
Abstract
The lifetime use of combination antiretroviral therapy (cART) highlights the need to understand patterns of and factors associated with adherence to cART. In this cohort study using a 10% random sample of dispensing claims data for eligible Australians, we identified 2042 people dispensed cART between January 2016 and December 2017 (mean age 48.0 ± 12.0 years old, 88.6% male, and 85.9% treatment experienced). We considered people to be adherent if the proportion of treatment coverage days was ≥80% in the 360 days after their first observed cART dispensing. We also used group-based trajectory modeling (GBTM) to examine different patterns of adherence for 360 days from first observed cART dispensing. Most commonly, people receiving cART were treated with two nucleoside/nucleotide reverse transcriptase inhibitors with an integrase strand transfer inhibitors (INSTI—46.6%). Overall, 1708 people [83.6% (95% confidential interval 82.0–85.3%)] remained adherent over 360 days. GBTM identified three distinct adherence patterns: nearly always adherent [67.8% (63.7–71.9%) of the cohort], moderate adherence [26.6% (23.0–30.1%)], and low adherence [5.6% (4.1–7.2%)]. People were more likely to belong to the “nearly always adherent” trajectory if they were older (per additional year of age), treated with an INSTI regimen, and on treatment for more than 6 months. Our study demonstrates that the 360-day adherence to cART is generally high, but approximately one-third maintain a moderate or low adherence pattern. The use of INSTI regimens and additional support of treatment adherence, especially among younger people and those initiating therapy, may further improve adherence.
Introduction
Combination antiretroviral therapy (cART) is the cornerstone of HIV therapy as it prevents disease progression, improves quality of life, and eliminates the transmission risk when patients achieve undetectable viral load. Following the World Health Organization guidelines in 2015, 1 most countries now recommend initiating therapy for all patients irrespective of CD4 count or clinical stage, thus increasing the number of people eligible for treatment.
Adherence to cART is the main determinant of viral suppression, with a minimum adherence between 80% and 95% required to achieve success, depending on the therapeutic regimen. 2,3 However, maintaining optimal adherence (higher than 80–95%) in routine clinical practice is challenging, and meta-analyses have shown that only 62–70% of people with HIV achieve these adherence levels worldwide. 4 –6 Previous studies have also suggested some patients prescribed antiretrovirals may never initiate treatment (primary nonadherence), and some of those on therapy may experience treatment breaks or reduced adherence over time, highlighting the dynamic nature of adherence to therapy. 7,8 However, most of the previous adherence assessments have been performed cross-sectionally or cumulatively, providing incomplete information on risk factors and patterns of nonadherence.
The introduction of less toxic medicines with better tolerability profiles such as integrase strand transfer inhibitors (INSTI), and regimens with lower pill burden (i.e., single-tablet regimens) are likely to increase adherence. 9 Australian studies report an increase in the use of INSTI and single-tablet regimens, dispensed to over 55% of patients in 2016. 10,11 However, the population-level patterns of adherence to cART are still unknown.
To address this knowledge gap, this population-based study quantifies the rate of adherence at 360 days in people initiating or receiving on-going cART, describes adherence trajectories, and identifies factors associated with better adherence.
Methods
Setting and access to HIV medicines
All Australian residents are entitled to subsidized access to prescribed medicines through the Pharmaceutical Benefits Scheme (PBS). Medicines for HIV treatment are PBS subsidized and can be prescribed by specialists or general practitioners who have undertaken specific training. Patients can access their prescribed treatment through community, private, or public hospital pharmacies and may have to pay a capped co-payment, depending on their PBS beneficiary status.
Since July 2013, all dispensings of PBS-listed antiretrovirals are captured in the PBS data collection, meaning all antiretrovirals dispensed to outpatients and private hospital inpatients are captured. However, the PBS collection does not include antiretrovirals prescribed to public hospital inpatients, obtained through compassionate access or clinical trials, or paid in full by patients. 11,12 Antiretrovirals for pre-exposure prophylaxis (PreP) were listed on the PBS in 2018 and postexposure prophylaxis is not PBS funded.
