
Abstract
Antiretroviral therapy (ART) adherence is vital for optimal HIV treatment. However, there is limited ART adherence research on the US Latinx population, who are at increased risk for HIV infection and worse HIV health outcomes. This study examined electronically measured ART adherence (Medication Event Monitoring System) and its association with demographic, clinical, neurocognitive, and sociocultural variables in Latinx and non-Latinx white (NLW) persons living with HIV [PLWH (N = 128)]. Latinx participants demonstrated worse adherence than NLW participants (p = 0.04). Linear regressions revealed different predictors of adherence. Among Latinx participants, recent cocaine use, stress, and, unexpectedly, higher US acculturation predicted worse adherence (ps < 0.05). Among NLW participants, recent cocaine use predicted worse adherence (p < 0.05). Intergroup comparisons within the Latinx group were not conducted due to subsample size. Thus, ethnicity, sociocultural variables, and cocaine use are important considerations for ART adherence, and poor ART adherence may be one pathway explaining worse outcomes in Latinx PLWH. Culturally tailored adherence interventions incorporating substance use treatment, acculturation, and stress management are warranted to improve health outcomes.
Introduction
Latinx adults in the United States are disproportionately affected by health disparities, particularly HIV/AIDS. Latinx adults comprise 18% of the US population, 1 but account for ∼25% of new HIV diagnoses per year. 2 Further, HIV prevalence in the US Latinx population is expected to grow, comprising up to 32% of HIV cases in the United States by 2045. 3 Upon seroconversion, Latinx persons living with HIV (PLWH) also experience worse health outcomes compared with their non-Latinx white (NLW) PLWH counterparts, including earlier mortality and higher rates of comorbidities, such as HIV-induced cognitive and functional impairment also known as HIV-associated neurocognitive disorders. 4 –11 While the reasons for these worse health outcomes among Latinx PLWH remain poorly understood, an important factor to consider is antiretroviral therapy (ART) adherence.
Optimal ART adherence is necessary for HIV viral suppression and has been associated with higher CD4 count (i.e., immune reconstitution) and decreased rates of hospitalization, opportunistic infections, morbidity, and mortality. 12 –16 Most research suggests that PLWH should maintain a 90–100% adherence rate for ART to be effective. 13,15,16 Suboptimal ART adherence is associated with worse health outcomes, including incidence of multidrug-resistant viral strains, increased morbidity, and higher rates of disease transmission. 15,17 –19
Among primarily NLW and African American PLWH, worse ART adherence is associated with neurocognitive dysfunction; psychiatric disorders/substance use; psychosocial difficulties (i.e., HIV-related stigma, poor social support, and poor patient/physician relationships); and sociocultural factors [i.e., quality of education, socioeconomic status (SES), acculturation 20 –25 ]. Research also suggests a bidirectional relationship between neurocognitive functioning and ART adherence, such that better ART adherence is associated with better neurocognitive functioning and vice versa. 21,22,26 –28 However, these relationships remain poorly understood in the Latinx PLWH population.
Of the limited research focused on US-based samples of Latinx PLWH, studies suggest that Latinx PLWH may be less adherent to ART, but important methodological and sociocultural considerations warrant attention. In one large-scale study of self-reported adherence, 29 several Latinx PLHW subpopulations (i.e., Caribbean, Central American, South American origin) reported lower adherence rates in comparison with NLWs and other racial/ethnic minority groups, but the authors noted that a major limitation of this study was the omission of acculturation data to better understand these findings.
Another important consideration is how adherence is measured—few studies inclusive of Latinx PLWH, of which we are aware, have utilized electronic measures of adherence. The adherence research conducted with Latinx PLWH has primarily relied on self-report measures of ART adherence, 30 –32 yet research has shown that self-report may overestimate adherence. 33 One study that utilized directly observed therapy (DOT) found that Latinx PLWH were significantly more likely to make errors when taking their ART medications than their NLW counterparts, but did not examine sociocultural factors to contextualize these findings. 34
Only one study to date that used an electronic measure of ART adherence, Medication Event Monitoring System (MEMS caps), 35 also examined the role of sociocultural factors in ART adherence among Latinx PLWH. 36 Specifically, Robbins et al. found that better ART adherence was associated with higher acculturation to both majority culture (United States) and “culture of origin” (Latinx), which includes either physical (i.e., birthplace) or family cultural origin. Thus, there is also a need to (1) examine electronically measured ART adherence in this population (i.e., MEMS 35 ) and (2) comprehensively characterize potential predictors of ART adherence.
Similarly, another important limitation in the current literature is the insufficient exploration between sociocultural factors, medication adherence, and neurocognitive functioning. While acculturation is linked to neurocognitive functioning in Latinx PLWH, 37 this research does not investigate the relationship between sociocultural factors and ART adherence among Latinx PLWH. Prior research among Latinx clinical populations other than HIV (e.g., those living with diabetes, hypertension, cancer, liver disease) has found that sociocultural factors (e.g., acculturation, language, health literacy) are associated with treatment adherence. 38 –41 Despite these important findings, no research to date has taken a comprehensive approach to characterizing adherence in Latinx groups while simultaneously measuring other potential contributing factors (e.g., depressive symptomatology, substance use).
