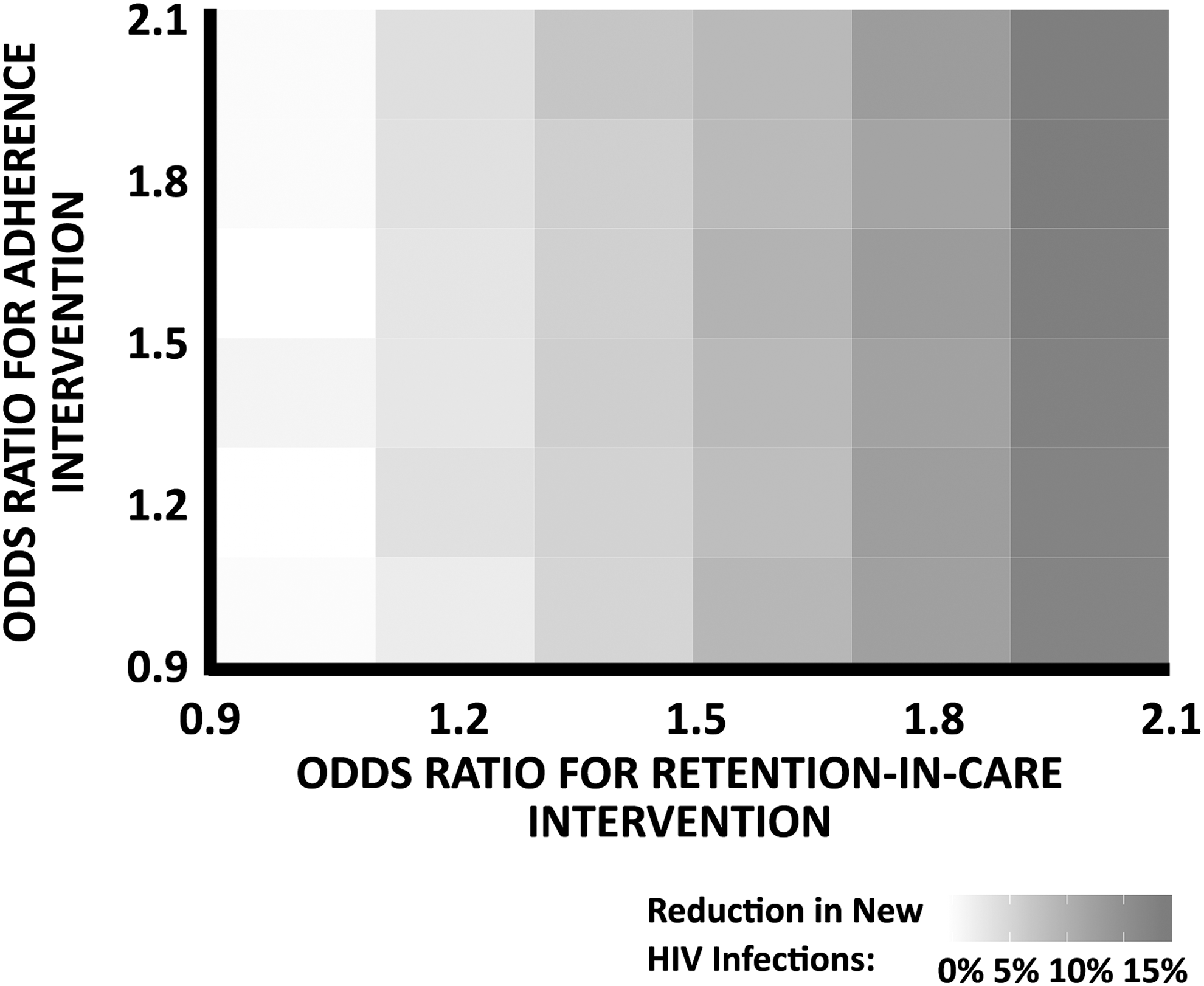
Estimated impact of a joint intervention improving adherence and retention in care among men who have sex with men who use pre-exposure prophylaxis on HIV incidence. Each tile in the chart notes a different combination of intervention efficacies for improving retention in care (ORs from 1.0 to 2.0) and for improving adherence (ORs from 1.0 to 2.0). Looking across the rows, HIV incidence is reduced when retention in care is improved, but looking down the columns, there is little or no difference when adherence is improved on its own. OR, odds ratio.