Data source
The PBS 10% sample consists of the medicine dispensing history for a 10% random sample of PBS-eligible people, extracted based on the individual's randomly assigned unique ID. The PBS dataset contains information on the medicine dispensed, including the PBS item code, date of supply, date of prescription, and quantity dispensed.
Study design and cohort
We used the PBS 10% sample data for the period between January 1, 2013, and December 31, 2018, to identify all people ≥18 years of age dispensed antiretroviral agents between January 1, 2016, and December 31, 2017. We further restricted our cohort to people dispensed cART regimens, defined as having at least three antiretroviral agents in a 30-day window [nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), INSTIs, protease inhibitors (PI), or entry inhibitors (EI)]. The cART index date corresponded to the date of dispensing of the last medicine of the regimen occurring within this 30-day period. We followed patients for 360 days after the index date (Fig. 1). Table 1 contains details of all antiretroviral medicines included in our analysis.
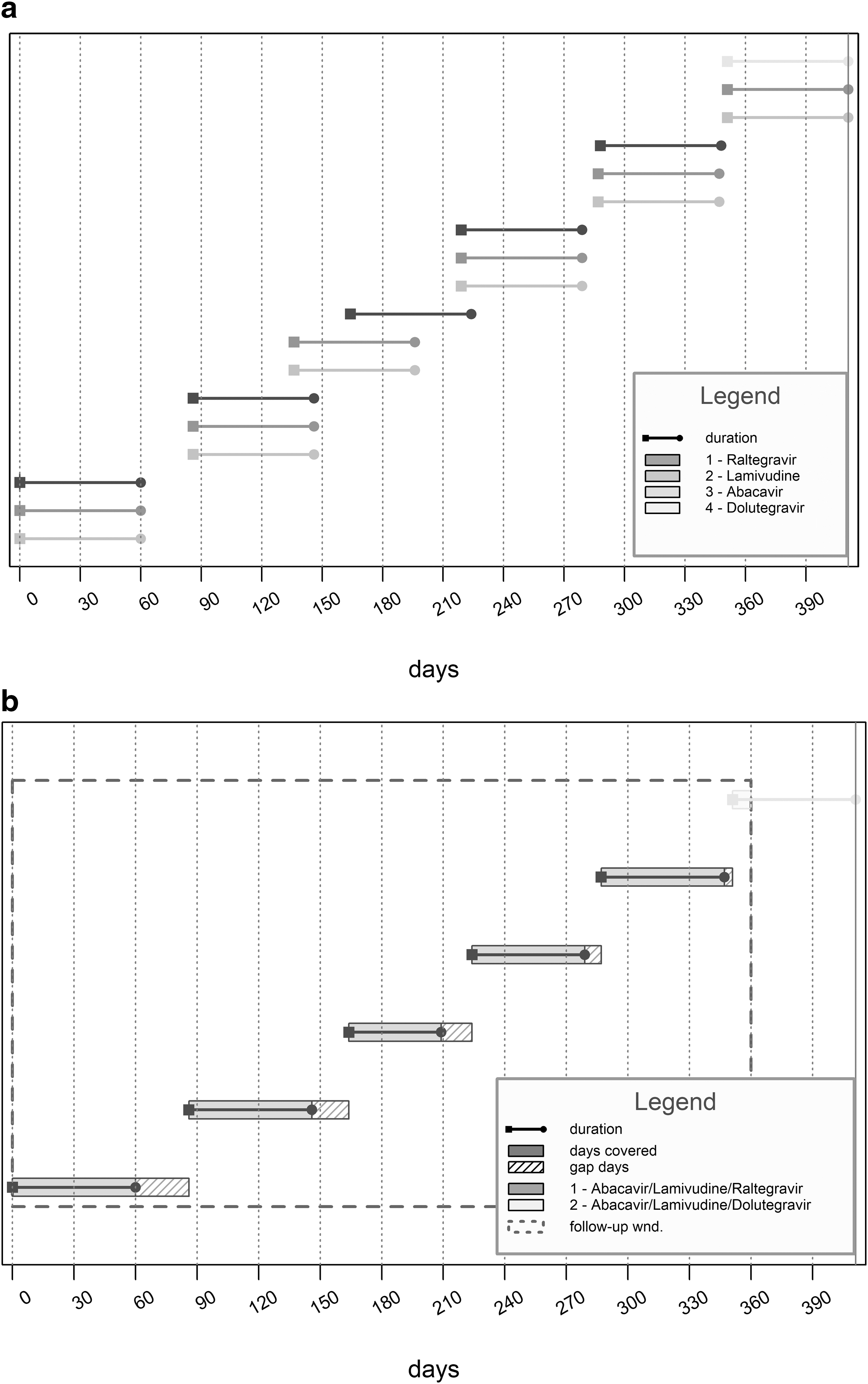
Antiretroviral regimens and duration according to dispensing records for one person.