In sum, research suggests that Latinx adults experience worse HIV-associated health outcomes and are more likely to have suboptimal ART adherence. This suggests ART adherence may be an important pathway for understanding health disparities experienced by Latinx PLWH, but no study to date has examined these issues while electronically measuring ART adherence. Further, no study to date has utilized a comprehensive biopsychosociocultural theoretical framework 42 to assess ART adherence in this population, including consideration of neurocognitive, psychiatric/substance use, psychosocial, and sociocultural factors.
Therefore, the aim of this study was to apply this framework to understand adherence among Latinx PLWH. To that end, we sought to compare rates of electronically measured ART adherence over the course of 30 days and to characterize if and how neurocognitive functioning, psychiatric/substance use, psychosocial, and sociocultural factors contribute to ART adherence in a well-characterized sample of NLW and Latinx PLWH participants. It was hypothesized that: After accounting for relevant covariates the Latinx group would demonstrate significantly worse, electronically measured ART adherence compared with the NLW group. Neurocognitive functioning, psychiatric/substance use (i.e., depressive symptomatology and recent substance use based on urine toxicology results), and sociocultural factors (i.e., quality of education, SES, health literacy, medication beliefs, perceived stress) would significantly predict ART adherence in both the Latinx and NLW groups. Acculturation to US culture and Latinx culture of origin would be significantly positively associated with ART adherence in the Latinx group.
Methods
Participants
A total of 128 PLWH (95 Latinx and 33 NLW participants) participated in the NIMH-funded Medication Adherence Study (K23MH078718; Principal Investigator: M. Rivera Mindt) at the Icahn School of Medicine at Mount Sinai (ISMMS) in New York City. A majority of participants were recruited through community-based outreach and self-referral in Spanish Harlem and the Bronx. Participants were also referred to the study by clinics and related research studies at ISMMS.
Inclusion criteria
All participants were HIV-seropositive (confirmed by medical records), 18–80 years old, self-identified as Latinx (of any race) or NLW, and proficient in English. To ensure familiarity with their medication regimen, only participants who were independently taking their prescribed ART medications in pill form for at least 12 weeks were included in the study.
Exclusion criteria
Participants were excluded if they met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria for current or past schizophrenia spectrum and other psychotic or bipolar disorders based on a structured clinical interview (i.e., Composite International Diagnostic Interview 43 ) administered by trained research staff.
Procedures
All participants provided written informed consent. This study was approved by both the ISMMS and Fordham University Institutional Review Boards (IRB). Participants completed two study visits ∼30 days apart.
During the first visit, participants underwent brief neuromedical evaluations (i.e., neuromedical interview, blood draw, urine toxicology), comprehensive neurocognitive and psychiatric/substance use assessments, and demographic and psychosociocultural questionnaires. They were also trained to use the MEMS and were sent home with instructions and an MEMS bottle and cap to use for 30 days. During the second visit, participants returned the MEMS caps for data analysis and completed an MEMS follow-up survey. Participants were compensated for their time.
Neuromedical evaluation
Participants completed a brief neuromedical questionnaire assessing HIV-related medical history, including nadir CD4, viral load, date of HIV diagnosis, current and past medical history, and current medications (including ART). They also underwent a blood draw for CD4 cell count and plasma HIV viral load assays.
Psychiatric/substance use evaluation
Recent depressive symptoms were assessed using the Beck Depression Inventory-II (BDI-II total score 44 ). Participants provided a urine sample for toxicology testing for the presence of cocaine and other illicit substances (e.g., heroin, nonprescribed marijuana).
Neurocognitive evaluation
Table 1 summarizes the comprehensive neurocognitive evaluation that participants completed, which assessed seven neurocognitive domains: verbal fluency, executive functioning, processing speed, attention/working memory, learning, memory, and psychomotor functioning. This battery has been well validated for use in HIV/AIDS research. 45 Trained psychometrists administered the battery using standardized procedures. A board-certified clinical neuropsychologist (M.R.M.) oversaw all data collection and interpretation.
Neurocognitive Measures and Normative Data Sources
Consistent with empirically supported methods, raw neurocognitive test scores were transformed into demographically corrected T-scores using the best available published normative data (see Table 1). 6,46 The T-scores of the individual tests in each domain were averaged to create neurocognitive mean domain T-scores, and all individual test T-scores were averaged to create the Global Neurocognitive Average T-score, which reflects global neurocognitive functioning. Consistent with prior literature, Global Neurocognitive and Neurocognitive Domain Average T-scores less than 40 were considered impaired. 47
Demographic, psychosocial, and sociocultural evaluation
Demographics
The demographic questionnaire assessed age, years of education, gender, race/ethnicity, employment status, SES, housing status, and language use.
