
Abstract
Resilience is defined as the ability and process to transform adversity into opportunities for growth and adaptation. Resilience may be especially important for people living with HIV (PLWH), who are susceptible to anxiety and depressive disorders, which are commonly linked to risk behaviors (i.e., alcohol and drug abuse), poor adherence to medical regimens, increased risk of morbidity and mortality, and related stigma and discrimination. To date, few studies have examined the impact of resilience on health-related behaviors and outcomes among PLWH, particularly among minority women living with HIV (WLWH) who are dealing with multiple stressors impacting their health. This study used a convergent parallel mixed-methods design to collect, analyze, and integrate qualitative and quantitative data from a subsample of WLWH enrolled in the Women's Interagency HIV Study (WIHS). The aims of the study were to (1) qualitatively examine the resilience perspectives of 76 marginalized WLWH, and; (2) quantitatively assess the associations of resilience with HIV health outcomes—adherence to antiretroviral therapy and viral suppression—in the context of differing levels of internalized HIV-related stigma and depressive symptoms (n = 420). Findings from this mixed-methods study suggest that resilience is an important resource that can aid WLWH in coping constructively with adversity by capitalizing on intrapersonal traits and states, interpersonal and institutional resources, and spiritual and/or religious practices. Given the complex medical and social needs of marginalized WLWH, intervention strategies should focus on mitigating psychosocial burdens of stigma and depression, in addition to building resilience.
Introduction
Resilience is the ability to positively cope, adapt, and function despite experiences of adversity, trauma, tragedy, threats, or sources of stress. 1 Resilience has been characterized as a personality trait, a process, or an outcome that influences one's ability to function adaptively after a traumatic experience. 2 More recent work emphasizes the importance of developing multi-level approaches to locate the source of resilience; empower resilience within marginalized and other at-risk populations; and elucidate epigenetic, socioecological, and neurobiological mechanisms to predict individuals' ability to both be and become resilient. 3 Several well-evidenced psychosocial resilience-building strategies have been identified, including (1) active coping (i.e., problem solving, planning); (2) hardiness (commitment, control, and challenge); (3) optimism; (4) positive emotions; (5) religious coping; (6) self-esteem; (7) self-efficacy; and (8) social support. 4
Recognizing that health is influenced by a complex interplay of factors at multiple levels (i.e., intrapersonal, interpersonal, societal/policy 5 ), an emerging body of literature highlights the importance of investigating determinants of resilience in various social contexts and populations. 6 –8 People living with HIV (PLWH) are susceptible to anxiety and depressive disorders, which have been linked to risk behaviors (i.e., alcohol and drug abuse), poor adherence to medical regimens, and increased risk of morbidity and mortality. 9,10 In addition to these concomitant factors, PLWH contend with other major social stressors such as HIV-related stigma and discrimination. 11 –13 Thus, resilience may be especially important for people living with chronic, stressful, and burdensome health conditions, such as HIV infection, requiring lifelong self-management. 9
Increasing evidence suggests that resilience may serve as an especially important resource for marginalized or vulnerable populations, such as women living with HIV (WLWH). WLWH are vulnerable to adverse health outcomes associated with HIV disease, including elevated viral loads resulting from poor adherence to antiretroviral therapy (ART), and this relationship is magnified for WLWH who are a part of a racial/ethnic minority group. 14 In an effort to explore the biopsychosocial burden of intersectional stigma arising from living with HIV and belonging to another marginalized group or identity (e.g., race, gender, class, disability status), 15 a promising wellspring of research has emerged documenting the experiences of African American WLWH. 16,17 Several studies conducted by Dale et al., among samples of predominately African American WLWH, found higher resilience to be associated with lower depressive symptoms, higher quality of life, undetectable viral load, higher ART adherence, and lower gender-related coping. 18 –20 Qualitative work by Smith et al. may help explain some of the resilience-related associations by highlighting that resilience may be especially protective for African American WLWH. 21 Despite the adverse circumstances faced by many African American WLWH in their sample, many women not only found constructive ways to live with HIV but ultimately achieved a higher state of self-actualization (e.g., self-acceptance, autonomy, a feeling of purpose or mission in life) as well. 22
Taken together, these findings suggest that, if African American WLWH (and other marginalized or vulnerable groups) lack strategies to deal and cope with stressors associated with both the HIV experience and concomitant life challenges, resilience-building processes may act as a psychological salve to transform these lifelong obstacles. However, the impact of depressive symptoms on the protective potential of psychological resilience on the HIV experience is underexplored. With the ultimate goal of developing and implementing resilience-building interventions with and for WLWH, this study seeks to qualitatively and quantitatively measure and explore how psychological resilience, psychopathology (e.g., depression), and HIV intersect within a social context of marginalization (e.g., stigma) in society.