Antiretroviral Medicines Evaluated by Generic Name and Item Code
Codes from the Pharmaceutical Benefits Scheme relevant to the study period (2013–2018). More details on each item code form and strength, pack size, and days of use are available upon request.
We assumed that the dispensing of three antiretroviral agents was indicative of treatment for HIV, 1 compared with one (tenofovir or lamivudine) for the treatment of hepatitis B and two (tenofovir and emtricitabine) for PreP, or other dual therapies recommended for HIV patients in specific clinical situations. Therefore, we excluded patients who received only tenofovir or lamivudine during the study period and those who received less than three antiretroviral agents in their first dispensing.
We defined the characteristics of patients at the index date by sex, age, state of the pharmacy where the cART was filled, antiretroviral components of the cART regimen, cART class (NRTI, NNRTI, INSTI, EI, and PI), cART regimen type (single or multi-tablet), treatment status (naive or experienced), and dispensing of medicines for mental health disorders, defined below.
We classified the cART regimen type as single tablet if the patient was dispensed one of the following: Atripla® (tenofovir disoproxil fumarate/emtricitabine/efavirenz), Eviplera® (tenofovir disoproxil fumarate/emtricitabine/rilpivirine), Stribild® (tenofovir disoproxil fumarate/emtricitabine/elvitegravir/cobicistat), Triumeq® (abacavir/lamivudine/dolutegravir), Genvoya® (tenofovir alafenamide/emtricitabine/elvitegravir/cobicistat), or Odefsey® (tenofovir alafenamide/emtricitabine/rilpivirine). All regimens involving the dispensing of multiple tablets, even if one was a single-tablet regimen, were classified as multi-tablet. We used a 3-year period before the index date to evaluate prior antiretroviral exposure, defining naive patients as those with no antiretroviral dispensing in this period. We further classified experienced patients according to the length of time on the current cART regimen (≤6 vs. >6 months).
We evaluated prior dispensing of psychotropic medicines as a proxy of mental health disorders, consisting of the occurrence of at least two dispensings of medicines of the WHO Anatomical Therapeutical Classification (ATC) groups 13 N05A (antipsychotics), N05B (anxiolytics), or N06A (antidepressants) in the 6 months before the index date.
Outcome measures
Our outcome of interest was adherence to cART. We defined adherence using the proportion of days covered (PDC), calculated as the total number of days that a patient had access to all components of their cART regimen (i.e., overlapping days of use of at least three antiretroviral agents, with exception of the enhancer's ritonavir and cobicistat) divided by the total time period (Fig. 1). 14 Thus, we considered a noncovered day whenever a patient had received two or fewer antiretroviral agents.
For single-tablet regimens, we assumed patients were taking the pills once daily. For multi-tablet regimens, we considered the size of the packs (median 30 days), the quantity dispensed, and the recommended doses according to the Australian Clinical guidelines 15 to obtain the duration of each component of the regimen. Refills occurring before the expected date of refill (i.e., before ending the stock of medicines in the participant's possession) were carried forward to subsequent periods.
We considered the adherence threshold of 80% as optimal adherence, as recent studies evaluating more contemporary regimens reported an absence of difference between this and higher levels of adherence in relationship to their capacity to predict viral suppression. 6 In addition, we evaluated treatment interruptions, defined as cessation of a complete cART regimen for >30 consecutive days and subsequent recommencement. 16
Statistical analysis
We conducted a descriptive analysis and compared categorical variables using the χ 2 test or the exact Fisher test and continuous variables using the nonparametric Kruskall-Wallis test. We calculated adherence assigning people to the cART regimen dispensed in the index date even if they had switched therapy during the follow-up.