Quality of education
Quality of education was measured using the Wechsler Test of Adult Reading (WTAR). The WTAR is a test of single-word reading that was developed as a measure of estimated premorbid functioning. Single-word reading tests, including the WTAR, have been validated as a measure of the quality of education. 48 –50 The WTAR has well-established reliability and validity. 51 The WTAR Standard Score was used in all analyses.
Acculturation
The Abbreviated Multidimensional Acculturation Scale (AMAS 52 ) is a self-report, bidirectional measure that assesses acculturation levels to both majority culture (United States) and culture of origin (Latinx). It includes six subscales (three for each culture) related to language competence, cultural competency, and cultural identity, producing two summary scores: (1) Total US Acculturation Score and (2) Total Latinx Acculturation Score (scores range from 1 to 4; higher scores indicate higher acculturation levels). The AMAS has excellent psychometric characteristics and has been validated with the urban populations of PLWH similar to the current sample. 53 For this study, the AMAS Total US Acculturation and Total Latinx Acculturation Scores were used.
Socioeconomic status
Information about participants' educational and occupational history was obtained through a demographic questionnaire. SES was estimated using the Hollingshead Index of Social Prestige (ISP) score, which was calculated based on a weighted sum of the participant's educational level and occupational rank 54 and is among the most commonly used SES measures in the literature. 55 For a more detailed description of the Hollingshead ISP calculation in this sample, see Arentoft et al. 56
Health literacy
The Test of Functional Health Literacy (TOFHLA) objectively measures comprehension of health-related materials, testing reading comprehension and arithmetic ability. 57 There are three separate factors (literacy for prose passages, literacy for appointment slips, documents, and prescription bottle directions, and quantitative numeracy), from which a total score is computed. The TOFHLA has good psychometric properties and is frequently used to measure health literacy, 58 particularly in HIV+ populations. 58 –62 The TOFHLA total score was used for this study.
Medication beliefs
The Beliefs Related to Medications Survey (BERMA) is a 53-item self-report measure that assesses efficacy-related beliefs regarding medications, which may play a vital role in medication adherence. 63 Prior research supports the psychometric properties of the BERMA. 64 The three BERMA subscale scores were used: Medication Management Efficacy, Dealing with Health Professionals, and Attitudes About Medications.
Perceived stress
The Perceived Stress Scale-10 (PSS) is a 10-item self-report questionnaire that measures an individual's appraisal of stressful situations. 65,66 The measure has well-established psychometric properties with both NLW and Latinx populations. 67 The PSS total score was used in this study.
Medication adherence evaluation
The Medication Event Monitoring System (MEMS 68 ) was used to electronically measure adherence to HIV medications. At the first study visit, participants were given an MEMS medication bottle and cap containing a microchip to record the date and time of every bottle opening. MEMS is a well-validated measure of ART adherence in HIV. 21,69 –72
Participants used the MEMS to track one of their ART medications—either their protease inhibitor or their most frequently dosed nonprotease inhibitor. Participants were trained to use the MEMS as described by Bova et al. 73 Specifically, they were informed about the microchip recorder, instructed to only remove the designated dose at each opening, and told not to remove more than one dose of medication at a time (“pocket dosing”). Finally, they were trained to open and close the pill bottle properly so that the recording device was activated. Study staff transferred the selected ART medication into the MEMS bottle and taught participants to do this on their own, in case a medication refill occurred during the monitoring period. After training, the MEMS caps monitored participants' ART adherence for at least 30 days.