The aims of the study were to (1) qualitatively examine resilience strategies used to cope with stressors and challenges from the perspectives of 76 marginalized WLWH in four different geographic locations, and (2) quantitatively assess the associations of resilience with HIV health outcomes—adherence to ART and viral suppression—in the context of differing levels of internalized HIV-related stigma and depressive symptoms (n = 420). Findings have the potential to inform tailored resilience strategies to optimize the overall health and well-being of WLWH.
Methods
This study consisted of a secondary analysis of qualitative and quantitative data collected from a subsample of WLWH enrolled in the Women's Interagency HIV Study (WIHS). Established in 1993, WIHS is a multi-center, prospective, observational cohort study of women living in the United States who are either HIV infected or at risk of HIV acquisition. 23,24 The WIHS examines various topics, including the epidemiology of HIV, disease progression, treatment use and outcomes, and comorbidities among US residents with HIV. 23,24 This study utilized data collected from WIHS participants in Birmingham, AL—Jackson, MS, Atlanta, GA, and San Francisco, CA enrolled in the Women's Adherence and Visit Engagement (WAVE) substudy. 24 The WAVE study employed a mixed-methods approach to collect, analyze, and integrate qualitative interviews and quantitative survey data to examine how HIV-related and other intersecting stigmas affect adherence to HIV treatment recommendations and HIV clinical outcomes among WLWH. 25 All participants provided written informed consent, and study procedures were approved by the WIHS Executive Committee and the associated WIHS site Institutional Review Boards.
Qualitative phase
Qualitative interviews
Qualitative interviews were conducted between June and December 2015 with 76 WLWH enrolled in the qualitative phase of the WAVE substudy. Eligible participants for both study phases were WLWH enrolled in the WIHS cohort study, ≥18 years of age, English speaking, and able to provide written informed consent. Interviews lasted ∼73 min and were conducted in private rooms by female researchers (3 black, 3 white, and 1 mixed race/ethnicity) trained in qualitative interviewing techniques and explored the following: (1) the influence of stressors and challenges on women's overall health and well-being and (2) the role of positive coping mechanisms and resilience strategies to combat adversity. Sample questions specific to resilience included the following: “How do you cope or manage some of these experiences?” “What gives you strength?” and “What keeps you going every day?” To compensate women for their time and participation in the study, each participant received $30. Full details of the qualitative parent study, including results on other related themes, are described elsewhere. 15
Quantitative phase
Validated questionnaires were administered cross-sectionally to 420 women enrolled in the WAVE substudy from 2016 to 2017. 25 The following constructs were assessed.
Internalized HIV-related stigma
This was assessed with the negative self-image subscale of the revised HIV Stigma Scale (range 1–4), which consists of seven items (e.g., “I feel I'm not as good as others because I have HIV.”) rated on a four-point scale (strongly disagree to strongly agree), with higher values indicating higher internalized stigma. 26,27
ART adherence
ART adherence was assessed by asking participants to self-report how often they took their HIV medication(s) as prescribed over the past 6 months. Response options were “100% of the time,” “95–99% of the time,” “75–94% of the time,” “<75% of the time,” and “I haven't taken any of my prescribed medications.” As in previous studies, 18,28 we used the 95% cutoff for optimal versus suboptimal adherence.