We measured adherence in two different ways: first, we calculated PDC over the entire year; and second, we calculated PDC over 12 (30-day) intervals. For the cumulative period, we classified people as adherent if they had cART coverage for at least 80% of the days (288 of 360 days). For each 30-day interval, we classified people as adherent if they had cART coverage for ≥24 days to allow the construction of trajectories using group-based trajectory modeling (GBTM). 17
GBTM clusters people based on similar adherence behaviors and has been used previously to identify groups of people and factors associated with belonging to each group. 17,18 We selected the number of trajectory groups based on interpretability, reasonable size of groups, and lower Bayesian information criteria. The probability of adherence over time was modeled as a quadratic polynomial function. We assessed model adequacy as ensuring that the average of the posterior probabilities of group membership for individuals assigned to each group exceeds a minimum threshold of 0.7. 17
We evaluated baseline characteristics associated with group membership using multivariable logistic regression analysis, comparing the probability of belonging to each adherence trajectory group with all other trajectories combined as the reference. We included independent variables in the models based on their clinical relevance to influence adherence: sex, age, cART regimen, treatment status, and prior use of medicines for mental health disorders. We did not include the type of cART (single vs. multi-tablet) in the model because this variable was very strongly correlated to the dispensed regimen and some regimens were only available as multi-tablet regimens.
We performed statistical analysis using SAS® software version 9.4 (SAS Institute, Inc., Cary, NC) using the PROC TRAJ macro. The graphs were developed using the packages “AdhereR,” “ggplot2,” and “forestplot” from the R Foundation for Statistical Computing Program 3.6.0 version (R Core Team 2017, Vienna, Austria).
Sensitivity analysis
We evaluated the impact of a change in our adherence definition by allowing a 3-day window between refills (grace period). This time frame has been used previously to account for the fact patients may not fill all their treatment prescriptions on the same day. 19,20 We also used an alternate definition of adherence where people had to have access to at least one antiretroviral (rather than three at the same time), to provide upper estimates for adherence. Finally, we censored patients after the end of supply days of their last antiretroviral dispensing in the 360-day period to evaluate the impact of loss to follow-up.
Ethics and data access approval
This study was approved by the New South Wales Population and Health Services Research Ethics Committee (Approval Number: 2013/11/494) and data access was granted by the Australian Department of Human Services (DHS) External Request Evaluation Committee.
Results
We identified 2042 people receiving cART (dispensed three or more antiretroviral therapies) between Jan 2016 and Dec 2017 (Fig. 2).

Diagram of cohort selection.
Cohort characteristics
Most patients were male (88.6%), the mean age was 48.0 years (standard deviation 12.0), with 42.9% over 50 years of age, and ranging from 18 to 83. Approximately 40% of people had their first dispensing in New South Wales, followed by Victoria (28.6%), Queensland (17.8%), and Western Australia (7.6%). There were 384 (18.8%) people dispensed medicines for mental health disorders in the 6 months before the index date (Table 2).
Cohort Characteristics, 2016–2017 (N = 2042)
Antipsychotics (N05A), anxiolytics (N05B), or antidepressants (N06A).
cART, combination antiretroviral therapy; EI, entry inhibitors; INSTI, integrase strand transfer inhibitors; NRTI, nucleoside/nucleotide reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
cART regimens exposure
Most people were first dispensed a single-tablet regimen (56.4%), used the backbone of 2 NRTI plus an INSTI (46.6%), NNRTI (34.6%), or PI (8.3%), and were treatment experienced with more than 6 months on the current cART regimen (75.2%) (Table 2). Tenofovir plus emtricitabine or lamivudine was the most common regimen backbone (64.3%, n = 1313), followed by abacavir plus lamivudine (28.1%, n = 573) and zidovudine plus lamivudine (1.5%, n = 31).