At the second study visit, conducted at least 30 days later, participants returned their MEMS device and completed a brief MEMS follow-up interview to ensure that it was used correctly during the monitoring period. MEMS data were then downloaded and analyzed. Each participant's overall adherence rate was calculated as the number of monitored doses taken during the 30-day monitoring period (subtracting any “pocket doses” or extra container openings reported by the participant during the MEMS follow-up interview) divided by the number of doses prescribed during that period. The dependent variable for the study analyses was the Total Adherence Score. In addition, we utilized the visual analog scale as a self-report measure of ART adherence. While this was not our measure of adherence for hypothesis testing, it was included to examine the association between self-report and electronic measurement of ART adherence. 68
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics Version 24. Most variables met homogeneity of variance assumptions and were normally distributed; variables that did not meet assumptions were analyzed using nonparametric tests or transformed as recommended by Field. 74 Plasma HIV viral loads were significantly positively skewed, and these variables were logarithmically transformed. In addition, as expected, medication adherence was significantly negatively skewed. When possible, nonparametric analyses (i.e., Spearman's correlations) were used to account for this. In all multivariable analyses utilizing parametric analyses [i.e., partial correlations, analysis of variance (ANCOVA), linear regressions], we transformed the Total Adherence Score variable by applying reverse (i.e., subtracting each score from 1+ the highest score obtained) and square root transformations. 75,76
Categorical variables were examined using chi-square. Independent-samples t-tests, Mann–Whitney U-tests, and ANCOVA were used to analyze group differences on continuous variables. Spearman's correlations were used to examine linear relationships between adherence and other variables, and linear regressions were used to compute overall models. In addition, covariates (i.e., age, education) were added to relevant analyses if a demographic variable demonstrated between-group ethnic differences and/or was related to the dependent variable. For instance, the WTAR was used as a covariate in the between-group ethnic comparisons of neurocognitive functioning, as measures of quality of education and literacy, such as the WTAR, are known to be significantly associated with neurocognitive test performance. 48 –50
Results
Sample overview
Overall, 46.5% of the sample was monitored on a single-pill combination ART, and the remaining 53.5% were monitored on either a protease inhibitor or their most frequently dosed nonprotease inhibitor. The sample's total adherence ranged from 9% to 100% {M = 83% (SD = 21.70); Mdn = 90.6% [interquartile range (IQR) = 17%]}. Less than half of the sample was adherent at the 90%+ rate (47.4%). Table 2 illustrates the demographic (i.e., age, education, gender), clinical (i.e., HIV, psychiatric, substance use), neurocognitive (i.e., average neurocognitive T-scores), and sociocultural (i.e., quality of education, SES, health literacy, medication beliefs, perceived stress) characteristics of the study sample. Herein we highlight the characteristics of the overall sample, between-group differences for the Latinx and NLW groups, and key bivariate correlations between the HIV-specific clinical and adherence variables to assess the validity of our adherence measure.
Demographic, Clinical, Neurocognitive, and Sociocultural Variables for the Study Sample and by Ethnicity
log10 transformed.
t-ratios for ethnicity based on comparisons for neurocognitive scores utilizing analysis of variance with Wechsler Test of Adult Reading as covariate.
Mann–Whitney U due to skewness of variable.
p < 0.05.
p < 0.01.
AMAS, Abbreviated Multidimensional Acculturation Scale; BDI-II, Beck Depression Inventory-II; BERMA, Beliefs Related To Medications; IQR, interquartile range; ISP, Index of Social Prestige; PSS, Perceived Stress Scale; TOFHLA, Test of Functional Health Literacy; WTAR, Wechsler Test of Adult Reading.
Demographic characteristics
On average, the sample was middle-aged and had approximately a high school level of education. The sample was primarily male and Latinx. Compared with the NLW group, the Latinx group was significantly younger and completed significantly fewer years of education (all ps < 0.01), and these variables were included as covariates in the between-group comparison of adherence. In addition, within the Latinx group, 81% identified as Caribbean (75% Puerto Rican, 5% Dominican, and 1% Cuban), 7% as Mexican, 7% as Central American, 4% as South American, and 1% as “Other Latinx subpopulation.”
Clinical characteristics
Participants had been diagnosed with HIV for a median of 17 years (IQR = 7.00) and 11% of the sample was immunosuppressed (based on current CD4 count <200). The Latinx group had significantly lower current CD4 count and higher current plasma HIV viral load compared with the NLW group (all ps < 0.05). However, the two groups did not significantly differ on nadir CD4 count (p > 0.10). In terms of psychiatric characteristics, average depressive symptomology (based on the BDI-II) fell within normal limits, and there were no ethnic group differences. Regarding recent substance use, the most prevalent recently used substances were tetrahydrocannabinol (THC) (30.5%), cocaine (14.1%), benzodiazepines (7.8%), and opiates (6.3%), as measured by urine toxicology. There were no ethnic group differences, with the exception of recent opiate use, in which NLW participants demonstrated greater recent use of opiates (p < 0.05).
Neurocognitive characteristics
Within the entire sample, average neurocognitive functioning fell within normal limits for global functioning and all domains, with the exception of learning and memory. Impairments in these areas appeared to be driven by learning and memory impairments in the Latinx group. There were no significant differences between the Latinx and NLW participants in the global or other neurocognitive domains after accounting for effects of quality of education (WTAR; all ps > 0.05).
Sociocultural characteristics
As illustrated in Table 2, compared with NLW participants, Latinx participants had significantly lower SES (i.e., Hollingshead ISP; p < 0.05), quality of education (i.e., WTAR; p < 0.01), and health literacy (i.e., TOFHLA total score, p < 0.01). There were no significant group differences in beliefs about medications (i.e., BERMA subscale scores) or perceived stress (i.e., PSS total score; all ps > 0.05). Within the Latinx sample, average US and Latinx acculturation scores fell in the high range suggesting that the Latinx sample was highly acculturated to both cultures and essentially bicultural.
Demographic, clinical, and sociocultural variables
Entire study sample analyses
As noted in Table 3, across the entire sample, we examined the relationship between urine toxicology test results and total adherence rates, and participants who tested positive for recent cocaine use had significantly lower adherence rates than those who tested negative for recent cocaine use (U = 539.00, p < 0.01). No significant differences were observed between those who tested positive or negative for recent use of any other illicit substances (all ps > 0.10).