Depressive symptoms
Depressive symptoms were assessed in WIHS using the 20-item Center for Epidemiological Studies Depression (CES-D) scale. 29 Possible range of scores is 0–60, with the higher scores indicating the presence of more symptomatology. Sample questions include the following: “I was bothered by things that usually don't bother me” and “I could not get going.” Response options were rarely (<1 day), some (1–2 days), occasionally (3–4 days), and most (5–7 days).
Resilience
We assessed resilience using the six-item Brief Resilience Scale. 30 Items include the following: “I tend to bounce back quickly after hard times,” “I have a hard time making it through stressful events,” “It does not take me long to recover from a stressful event,” “It is hard for me to snap back when something bad happens,” “I usually come through difficult times with little trouble,” and “I tend to take a long time to get over set-backs in my life.” Items were rated on a five-point scale (strongly disagree to strongly agree) with higher scores indicating higher resilience.
Viral load
WIHS conducts blood draws at every visit for assessment of HIV RNA viral load. Viral load was dichotomized as undetectable versus detectable using a cutoff value of 20 copies per milliliter.
Demographics
Participants also self-reported their age, education, income, time on ART, illicit drug use, and race/ethnicity (Table 1).
Sociodemographic and Health Characteristics of Women Living with HIV in the United States by Mode of Study Participation
ART, antiretroviral therapy; GED, general equivalency diploma; SD, standard deviation.
Data missing for some participants.
Data analysis and integration
Qualitative analytical methods
Qualitative interviews were audio recorded, transcribed, and analyzed by an established coding team employing both inductive and deductive strategies using thematic analysis methods in Dedoose. 31,32 Key themes and quotes around resilience and related strategies among WLWH were characterized through an iterative coding process based on concepts from theory, the extant literature, and the current data and summarized (Table 2).
Key Themes and Quotes Around Resilience Among Women Living with HIV
Quantitative analytical methods
We assessed demographic and health characteristics of the sample using descriptive analyses. Multivariable logistic regressions were conducted adjusting for age, race/ethnicity, education, illicit drug use, and time on ART to examine the main effects of resilience as well as the interaction effects of resilience with depressive symptoms and with internalized HIV-related stigma on ART adherence and on viral suppression. For significant interaction effects, we examined and depicted simple slopes at one standard deviation (SD) above and below the mean of each moderator. All statistical models were performed in SPSS with a cutoff p value of 0.05 and 95% confidence intervals (CIs) for statistically significant results.
Integration
This study employed a convergent parallel mixed-methods design where qualitative and quantitative data were integrated during the interpretation phase. 33 After independent analysis of both datasets, the investigative team examined the quantitative and qualitative data sources concurrently by comparing results through procedures such as side-by-side comparison in a discussion. 34 The team then examined the findings that emerged from each method and identified areas where the findings converged, diverged, or added insight to one another to inform study conclusions. Both data sources aided in establishing a more complete and robust understanding of resilience among WLWH by obtaining different, but complementary data.
Results
Qualitative participant characteristics
Participants were enrolled from four WIHS sites. Approximately two-thirds of participants were recruited from the San Francisco, CA and Atlanta, GA WIHS sites. The remaining participants were recruited from the combined Birmingham, AL/Jackson, MS WIHS site (Table 1). The mean age of women was ∼50 years, with the majority of women identifying as non-Hispanic black (59% of interviewees) and reporting an average yearly income of $12,000 or less (57% of interviewees).
Quantitative participant characteristics
Participants were enrolled from the same four WIHS sites. Approximately two-thirds of participants were recruited from the San Francisco, CA and Atlanta, GA WIHS sites. The remaining participants were recruited from the combined Birmingham, AL/Jackson, MS WIHS site (Table 1). The mean age of women was ∼50 years, with the majority of women identifying as non-Hispanic black (76% of questionnaire participants) and reporting an average yearly income of $12,000 or less (56% of questionnaire participants). Most women participating in the questionnaire (83%) reported ≥95% adherence to ART in the past 6 months, having been on ART for an average of ∼9 years.