We identified 160 different combinations of antiretrovirals of which 10 were used by more than 80% of the patients. Almost one-fifth of the patients were using abacavir, lamivudine, and dolutegravir, which was the most common combination (Table 3).
The 10 Most Commonly Used Antiretroviral Combinations (N = 1639)
Represents 80.3% of patients.
EI, entry inhibitors; INSTI, integrase strand transfer inhibitors; NRTI, nucleoside/nucleotide reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
During the follow-up, 13 (0.6%) patients died and 271 (13.3%) patients switched their cART regimen class. The most common switching was to a 2 NRTI + INSTI (73.1%, n = 198), from NNRTI (48.7%, n = 132), PI (17.3%, n = 47), or other combinations.
Adherence to cART
Overall, 1708 people [83.6% (95% confidential interval—95% CI 82.0–85.3%)] remained adherent after 360 days, with a median PDC equal to 96.4% (interquartile range 87.2–99.7%), meaning half people had 347 days of cART available within the 360 days.
Our GBTM identified three distinct adherence trajectories over 360 days: people in the “nearly always adherent” group comprised 67.8% of the cohort [95% confidence interval (63.7–71.9%)], 26.6% (23.0–30.1%) of the cohort were in the “moderately adherent” group, and the remaining 5.6% (4.1–7.2%) of the cohort were belonged to the “low adherence” group (Fig. 3).

Group-based trajectory analysis of adherence during the follow-up. The solid line represents the predicted probability of adherence in each group. The dashed line represents the observed proportion of people adherent in each group.
As expected, most people classified as adherent after 360 days belonged to the nearly always adherent group (82.8%), also the highest median PDC among the three trajectory groups (98.9%). Treatment interruptions occurred among 22.5% (n = 460) peoples and were more common among those belonging to the moderate and low adherence groups. In addition, people in the “low adherence” group were less likely to use single-tablet regimens and 2 NRTI + INSTI regimens, and to be experienced people with longer length of time on the current cART (Table 4). They were also more likely to have died (6.7%, n = 8, p < 0.001) or have only one dispensing within the follow-up period (20.0%, n = 24, p < 0.001).
Characteristics of People by Adherence Trajectory (N = 2042)
χ 2 test.
Antipsychotics (N05A), anxiolytics (N05B), or antidepressants (N06A).
Exact Fisher test.
Kruskall-Wallis test.
cART, combination antiretroviral therapy; INSTI, integrase strand transfer inhibitors; IQR, interquartile range; NRTI, nucleoside/nucleotide reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
Factors associated with adherence trajectories
The characteristics associated with a higher probability of belonging to the “nearly always adherent” group included older age (per additional year of age, p < 0.001), the use of 2 NRTIs + INSTI regimens compared to 2 NRTI + PI (p = 0.007), EI/etravirine-based regimens (p = 0.005) or other regimens (p = 0.048), and more than 6 month of cART on their current regimen (p < 0.006) (Fig. 4).

Results of logistic regression model predicting the probability of membership in the nearly always adherent group according to patient and treatment characteristics. Reference groups: *2 NRTI + INSTI; **Experienced patients on current combination antiretroviral therapy for more than 6 months. Prior use of medicines for mental disorders: antipsychotics (N05A), anxiolytics (N05B), or antidepressants (N06A). EI, entry inhibitors; INSTI, integrase strand transfer inhibitors; NRTI, nucleoside/nucleotide reverse transcriptase inhibitors; NNRTI, non-nucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
Sensitivity analysis
We found that introducing a 3-day grace period had little impact on study outcomes, with an overall proportion of adherent patients of 84.8% (95% CI 83.2–86.3%). The trajectory groups showed the same pattern and distribution: nearly always adherent [73.8% (71.1–76.5%)], moderate adherence [23.6% (20.9–26.2%)], and low adherence [2.64% (1.9–3.4%)]. Using a definition of adherence based on the use of at least one antiretroviral increased the overall proportion of adherent patients to 85.5% (84.0–87.0%), with similar trajectory patterns [72.1% (68.9–75.3%), 24.8% (21.8–27.8%), and 3.1% (2.2–4.0%) for groups 1, 2, and 3, respectively]. Finally, censoring patients increased the overall proportion of adherent patients to 87.5% (86.1–89.0%), and the trajectory patterns included the following groups: perfect adherence [28.4% (23.9–32.9%), moderate to high adherence [57.5% (53.6–61.3%)], and low adherence [14.1% (11.0–17.3%)].