Nonparametric Correlations and Mann–Whitney U-Tests Examining Total Adherence and Demographic, Clinical, and Sociocultural Variables for the Entire Study Sample and by Ethnic Group
p < 0.05.
p < 0.01.
AMAS, Abbreviated Multidimensional Acculturation Scale; BDI-II, Beck Depression Inventory-II; BERMA, Beliefs Related To Medications; ISP, Index of Social Prestige; PSS, Perceived Stress Scale; TOFHLA, Test of Functional Health Literacy; WTAR, Wechsler Test of Adult Reading.
We then examined associations between adherence and other study variables. These results revealed that higher adherence was also significantly positively correlated with greater perceived capacity for dealing with health professionals (BERMA-Health Professional subscale; rs = 0.18, p = 0.04). No other significant associations were observed between adherence and demographic, clinical, or any other sociocultural variables (all ps > 0.05). Thus, cocaine use and the BERMA-Health Professional subscale were added as covariates for the between-group comparison of adherence.
To examine the validity of our adherence measurement, we examined the correlations between our adherence measure (Total Adherence Score) and HIV clinical indices. The results revealed that higher adherence was positively correlated with current CD4 count (rs = 0.27, p < 0.01) and negatively correlated with current HIV viral load level (rs = −0.20, p = 0.03). Of note, our electronically measured adherence variable was also positively correlated with self-reported adherence (rs = 0.61, p < 0.01). The correlation between CD4 count and adherence was not significantly different between the Latinx group and the NLW group (Fisher's Z = 0.41, p > 0.05). However, the correlation between HIV viral load and adherence was significantly greater in the NLW group (rs = −0.67, p < 0.01) than in the Latinx group (rs = −0.23, p < 0.05; Fisher's Z = 2.67, p < 0.01).
Between-group ethnic comparisons
For descriptive purposes, Fig. 1 provides an overview of the mean adherence rates for the two groups, which indicated a small-to-medium effect size. To test the first hypothesis regarding ethnic differences in ART adherence, ANCOVA was computed to assess whether there was a significant difference between ethnic groups on total adherence after accounting for relevant covariates (i.e., age, education, recent cocaine use, and BERMA Health Professional subscale).
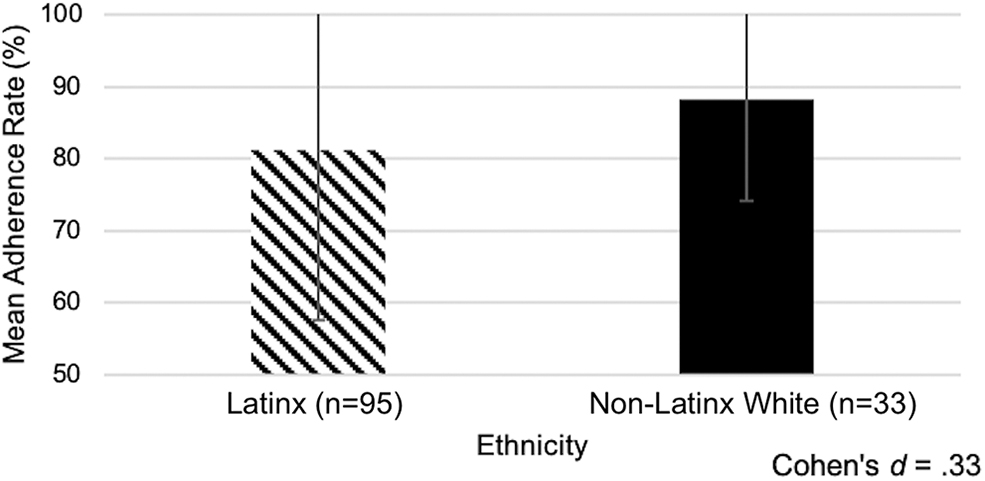
There was a significant effect of ethnicity on adherence rate. The Latinx group had significantly lower total adherence compared with the non-Latinx white group.
The results revealed that the model was significant (F(5,112) = 4.63, p < 0.001) and there was significant effect for ethnicity such that the Latinx group had significantly lower total adherence compared with the NLW group (F(1,112) = 4.21, p = 0.04). Next, the relationships between adherence with demographic and clinical characteristics within each of the ethnic groups were examined using separate bivariate correlations to test the second and third hypotheses.
Within-group Latinx analyses
As Table 3 illustrates, Latinx participants who tested positive for recent cocaine use had significantly lower adherence rates (Mdn = 80.55) than Latinx participants who tested negative (Mdn = 90.32; p < 0.05). Within the Latinx group, total adherence was significantly negatively correlated with US acculturation (i.e., AMAS Total US Acculturation) and self-reported stress (i.e., PSS total), such that better adherence was associated with lower US acculturation and self-reported stress (all ps < 0.05). Adherence was not significantly related to any other demographic, clinical, or sociocultural characteristic in this group (all ps > 0.05). In addition, within-group comparisons of adherence based on the country of origin were not computed due to the small sample sizes in all of the Latinx subgroups with the exception of the Puerto Rican group.