Qualitative results: resilience among WLWH in the United States
Interviewees described various resilience strategies, including (1) intrapersonal traits and states (i.e., hardiness, acceptance, gratitude); (2) interpersonal and institutional resources (i.e., social support from multiple sources, including family, friends, other WLWH and health care providers); and (3) active engagement with spiritual and/or religious practices.
Intrapersonal traits and states
We found that many participants' individual traits (i.e., personality) and states (i.e., gratitude) were intrinsic to women's experiences of overcoming adversity associated with living with HIV.
3
Participants described their experiences of resilience in terms of having a “hardy” personality, reflecting a sense of control over one's life, a commitment to various activities and diverse relationships, and appraising difficult situations as challenges to overcome (see Table 2 for illustrative quotes).
35
Furthermore, temporary states, such as gratitude toward others, and an acceptance of one's fate, were reported within our sample. As stated by one participant,
And I think about how grateful I am that medication and research has come so far that now. It used to be you had to take 20 pills a day. And he had diarrhea and he had the vomiting and he had all that. Me, I take one pill and once in a while I have a vivid dream. Gee! I can handle that. Life isn't so bad.
(Atlanta GA, African American, Age 34)
Interpersonal and institutional resources
Gaining social support from important relationships with others (i.e., family, friends, other WLWH and health care providers) emerged as a key theme. In our study, participants explained that social support enhanced overall well-being by providing them with empowering networks and spaces to cope with multiple stressors (HIV and non-HIV related) and deal directly with challenges and adversity.
Regular contact with other WLWH offered women examples of supercopers (behaviors modeling constructive responses to a threat
36
), and inspired behavioral change within many women in our sample. As one participant stated,
Like I met one lady. She had to have been through cancer six times, but that lady looked good. It was like I had a lot of inspiration going for my treatment just to keep pushing and keep going. That's what I did.
(Atlanta GA, African American, Age 40)
Another participant described modeling resilience as motivation to both resist depressive feelings and engage in health-promoting behaviors:
So, I try to take a page out of her book and say, “This [HIV] isn't going to get me down.” I'm going to stay positive. I'm going to take my medicine. I'm going to go to my appointments the way I'm supposed to. I'm going to continue to enjoy my life.
(Jackson MS, Caucasian American, Age 51)
Encouraging and empowering other WLWH to cope constructively with adversity was central to the lives of many women in our sample. As expressed by one participant,
I do hope that maybe I can be an example to help them [other WLWH] get the courage and the strength and their self-confidence and self-worth.
(Atlanta GA, African American, Age 44)
Similarly stated by another respondent,
I think my strength helps other people to deal with their own problems.
(San Francisco CA, Caucasian American, Age 57)
Finally, health care providers also served as a positive and meaningful source of social support in our sample. As stated by a WLWH,
They [health care providers] encourage me. “You can stop drinking. You can stop. Just take your medication. Keep your doctor's appointments.”
(Birmingham AL, African American, Age 51)
Active engagement with spiritual and/or religious practices
Despite the adversity associated with living with HIV, finding meaning and purpose in life with regard to self, others, and activities through faith and spirituality was another key theme. 37 For many women, active engagement with spiritual and religious-based faith and practice offered both existential meaning and practical direction for their lives. Faith in a higher power offered tangible coping strategies to tackle concomitant life challenges. Similarly, participants described reliance on God as centrally related to various resilience strategies/approaches as evidenced by frequently expressed statements such as
Give it all to God.
(Atlanta GA, African American, Age 47)
God is not going to put any more on you than you can handle. I thank him every day.
(Jackson MS, Caucasian American, Age 56)
Women also described overcoming adversity and dealing with stressors by employing active spiritual/religious practices such as praying and meditation. One interviewee expressed,
Keep your head up and keep praying. God's got you and everything will be all right.