Assuming constant rates of retention in PrEP care (60%), increasing the proportion of MSM with optimal adherence to PrEP had little to no effect on the overall number of new HIV infections among MSM over the simulation period. As adherence increased from 82% to 92%, the number of new HIV infections among MSM who had ever initiated PrEP remained constant (Fig. 1), with 29.1 (95% SI = 28.6–29.7) and 29.7 (95% SI = 29.1–30.2) infections over 5 years in each scenario, representing little or no change from the base case scenario (2.4% reduction; 95% SI = −0.5 to 4.2).
In scenarios where adherence and retention in care were jointly varied (Fig. 1), synergistic reductions in the number of new HIV infections among MSM who had ever initiated PrEP were not observed.
Discussion
This is among the first studies to evaluate the population-level impact of potential interventions targeting adherence and retention in PrEP care on HIV incidence among MSM. We found that lower rates of retention in PrEP care and not adherence alone led to increased HIV transmission. Retention in PrEP care is tightly linked to adherence but focusing only on adherence may overlook the importance of retention. In our model, interventions that improved retention in PrEP care led to greater reductions in HIV incidence compared with interventions that improved adherence alone. Although early studies suggested that PrEP adherence may be a limiting step during implementation, our previous work 10 and this study suggest that retention in PrEP care may be as or more important as efforts to promote adherence alone. In addition, we determined the optimal effectiveness of an intervention targeting retention in PrEP care to maximize reductions in HIV incidence. These results will help guide PrEP implementation and intervention development to achieve optimal outcomes across the PrEP care continuum. Future models should explicitly incorporate race/ethnicity to identify the impacts of these interventions on disparities in HIV incidence among key populations (e.g., young black/African American MSM).
Retention in PrEP care is one of the least studied aspects of the PrEP care continuum. 4 Emerging data suggest that retention in PrEP care is suboptimal across multiple populations. 10 Reasons include individual-, social-, and structural-level challenges including cost, stigma, risk perception, side effects, and access to care. 10,13 Of note, adherence and retention in PrEP care are inter-related. Individuals who are retained in PrEP care are largely adherent to the medication. 10 However, individuals who are not retained in PrEP care cannot be adherent. Although adherence is needed for PrEP to be effective, retention in care is the critical step that undergirds, precedes, and promotes adherence. Of importance, individuals retained in care may benefit from other HIV prevention approaches (e.g., routine HIV screening), even if they are suboptimally adherent to PrEP.
We find that enhancing retention in PrEP care could achieve an estimated 40% reduction in HIV incidence with an intervention efficacy of 5.0. After this point, population-level changes in HIV incidence would be minimal. Interventions focused on improving PrEP adherence alone had little to no effect in our study. Previous interventions focused on retention in HIV care have demonstrated an effect of up to an OR of 3.0. 30 These retention in HIV care interventions have focused on mobile health programs, case management, peer/patient navigation, support services, and others. 31 Given this, achieving a PrEP intervention with an OR of 5.0 may be optimistic, but suggests a possible ideal intervention goal.
This study is subject to several limitations. The model was based on the state of Rhode Island and results may not be generalizable to other settings. As with any model, some assumptions were made. We assumed a higher estimate of PrEP uptake than in reality, which was needed to fully evaluate PrEP outcomes. However, every attempt was made to otherwise use local data that reflected the current population. Our findings have important implications for PrEP implementation across the United States.
In conclusion, this is among the first studies to evaluate interventions focused on improving adherence and retention in PrEP care and effect on population-level HIV incidence. Interventions that improved retention in PrEP care had the greatest impact on reducing population-level HIV incidence, but improvements plateaued at a given level. These results suggest that interventions targeting retention in care should be a focus to achieve optimal PrEP continuum of care outcomes. In addition, long-acting antiretroviral drug formulations should be considered for populations that face disproportionate barriers to adherence and retention in care and could benefit from the longer periods of protection that may be conferred by these modalities. 32
Footnotes
Acknowledgments
The study was supported by grants R21MH109360 and R01MH114657. Additional support was provided by the Providence/Boston Center for AIDS Research (P30AI042853).
Author Disclosure Statement
No competing financial interests exist.