Within-group NLW analyses
As noted in Table 3, NLW participants who tested positive for recent cocaine use also had significantly lower adherence rates (Mdn = 82.06) than NLW participants who tested negative (Mdn = 93.74; p < 0.05). Within the NLW group, total adherence was significantly positively correlated with the BERMA “Dealing with Health Professionals” subscale (p = 0.03). Total adherence was not significantly related to any other demographic, clinical, or sociocultural characteristics in this group (all ps > 0.05).
Neurocognitive variables
A series of partial correlations were computed to examine the association between neurocognitive function and total adherence. Given the potential impact on neurocognitive test performance and its association with adherence, cocaine use was included as an additional covariate in the following analyses. In the Latinx group, the results revealed that total adherence was not significantly associated with any Neurocognitive Domain or the Global Neurocognitive Average T-scores (rs = 0.04–0.17; all ps > 0.10). In the NLW group, the results revealed that total adherence was significantly associated with the neurocognitive domains of Attention/Working Memory, Learning, and Memory (rs = 0.38–0.45; all ps < 0.05), such that better neurocognitive functioning was associated with better adherence. However, no other significant associations were observed with the Global or other neurocognitive domains (all ps > 0.10).
Multivariable models predicting adherence
Lastly, linear regressions were computed to examine the relationship between clinical, neurocognitive, and sociocultural variables with total adherence. Because significant predictors of adherence differed across ethnic groups, separate regression models were computed for the Latinx and NLW groups. Variables that were significantly associated with adherence, in the analyses above, were entered into each respective model.
For the Latinx group, recent cocaine use, AMAS Total US Acculturation score, and perceived stress (i.e., PSS score) were entered into the model. The results revealed that this model significantly accounted for 25.7% of the variance in adherence scores (F(3, 61) = 7.04, p < 0.001), and the results showed that all three variables significantly contributed to the model: recent cocaine use (B = 1.75, SE = 0.079, p = 0.03), AMAS Total US Acculturation (B = 0.25, SE = 0.08, p < 0.01), and perceived stress (B = 0.10, SE = 0.04, p = 0.03) were significant predictors of adherence. Overall, lack of recent cocaine use, lower US acculturation, and lower perceived stress predicted better adherence in the Latinx group.
For the NLW group, recent cocaine use, Attention/Working Memory, Learning, and Memory Domain T-scores, and BERMA-Health Professional subscale were entered into the model. The results revealed that this model significantly accounted for 49% of the variance in adherence (F(5, 31) = 5.09, p < 0.001), and the results showed that only recent cocaine use (B = 2.68, SE = 0.64, p < 0.001) was a significant predictor of adherence. Thus, lack of recent cocaine use predicted better adherence in the NLW group.
Discussion
This study sought to identify potential ethnic disparities in electronically measured ART adherence over a 1-month period and apply a biopsychosociocultural framework to understand how neurocognitive (e.g., learning, memory), sociocultural (i.e., acculturation, medication and health beliefs, perceived stress, SES, health literacy), and other factors (i.e., depressive symptomatology, cocaine use) relate to adherence in Latinx and NLW PLWH. The results revealed important ethnic differences in ART adherence, such that the Latinx PLWH demonstrated significantly worse adherence than the NLW PLWH. In general, predictors of adherence differed between the two ethnic groups, with one exception. In the Latinx group, sociocultural factors (i.e., lower US acculturation, lower perceived stress) predicted better adherence. In the NLW group, better neurocognitive functioning (i.e., learning, memory, attention/working memory) and only one sociocultural factor (better ability to deal with health professionals) predicted better adherence. However, recent cocaine use was a robust predictor of adherence for both groups, such that recent cocaine use at the baseline visit (as measured with urine toxicology) predicted worse adherence in the subsequent 30-day period.
Our finding that the Latinx group had significantly worse ART adherence compared with the NLW group extends the prior literature in important ways. First, this study supports the validity of prior studies that used self-report measures. 29 –32,53 Second, the current findings extend the Arnsten et al. 34 DOT findings on the increased risk for medication errors in Latinx PLWH by providing sociocultural data to better contextualize adherence behaviors in this population. Together, these converging findings suggest that ethnic disparities in adherence exist and Latinx PLWH are at increased risk for worse HIV health outcomes compared with NLW PLWH.
In fact, the current study results revealed that the Latinx group demonstrated significantly worse HIV-related clinical outcomes. Specifically, the Latinx group had significantly lower CD4 count and higher HIV viral load compared with the NLW group, suggesting greater disease progression and worse control of HIV viremia. While causal inferences cannot be made, worse ART adherence may be linked to the HIV-related health disparities (e.g., opportunistic infections, neuropathy, mortality, morbidity) observed in the Latinx PLWH population.