(Birmingham AL, African American, Age 51)
Furthermore, “finding purpose” manifested in various ways, including altruistic behaviors and kindness toward others, thereby supporting the notion that resilience operates bidirectionally: simultaneously affecting and affected by others' behavior. 38,39
Quantitative results
Based on the promising role of these resilience resources in the qualitative data, we used our quantitative data to examine how helpful these resources might be in supporting health in WLWH. The correlation coefficients among study variables are presented in Table 3.
Correlations Among Study Variables
p < 0.05, ** p < 0.01.
ART, antiretroviral therapy.
First, we assessed the relationship that resilience and depression have with viral suppression. This analysis indicated a significant interaction (i.e., moderation) effect between resilience and depressive symptoms [B = −0.04, AOR = 0.96, p = 0.01, 95% CI (0.94–0.99)]. Simple slope analyses (Fig. 1A) revealed that resiliency skills are associated with higher likelihood of viral suppression if the level of depressive symptoms is low [i.e., at 1 SD below the mean; B = 0.52, AOR = 1.68, p = 0.03, 95% CI (1.04–2.70)], but not when depressive symptoms are high [i.e., at 1 SD above the mean; B = −0.37, AOR = 0.69, p = 0.12, 95% CI (0.44–1.10)].
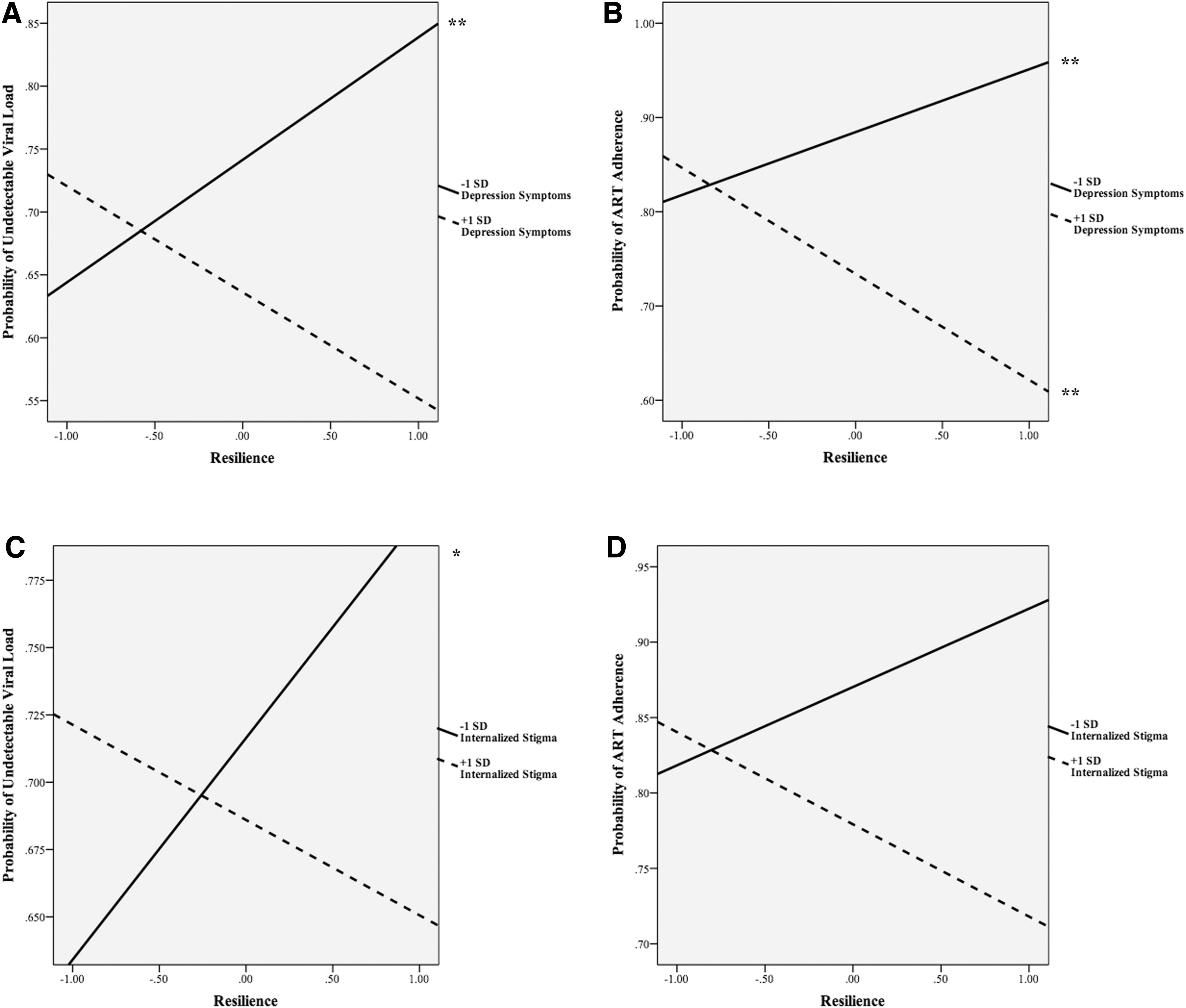
Then we assessed the relationship between resilience and ART adherence moderated by depressive symptoms. The analysis also indicated a significant interaction effect between resilience and depressive symptoms [B = −0.05, AOR = 0.95, p = 0.01, 95% CI (0.91–0.98)]. Simple slope analyses indicated that resilience is associated with optimal ART adherence at low levels of depressive symptoms [B = 0.68, AOR = 1.97, p = 0.04, 95% CI (1.03–3.77)], but with suboptimal adherence at high levels of depressive symptoms [B = −0.59, AOR = 0.56, p = 0.04, 95% CI (0.32–0.97)] (Fig. 1B).