Discussion
This is the first study, to our knowledge, to assess cART adherence patterns in a nationally representative sample of Australians. Our study, using two different measures of adherence, demonstrated that while adherence was generally high, almost one in six people experienced suboptimal adherence, and one third had moderate or low adherence patterns over 360 days. Our study also identified older age, been treated with an INSTI regimen, and on treatment for more than 6 months to be associated with a higher probability of belonging to the “nearly always adherent” group.
Interestingly, we observed a difference between the estimated rates of adherence and the viral suppression rates among adults on cART in Australia, which ranged between 93% and 95% in the years 2016–17 based on data from over 4500 patients attending 31 sites throughout the country (hospitals, general practitioner, and sexual health clinics). 21 These estimates are corroborated by other studies reporting high levels (89–94.5%) of virological suppression in the country. 7,22,23 So how should we best explain this apparent discrepancy?
First, it may be possible that our study underestimates adherence. Although it is the first use of PBS dispensing records to evaluate adherence to HIV treatment in Australia, this approach has been used previously in other countries in the HIV context, with adherence rates ranging between 19.7% and 68.3% when considering 80% of PDC as threshold. 24 –28 Nevertheless, our method yielded similar results to previous studies using self-reported measures, where ∼85% of patients achieved optimal levels of adherence to cART in Australia. 23,29 –31 Second, it may be that some “nonadherence” patterns may mask or not be associated with high rates of treatment failure. An example of one such pattern might include patients who take unplanned (or undisclosed to their clinician) treatment interruptions and reinitiate treatment in advance of their clinical visit and viral load measurement. There are data in Australia to suggest that this has happened in the past, attributed to clinical (e.g., side effects) or lifestyle reasons (e.g., travelling, clean out the system, and financial burden) closely related to the overall health of patients. 7,16,23,31,32 Third, it may be that newer cART combinations are much more tolerant of nonadherence than previously suspected. For instance, preliminary results from a clinical trial showed that taking cART four times per week produced similar rates of viral suppression as seven times per week. 33
Despite all the advances in cART therapy, a high proportion of patients (21–46%) have difficulties remembering to take their medicines every day 23,34 or stop cART (24–43.5%) at some point. 7,23,31,34 Approximately 27% of our study cohort were “moderately adherent,” which was associated with a high rate of treatment interruptions in this group. Although we cannot evaluate the reasons for, or appropriateness of, these interruptions, these results reinforce the need to better understand adherence behaviors over time. We observed the greatest reductions in adherence between 2 and 4 months after the first observed dispensing, 8 suggesting the first few months are key to maintain adherence among people initiating or switching therapy.
Our study also identified age, cART regimen, and treatment status to be factors associated with the probability of belonging to different adherence trajectory groups. Consistent with previous studies, older age was associated with a higher probability of adherence. 19,35 –37 Young people living with HIV are more prone to depression, low social support, and report conflicting commitments to long-term use of medicines. 38,39
Regarding the cART regimens, patients using 2 NRTI + INSTI had a higher probability of belonging to the nearly always adherent group compared to most other regimens. The use of INSTI is associated with lower rates of adverse drug reactions, 25,40 a well-known factor related to adherence. Their good tolerability and safety profile, low occurrence of drug interactions, high barrier to viral resistance, and better virological efficacy posed these medicines as the first-line therapy to HIV worldwide, while also been used in treatment-experienced patients. 40 In contrast, PI regimens are associated with a greater number of adverse drug reactions and higher susceptibility to drug-to-drug interactions. In addition, these regimens are sometimes taken more than once daily, increasing treatment burden and potentially contributing to poorer adherence. 24,25 Moreover, they are prone to prescription bias, as PI regimens may be preferred in potentially nonadherent patients due to its higher barrier to antiretroviral resistance or as part of second-line regimens in patients who have previously failed treatment due to nonadherence. 15 Finally, etravirine and EI regimens are salvage therapies 15 and can indicate both the therapeutic failure to previous regimens and a previous profile of nonadherence, being markers of worse prognosis.