Further, the relationship between HIV viral load and total adherence was significantly stronger in the NLW group than the Latinx group, suggesting that ethnicity may modify the association between medication adherence and HIV viral load. Subsequently, understanding the underpinnings of adherence in this population at a granular level is imperative to effectively improve adherence and reduce HIV health disparities revealed in this and prior studies. 4 –11,29–32,34 To that end, a series of within-group analyses were conducted to better understand adherence in each ethnic group. Based on these results, a somewhat differential pattern of predictors of adherence emerged for the two groups.
In the Latinx group, two sociocultural factors (acculturation and perceived stress) and cocaine toxicology (discussed below) predicted adherence within our multivariate model. Contrary to our hypothesis and prior research, the current results showed that lower US acculturation was associated with better adherence. This was unexpected given that Robbins et al. 36 found that higher US acculturation was related to better adherence in a similar sample of PLWH. However, different measures of acculturation were used in the two studies, the AMAS 53 in the current study and the Bicultural Scale for Puerto Ricans in the Robbins et al. 36 study. The current results may be consistent with “negative acculturation” theory, which suggests that acculturation to the majority-dominant US culture involves greater adoption of American values, which can include behaviors that adversely affect health. 77,78 Research has shown that among Latinx individuals, higher levels of US acculturation are associated with poorer nutrition and dietary habits, worse perinatal outcomes (including low birth weight and prematurity), and increased substance use (particularly alcohol and nicotine use). 79 Therefore, the relationship between acculturation and adherence in this sample may suggest adoption of attitudes or behaviors from the majority culture that directly or indirectly reduce ART adherence.
In addition, lower perceived stress was also associated with better adherence in the Latinx group. This is consistent with prior studies reporting that stressors are associated with lower medication adherence, among other health outcomes. 80,81 The current findings provide support for a culturally tailored approach to adherence interventions that emphasizes the importance of medication adherence and highlight stress management as a potentially modifiable factor to improve adherence in this population.
It is also notable that within the Latinx group, neurocognitive functioning was not significantly associated with ART adherence. This finding was unexpected given the literature suggesting otherwise in NLW and African American populations. 21,22,27,28 However, given the fact that psychometrically sound normative data are generally available for neurocognitive tests for NLW and African American populations compared with the US-dwelling Latinx population, it is possible that normative data could have impacted the current results.
In the NLW group, bivariate analyses revealed that better neurocognitive functioning in learning, memory, attention/working memory, better ability to deal with health professionals, and lack of recent cocaine use predicted better adherence. However, the results of a multivariable analysis with all three of these variables included in the model revealed that only recent cocaine use significantly contributed to the model.
For both ethnic groups, cocaine use was significantly related to adherence such that recent cocaine use at the baseline visit predicted worse adherence in the subsequent 30 days. This is consistent with prior research showing that active substance use, particularly recent stimulant use, is associated with lower ART adherence in PLWH. 82 Studies have also shown that cocaine users had the lowest adherence rates, 83 and that the relationship between poor neurocognitive performance and lower medication adherence rates was partially mediated by cocaine use. 84 Thus, the current findings and prior literature suggest that assessment and treatment of substance use, and particularly cocaine use, should be an integral part of interventions to improve adherence in both Latinx and NLW PLWH.
Study strengths and limitations
The current study has several strengths that warrant consideration. This is the first large-scale study to focus on ART adherence in Latinx PLWH using MEMS, an electronic measure of adherence. Second, this is the first study to apply a comprehensive biopsychosociocultural theoretical framework to adherence in Latinx and NLW PLWH and utilized well-validated measures for all aspects of assessment. Further, by evaluating the relative importance of several predictors, such as acculturation and perceived stress, this work suggests that sociocultural factors, which are infrequently assessed in the literature, may play a more important role in adherence among Latinx individuals than the factors that are traditionally measured. Third, the sociocultural characteristics of the Latinx group were well characterized; the US Latinx population is highly heterogeneous, and including this information makes it clear for whom these findings are most generalizable (i.e., Latinx from Caribbean backgrounds). Fourth and finally, this study is of high clinical significance given that (1) the majority of Latinx participants were recruited from Spanish Harlem and the Bronx, areas with some of the highest rates of HIV infection and Latinx health disparities in the United States, 85,86 and (2) compared with other US-dwelling Latinx subpopulations (e.g., Mexican, Cuban), Puerto Ricans are at the greatest risk for HIV and experience worse HIV-related health outcomes. 7,87
Despite these study strengths, a number of study limitations also merit discussion. The NLW subsample was relatively small (n = 33), and this may have limited power for related within-group analyses. However, despite this limitation, the within-group linear regression analysis in this subsample still accounted for almost half of the variance in ART adherence.