Next, we assessed the relationship between resilience and viral suppression moderated by internalized HIV stigma. The interaction between resilience and internalized HIV stigma was marginally significant [B = −0.40, AOR = 0.67, p = 0.05, 95% CI (0.45–1.00)]. Simple slope analyses indicated that resilience is marginally associated with viral suppression at low levels of internalized HIV stigma [B = 0.41, AOR = 1.51, p = 0.05, 95% CI (1.00–2.27)], but not at high levels of internalized HIV stigma [B = −0.16, AOR = 0.85, p = 0.48, 95% CI (0.54–1.33)] (Fig. 1C).
Finally, we examined the relationship between resilience and ART adherence moderated by internalized HIV stigma. The analysis indicated a significant interaction effect between resilience and internalized HIV stigma [B = −0.58, AOR = 0.56, p = 0.03, 95% CI (0.33–0.93)]. Simple slope analyses revealed that resilience was more strongly associated with higher probability of optimal ART adherence at low levels of internalized HIV stigma [B = 0.47, AOR = 1.60, p = 0.09, 95% CI (0.93–2.74)] compared with high levels of internalized HIV stigma [B = −0.36, AOR = 0.70, p = 0.19, 95% CI (0.41–1.19)] (Fig. 1D). All coefficients and CIs of moderation analyses are presented in Table 4.
Coefficients and Confidence Intervals of Moderation Analyses
Note that 95% CIs are for odd ratios.
ADH, antiretroviral adherence; AOR, adjusted odds ratio; ART, antiretroviral therapy; CESD, Center for Epidemiological Studies Depression; CI, confidence interval; IHS, internalized HIV stigma; RES, resilience; SE, standard error; VS, viral suppression.
Discussion
Developing and implementing multi-level resilience-based strategies to improve health outcomes, particularly among individuals facing significant adversities and stressors, is a global public health priority. 40 As such, more research is needed to investigate the role of resilience in mitigating adverse health outcomes among individuals living with HIV, particularly among marginalized WLWH confronted with multiple, ongoing stressful life events. Both the qualitative and quantitative findings from this study suggest that resilience is an important resource for marginalized WLWH, fostering health-promoting behaviors (i.e., ART adherence) and leading to better health outcomes (i.e., viral suppression), particularly among women with lower levels of HIV-related stigma or depressive symptoms.