Experienced patients with longer time on the current cART regimen had a higher probability of belonging to the “nearly always adherent” group compared to experienced patients with a shorter time on cART. This can reflect their adaptation to the current regimen, where most of the adverse events related to cART or treatment failures (if any) may have been already managed. Previous studies have reported a higher probability of adherence among experienced patients 5 and its increase over time, 37 suggesting that people initiating or switching therapies should have additional support.
Measuring adherence to multiple medicines using claims data is challenging. The PDC may be estimated considering the overlapping days of all medicines of interest, a minimum number of medicines, or exposure to each component separately. 41 We decided to adopt a more conservative approach considering the consequence of nonadherence in the context of HIV, while also testing less conservative definitions; these sensitivity analyses had little impact on our study findings. However, antiretroviral dispensing records are a proxy for the consumption of cART by the patients, and other adherence measures may be more accurate to assess the simultaneous use of all components of cART.
Our study has some limitations. Antiretroviral dispensing for public hospital inpatients or unsubsidized therapy is not captured by PBS data, 11,12 meaning that our study may underestimate actual adherence in Australian patients living with HIV. In addition, we used guideline-recommended dosing and pack sizes to calculate treatment duration, which can vary across individual patients. Finally, because the data are collected for administrative purposes, rather than research, and for privacy reasons, limited patient characteristics are available. Given the PBS claims were not linked to clinical information at the individual level, we could not evaluate other factors known to be associated with adherence, such as ethnicity and substance use, nor the impact of nonadherence on virological and immunological outcomes. Despite these methodological limitations, our study provides a comprehensive, whole of population perspective of Australian adherence patterns; this evidence has the potential to inform pharmaceutical policy and interventions to increase adherence in routine clinical care.
Our study demonstrates that while most Australians taking cART are adherent, approximately one in six experience suboptimal adherence over 360 days, and one-third maintain a moderate or low adherence pattern, potentially affecting clinical outcomes. Adherence is likely to improve by using INSTI regimens and with more intensive support, especially among younger people, and those in the early months of a new treatment regimen.
We acknowledge, however, that adherence to therapy is a relatively small part of the challenges people living with HIV may have staying engaged in care. A range of factors has been identified among Australian patients and clinicians as barriers to adherence and retention, from electronic systems that do not track patients throughout the health system to cultural and identity barriers that may impact on access to health services and trust in clinicians. 7,29,42 While our study focuses mostly on patient and cART characteristics, strategies to increase adherence to therapy and healthcare should embrace a broader spectrum of clinical, social, economic, and cultural factors.
Footnotes
Acknowledgments
We thank the Department of Human Services for providing the data.
Contributors
J.O.C., A.L.S., S.W.N., and S.-A.P. conceived and designed the study. R.G. and N.A.M. contributed to the study design. J.O.C. conducted the statistical analysis. A.L.S., M.L., and H.M. contributed to statistical analysis. J.O.C., N.A.M., and S.A.P. drafted the initial article. All authors contributed to the interpretation of results and critical revision of relevant content. All authors commented on drafts and approved the final version for publication.
Author Disclosure Statement
S.A.P. is a member of the Drug Utilisation Sub-Committee of the Pharmaceutical Benefits Advisory Committee. The views expressed in this article do not represent those of the committee.
Funding Information
This research is supported by the National Health and Medical Research Council (NHMRC) Centre of Research Excellence in Medicines and Ageing (ID: 1060407) and a Cooperative Research Centre Project (CRC-P) Grant from the Australian Government Department of Industry, Innovation and Science (ID: CRC-P-439). JOC received a PhD visiting student scholarship from the CAPES Foundation (Process 88881.188410/2018-01) and an Endeavor Research Fellowship from the Australia Awards-Endeavour Scholarships and Fellowships. A.L.S. is supported by an NHMRC Early Career Fellowship (ID: 1158763).