Given the geographic location of the study and sample composition, the current findings may not be generalizable to suburban or rural populations, or other Latinx subpopulations. The study sample comes from an urban area (New York City) and the rate of optimal ART adherence was low, with only one-third of the sample demonstrating optimal adherence (90% ± adherence rate). Consistent with New York City demographics (particularly in Spanish Harlem and the Bronx, where the majority of study recruitment occurred), 81% of the Latinx group was Caribbean with the majority being Puerto Rican (75%), fluent in English, and highly acculturated to both US and Latinx cultures (or bicultural). 88 The Latinx group was also younger, had fewer years of education, and had lower literacy, health literacy, and SES compared with the NLW group. However, none of these factors was related to adherence in this study. Finally, HIV-1 RNA was drawn at only the first study visit. The absence of a follow-up HIV-1 RNA assessment precluded objective measurement of adherence through laboratory indicators.
Future research is needed to replicate the current findings with larger sample sizes and within different geographic regions (suburban, rural) and Latinx subpopulations. Future investigations should also include sociocultural measures, such as acculturation. Closer examination of potential barriers to adherence in Latinx PLWH is needed. Given that recent cocaine use was the only variable to significantly predict adherence in both Latinx and NLW participants, further research is needed to better understand how substance use and treatment can impact adherence interventions. Moreover, given the potential explanation of the “negative acculturation” theory, determining how stress may be related to acculturation, and how substance use may be related to acculturative stress (or adapting to US majority culture) is also an essential next step. Last, future research should investigate culturally tailored interventions to improve adherence in Latinx PLWH.
It is also important to note that the US Latinx population is heterogeneous and includes a variety of subpopulations (e.g., Caribbean, Mexican, Central American groups). These subpopulations have origins in countries with unique cultural characteristics that may be important to studies of adherence. In our study, the largest Latinx groups originated from Caribbean countries and included those who identify as Puerto Rican, Dominican, or Cuban. However, given that 75% of our Latinx sample identified as Puerto Rican, with much smaller percentages of other Latinx groups, we were not able to make within-group comparisons.
Future research should examine how these factors may differ across Latinx subgroups, particularly the relationship between acculturation and adherence. Prior research has found that compared with HIV+ Latinx adults in the United States, HIV+ Latinx adults born in Cuba and Puerto Rico were less likely to be connected to care within 3 months of diagnosis. Moreover, HIV+ Latinx adults who resided in neighborhoods with less than 25% Latinx were less likely to be connected to HIV care. 89 Thus, country of birth and neighborhood characteristics should also be considered when examining medication adherence and medical care engagement among HIV+ Latinx adults. 89
Finally, it is important to acknowledge the role of structural marginalization in perpetuating health disparities, such as those observed in HIV outcomes. Structural marginalization stems from the uneven institutional distribution of benefits and burdens to different groups of people. This marginalization extends to a wide range of social identities, such as race, ethnicity, gender, class, sexual orientation, HIV status, and SES. 90 Importantly, many of our participants have multiple marginalized social identities, which impacts not only their access to care but also treatment in health care systems at large. The consequences of systemic marginalization extend to health care behaviors, including medication adherence, and can go on to further perpetuate health disparities. This merits further investigation.
The present study results revealed important disparities in ART adherence and HIV-health outcomes such that Latinx PLWH demonstrated significantly worse adherence, immune function, and HIV viral suppression compared with their NLW counterparts. These disparities have immense social, economic, and public health implications in terms of risk for HIV transmission, opportunistic infections, mortality, and morbidity.
This study provides an initial step toward a better understanding of how cocaine use and sociocultural factors impact health behaviors, such as ART adherence, in a particularly vulnerable population through a comprehensive biopsychosociocultural framework. These findings suggest that poor ART adherence may be one pathway to worse HIV-health outcomes in Latinx PLWH. Culturally tailored adherence interventions that consider acculturation, substance use assessment/treatment, and stress management are warranted to improve outcomes and health equity.
Footnotes
Acknowledgments
The authors thank Drs. Susan Morgello (MHBB PI), Ana Abraído-Lanza, Julia Arnsten, Charles Hinkin, and Jane Simoni for their support of this project, and the participants. They would also like to thank the following research team members and community-based organizations for ensuring the success of this project: Erica D'Aquila, Ana Rosario, and Maria Pizzirusso, and Drs. Armando Fuentes, Caitlin Miranda, Jennifer Monzones, Kaori Kubo Germano, Kelly Coulehan, and Diane Scheiner as well as the Harlem Community Academic Partnership and the Manhatten HIV Care Network.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors would like to thank the Manhattan HIV Brain Bank (MHBB; Grant no.: U24MH100931). This research was supported by K23MH07971801 from the National Institutes of Health. MJS was supported by NSF award GRFP-G30328. AA was supported by NIH award SC2 MH118473. RNR was supported by NIH award P30 MH043520 (PI: Remien).