In the qualitative phase, 76 WLWH described several resilience strategies used to cope with stressors and challenges, including (1) intrapersonal traits and states (i.e., hardiness, acceptance, gratitude); (2) interpersonal and institutional resources (i.e., social support from multiple sources, including family, friends, other WLWH and health care providers); and (3) active engagement with spiritual and/or religious practices. In line with the seminal scholarship on resilience, we found that individual traits (i.e., personality) and states (i.e., hardiness, acceptance, and gratitude) were important resilience strategies for women in our sample. 25 Consistent with other qualitative studies, findings highlight that social ties to other individuals, groups, and the larger community can aid WLWH who often cope with multiple stressors (both HIV and non-HIV related), challenges, and adversities. 41,42 Relatedly, active engagement with interpersonal (i.e., friends and family) and institutional networks (i.e., health care clinics, WIHS research study, and religious institutions) engendered a sense of gratitude and thankfulness for resources and social support. A recent qualitative study by Dale and Safren similarly reports that African American WLWH as well as community stakeholders identify social support from their “village” as an important resilience resource. 17 Qualitative work by Smith et al. suggests that African American WLWH rely heavily on social support from their family members, friends/peers, and providers to overcome adversities and prioritize their health and well-being. 21
Furthermore, women in our sample expressed a deep connection to a higher power demonstrated through active engagement with spiritual and/or religious practices, which provided both intrinsic and extrinsic motivation and support to achieve optimal health and wellness. Combined, these findings suggest that the resilience-building process is a complex interlocking mechanism, calling upon intrapersonal, interpersonal, and system-level resources to promote adaptive coping. This interlocking mechanism offers material and immaterial advantages for WLWH, and can ultimately positively reconstruct HIV-related experiences as opportunities for personal change, growth, and transformation.
In quantitative analyses, significant interaction effects suggest that resilience is associated with better ART adherence and a higher probability of viral suppression, but only for WLWH reporting either low levels of internalized HIV-related stigma or low levels of depressive symptoms. For WLWH reporting high levels of internalized stigma or depressive symptoms, resilience did not predict better HIV-related outcomes. These findings suggest that resilience is an important resource for WLWH, but may lose its health protective effects at high levels of internalized HIV stigma and depressive symptoms. Bauermeister et al. report findings from a survey with young African American men who have sex with men (YBMSM), highlighting that YBMSM “who experience stigma are more vulnerable to psychological distress and may have diminished buffering through social support.” 43 Similarly, our study findings suggest that the WLWH-identified resilience resources might not be optimized without understanding and addressing the mental health needs and psychosocial stressors (i.e., internalized stigma and depression) experienced by WLWH.
Although depression is one of the most pervasive mental health disorders among PLWH and leads to adverse health outcomes, depression is underscreened, underdiagnosed, and undertreated in HIV clinical settings. 44,45 Thus, identifying the “best practices for implementing evidence-based collaborative care models for HIV-positive patients is warranted.” 46 In this context, resilience may be viewed as a coping mechanism; thus, building resilience may serve as an important strategy to address depression and stress reactions among PLWH. 47 In addition to improved screening for psychosocial burdens, optimizing resilience resources and capacity might require attention to the determinants and stressors that give rise to internalized stigma and depression. Drawing from John Metzl's notion of structural competency, 48 health care providers must be attentive to the systemic drivers (i.e., institutional, political, and economic factors) of health inequities (i.e., burden of stigma and depression) and the way in which such factors influence health behaviors (i.e., ART adherence) and outcomes (i.e., viral suppression).
Our study findings support the current shift to advance resilience-related research from a conceptual basis to concrete individual, community, and systems-level resilience strategies. 40 Earnshaw et al. 12,49 contend that individual-level strategies such as (1) creating in-group identities, (2) promoting contact with others living with HIV, and (3) enhancing social support can bolster resilience among PLWH. On a systemic and societal level, strengthening economic and community empowerment, building trust within institutions (i.e., health care), and addressing social inequities may further serve to increase resilience among PLWH. Consistent with Earnshaw et al.'s work, 49 women in our study identified a range of resilience-based strategies germane to the sociocultural context through which adversity exists. In light of the complex social, economic, and medical needs of marginalized WLWH, specialized and tailored strategies are needed to mitigate psychosocial burdens of stigma and depression so as to optimize resilience resources. This article outlines a potential conceptual development in these tailored strategies.
From an intervention perspective, we suggest a more complex and holistic approach to resilience outlined in this article, shaped primarily by our participants' testimonies to inform HIV-related health promotion programs. In light of qualitative findings, bolstering resilience in marginalized populations must occur at multiple levels and systems—ideally simultaneously. Successful resilience-building interventions should focus on (1) building or identifying latent hardiness traits (e.g., commitment to overcoming the challenges of life) while also (2) assisting clients to identify and increasingly rely on healing relationships (e.g., family members, supercopers), and encourage these clients to (3) explore the spiritual/existential dimension of the HIV experience (e.g., prayer or meditation). Quantitative findings suggest that care must be taken, however, by intervention programs to monitor psychopathology (e.g., depression) symptoms in WLWH undergoing resilience-building health interventions. Should their clients present symptoms of depression, for example, depression-focused counseling techniques and processes should be employed in conjunction with resilience-building strategies to stave off the deleterious effects of depressive symptoms on resilience in day-to-day life. Furthermore, these interventions must include social stigma theory, research, and practice to bolster the health and wellness of marginalized WLWH. Finally, we contend that an effective intervention would (1) minimize experiences of social stigma and shame, (2) assess and reduce psychopathology symptoms as they arise, and (3) locate and highlight the many potential sources of psychological resilience outlined by our participants.
This study has several limitations including the cross-sectional study design for the quantitative data collection, which prevents drawing causal conclusions, self-report measures for some variables, and time points at which data were collected or extracted. For instance, it is possible that data collected for measures of internalized stigma, depression, adherence, and resilience may have overlapped, occurred in an alternate order, or operated in a different sequence from what we hypothesized. Further, scores on the self-report scale reflect self-assessed resilience and may be biased or affected by impression management, levels of self-awareness, self-esteem, and social desirability motivations, and not lining up precisely with the actuality of experiences in dealing with stress. 50 In addition, quantitative HIV-related stigma measures used evaluated current internalized stigma, while qualitative questions explored women's experiences over time since their HIV diagnosis. Regarding the mixed-methods approach, it does appear that the two methods elucidated different processes/aspects of coping. Thus, there was relatively little convergence of qualitative and quantitative findings. As a limitation, we acknowledge the challenges of integrating two sets of very different data and their results; yet we feel that the different information derived from the qualitative and quantitative data gave us a fuller picture of women's experiences and how they affect outcomes. Finally, our distinct sample of women enrolled in the WIHS limits our ability to generalize findings to other WLWH who are not seeking care in an HIV clinic setting and/or not enrolled in a research study.
Despite limitations, this study contributes to a growing body of literature focused on resilience and HIV treatment outcomes among marginalized WLWH employing a mixed-methods design. Future research should assess the longitudinal influence of resilience on health outcomes among WLWH with varying levels of internalized stigma and depression. Further, intervention strategies should focus on mitigating stigma and depression, in addition to employing resilience-based strategies informed by the perspectives and experiences of marginalized WLWH.
Footnotes
Acknowledgments
Data in this article were collected by the Women's Interagency HIV Study, now the MACS/WIHS Combined Cohort Study (MWCCS).
Disclaimer: The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by WIHS substudy grant from the National Institute of Mental Health, R01MH104114. MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146240-01; Connie Wofsy Women's HIV Study, Northern California CRS (Bradley Aouizerat and Phyllis Tien), UAB-MS CRS (Mirjam-Colette Kempf and Deborah Konkle-Parker). The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional cofunding from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Human Genome Research Institute (NHGRI), National Institute on Aging (NIA), National Institute of Dental & Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), P30-AI-050409 (Atlanta CFAR), P30-AI-050410 (UNC CFAR), and P30-AI-027767 (UAB CFAR).